Study aim
This study aims to examine the effects of motivational interviewing for promoting ACP behaviors among palliative care patients. We hypothesized that the intervention group will exhibit significantly higher levels of readiness for ACP, lower levels of decisional conflicts regarding end-of-life care and stress, and better quality of life compared with the control group who received usual care.
Design and setting of the study
This study was a prospective, two-arm randomized controlled trial conducted at two public hospitals in Hong Kong. The participants were recruited through palliative care outpatient clinics. The ethical approval for this study was obtained from the Kowloon East Cluster Research Ethics Committee and the New Territories East Cluster Research Ethics Committee. This study adhered to the reporting guidelines of the Consolidated Standards of Reporting Trials (CONSORT).
Participants
Adult patients were eligible for the study if they had a diagnosis of a life-limiting condition and a Palliative Performance Scale (PPS) score ≥ 60% (i.e., reduced ambulation, activity, and self-care ability). PPS is a valid and reliable tool for assessing functional performance and predicting survival rates of palliative care patients. The median survival time of patients with a PPS of 60% ranged from 41 days to 65 days, regardless of diagnosis [20]. Patients were excluded if they were uncommunicable due to sensory or cognitive impairment, had language problems, were receiving active psychiatric treatment, or had advance directives or do-not-attempt cardiopulmonary resuscitation (DNACPR) order in the medical record.
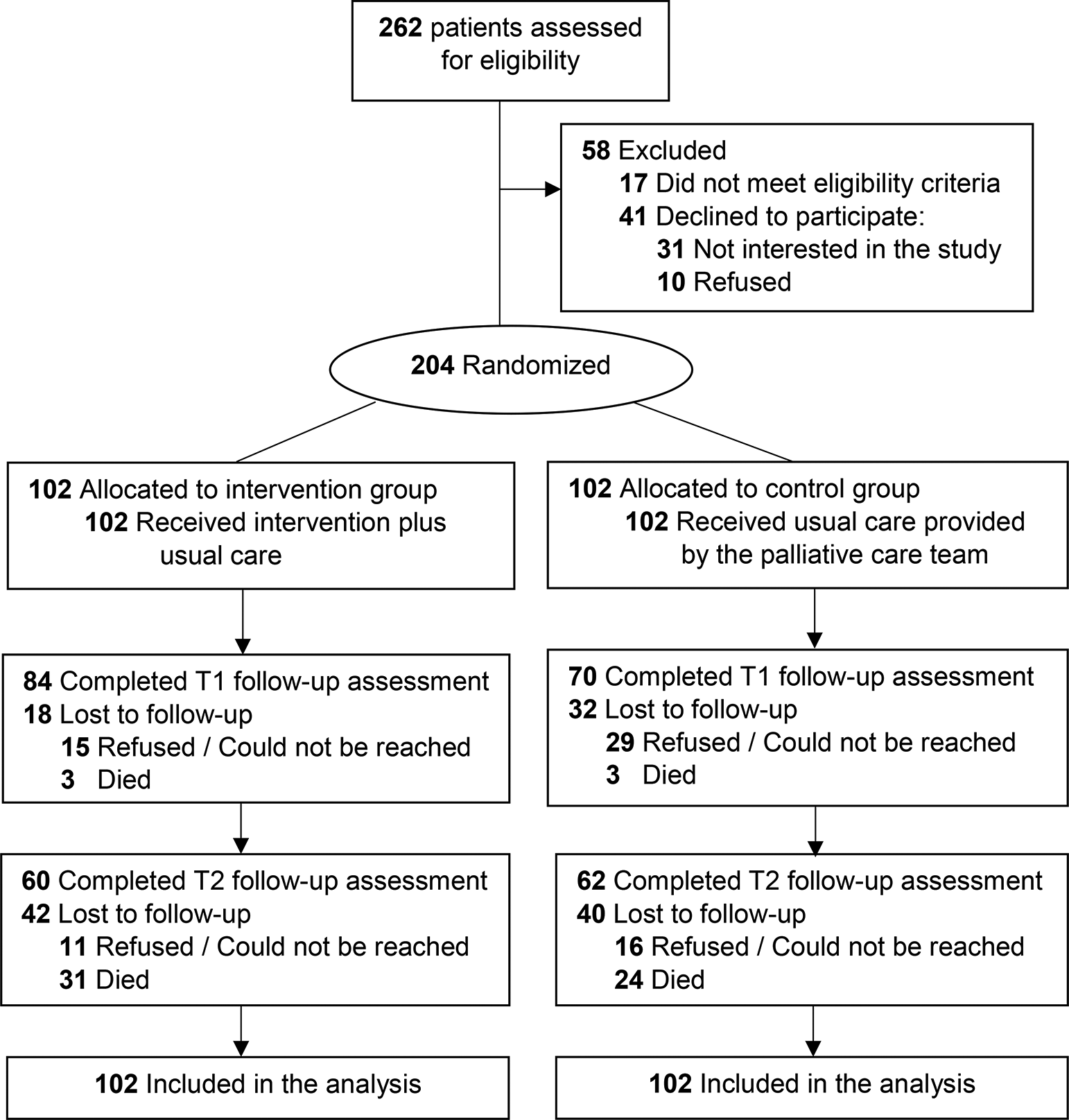
The sample size was determined based on documentation of end-of-life care decisions, which was one of the ACP behaviors, as reported in our previous study of an ACP program among Chinese patients with advanced diseases [21]. The relative risk for participants communicating their end-of-life care preferences is approximately 3.0. A total of 204 patients was needed, with 102 per arm, to achieve 80% power and detect a 20% difference between the groups by using a two-sided chi-square test at a 5% significance level and an expected attrition rate of 30% in 3 months.
