The objective of this study was to examine the proportion of nonurgent mental health patients presenting to EDs at general hospitals throughout Germany. This is the first nationwide investigation of its kind in Germany. The findings suggest that the frequency of nonurgent psychiatric presentations in EDs could have been underestimated to date.
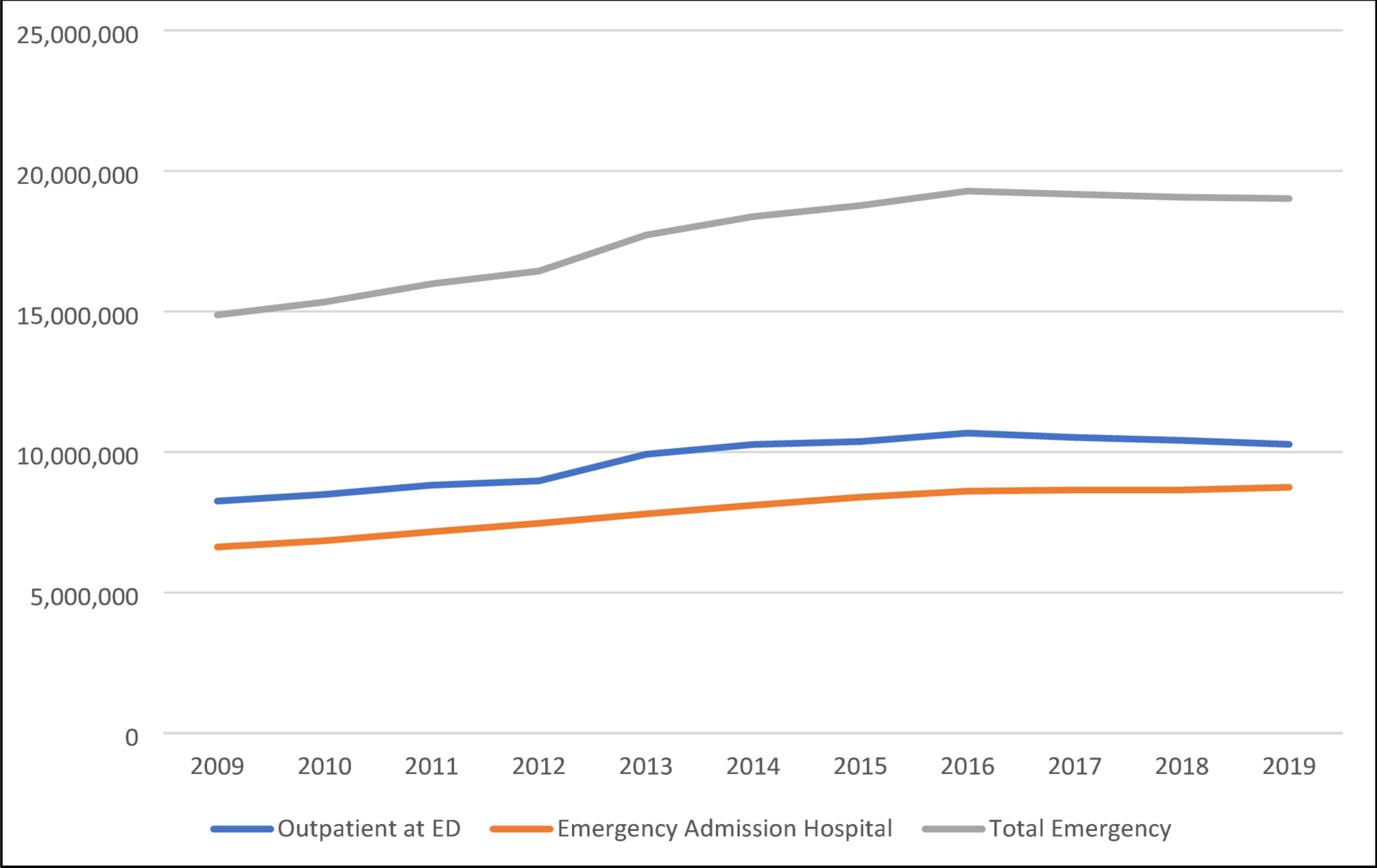
Average proportion of outpatient mental health emergency presentations among all outpatient ED visits
The continuous rise in the proportion of psychiatric presentations among all ED contacts in Germany—from 2.1% in 2012 to over 3.0% in 2021—despite a declining overall ED utilisation since 2017, highlights a growing and disproportionate demand for acute mental health services. While approximately 9.36 million outpatient ED cases (on average) and 7.66 million inpatient emergency admissions (on average) were documented annually during this period, psychiatric cases accounted for an estimated 2.58% of all outpatient ED contacts between 2012 and 2019 (239,913 cases per year on average). These trends may reflect insufficient accessibility of outpatient mental health care, evolving help-seeking behaviors, or increased psychiatric morbidity in the population [22, 23]. The stable rise in psychiatric ED utilization—despite structural reforms in emergency care and the temporary effects of the COVID-19 pandemic—emphasizes the need for integrated, diagnosis-specific approaches to acute psychiatric care, particularly in low-threshold and pre-hospital settings [24].