Randomization and masking
A research assistant approached all newly referred patients to explain the purpose of the study and nature of the intervention and invite those who were interested to undergo eligibility screening. Consented and eligible patients were randomized in a 1:1 ratio to either the intervention group, which received motivational interviewing on planning for end-of-life care, or the control group, which received usual care, according to a randomization scheme. A statistician, who was not involved in the subject recruitment, generated a list of random numbers for group assignment and concealed the sequence using opaque sealed envelopes, which were opened by the research assistant during the group allocation process. The outcome assessor was blinded to the group assignments to avoid undue influence during the data collection process.
Study armsIntervention
The participants in the intervention group received a motivational interviewing-based ACP program on an individual basis. The intervention was adapted from an ACP grounded on narrative approach developed by the first author [21]. The three themes in the program, namely My Stories, My Views and My Wishes, were delivered through three one-hour weekly home visits within a month. Given that death-related matters are sensitive topics, building a trusting relationship between the ACP facilitator and the participants is a cornerstone for fostering in-depth discussion. Therefore, the program was designed to include repeated encounters for rapport building between the facilitator and the participants. In the first session, the participants were encouraged to share their illness experiences and beliefs about their health conditions and goals for future care. This approach allowed the facilitator to assess the individual understanding of the disease trajectory and readiness for ACP. In the subsequent two sessions, the facilitator provided tailored information to empower the participants to elicit intrinsic motivation for behavioral change. The multiple encounters highlight that ACP is a process of exploration and reflection of personal values. This enabled the participants to identify discrepancies between their preferred goal of end-of-life care and personal values, and any factors that supported or hindered their readiness to ACP. The participants’ views were recorded in a booklet for documentation. The participants could stop the discussion or withdraw from the study at any time.
The intervention protocol was reviewed by an expert panel, which included a palliative care specialist, a palliative care nurse, a social worker experienced in palliative care service, two nursing researchers who had used motivational interviewing in their research studies, a clinical psychologist experienced in delivering motivational interviewing, and a qualified trainer of motivational interviewing, to establish the content validity of the intervention. The intervention was delivered by a trained social worker experienced in using motivational interviewing. All intervention sessions were audio-recorded, with 20% randomly selected for an experienced motivational interviewing trainer to assess using the Motivational Interviewing Treatment Integrity (MITI) Coding Manual 4.2.1 revised in 2015 to ensure the treatment fidelity.
Usual care
All participants received usual care, which included a range of services offered by the palliative care teams, such as medical consultation at outpatient clinics, symptom control and psychosocial support provided by an outreach multidisciplinary team, and social or rehabilitation services offered at day care centers. All participants were provided an information leaflet explaining the concept and purpose of ACP and its potential benefits upon subject recruitment to standardize support for information needs about ACP during the study period across the two study groups.
Measures
The study outcomes were measured at three time points: baseline (T0), 1 month (T1), and 3 months (T2) following group allocation. The primary outcome was readiness for four ACP behaviors at T2. Secondary outcomes included decisional conflict, perceived stress, and quality of life.
ACP behaviors
ACP behaviors in this study included four aspects: appointing a proxy for end-of-life care decisions, discussing end-of-life care with family, discussing end-of-life care with medical doctors, and documenting end-of-life care preferences. The participants were asked to rate their readiness for these behaviors using a five-point Likert scale, with scores ranging from 1 to 5 (where a high score indicates a high level of readiness). Furthermore, the participants’ medical records were reviewed at T2 to verify whether their end-of-life care decisions were documented using advance directives or a DNACPR order.
Decisional conflict
Decisional conflict regarding end-of-life care decisions was measured using the SURE test. There were four items assessing knowledge and support received for medical decision-making, with high scores indicating less decisional conflict [22].
Perceived stress
Perceived stress was measured by the 10-item Perceived Stress Scale (PSS). It comprises four positive items about coping and six negative items about affective reactions when people are confronted with uncontrolled or overloaded conditions, with high scores indicating a high level of stress [23].
Quality of life
Perceived quality of life was measured by the 23-item modified Quality of Life Concerns in the End-of-Life Questionnaire (mQOLC-E). It covers six domains, namely, physical, food-related, emotion, social support, value of life, and existential, rated on a four-point Likert scale, with high scores indicating enhanced quality of life [24].
Data analysis
The study hypotheses were evaluated using intention-to-treat analyses, including all participants enrolled and randomized to each group. The baseline characteristics between completers and non-completers at 1 month and 3 months were compared using independent t-tests or chi-square tests. We used chi-square tests to assess the effect of the intervention and calculated the relative risk with a 95% confidence interval (CI) for the binary outcomes measured at T2. Generalized estimating equation (GEE) models were used to assess treatment effects from baseline to the follow-up assessments for continuous measures. The GEE models accounted for the dependence between repeated measures within individuals and can take into account of missing data. The interactions with each time variable of the treatment groups were assessed to examine whether the groups significantly differed with regard to changes in outcomes. Multiple imputation was used to impute missing values using chained equations in regression models that included outcome. A total of 500 imputed datasets were generated. The pooled parameter estimates from the GEE analyses and the corresponding 95% CI were calculated based on the 500 imputed datasets. The analyses were performed using SPSS version 28.0 (IBM, Armonk, NY, USA).







Comments (0)