General trend of MHE incidences with primary and/or secondary mental health diagnosis
When examining the overall trend in outpatient psychiatric emergency patients presenting with a primary and/or secondary diagnosis at the ED of a general hospital - throughout Germany, and over the entire investigated observation period - this study identified several potential developments that must be viewed in a broader context.
Since 2012, the rate at which psychiatric patients presented to the ED increased markedly. One possible explanation is a genuine rise in the prevalence of mental health conditions. Another possible justification is that such patients are increasingly seeking care - primarily through the ED, rather than through other healthcare pathways. Presently, however, the underlying cause remains unclear since insufficient data exists to determine which factors drive this trend. A previous study by the authors (2023) suggested that up to one-fith of all psychiatric emergency visits in Germany could be nonurgent [25]. Similar trends in somatic presentations are well documented internationally [4, 26, 27] and were additionally observed across several German studies [14, 15, 28]. For example a qualitative study by Schmiedhofer et al. (2017) explored the motivations of patients with non-urgent conditions for presenting to emergency departments (EDs) in Germany [15]. The study identified several key factors influencing this behavior. Patients often cited difficulties in securing timely appointments with general practitioners or specialists, leading them to seek immediate care in EDs. The 24/7 availability of EDs provided a level of time flexibility not offered by regular outpatient services. Additionally, patients perceived EDs, particularly those in university hospitals, as offering higher-quality care and access to multidisciplinary services in a single visit. This perception contributed to a preference for EDs over traditional outpatient settings (GP respectively „Hausarzt“). The study also noted that the ease of access to EDs sometimes resulted in patients making less effort to obtain appointments in the outpatient sector. These findings suggest that EDs serve an independent role in outpatient care, and that even with improved outpatient service availability, ED utilization for non-urgent conditions may persist.
During the COVID-19 pandemic in 2020 and 2021, this study’s findings revealed a notable leveling-off, and even a decline, in ED presentations, consistent with global reports [29,30,31,32,33]. The absence of nonurgent psychiatric emergency patients, often with affective or anxiety disorders, could reflect pandemic-related factors. By 2022, however, case numbers rose again, indicating renewed ED utilization. A critical issue is that ED personnel resources have not necessarily increased at the same pace, as previously discussed by the authors [34].
Finally, the general trend of rising incidences also appeared in the 2024 study by Thom et al., which examined the prevalence of ambulatory psychiatric diagnoses in Germany during 2012–2022. The proportion of individuals with outpatient mental disorder diagnoses rose from 33.4 to 37.9%, equating to a + 13.4% increase [35]. Depression remained as the predominant diagnosis, while anxiety disorders and substance-related disorders had greater relative growth. Thom et al. examined national data across all levels of outpatient care, and found that approximately 33% of patients had a psychiatric diagnosis. The study population within this investigation represents a subgroup of these findings, focusing on emergency care, and highlighting the growing utilization of ED resources by psychiatric patients.
Specific analysis of F12.x presentations at EDs in 2019
Substance-related presentations are among the most frequent causes of psychiatric emergency contacts worldwide, with alcohol-related conditions traditionally being predominant [36, 37]. Given novel German legislation (effective April 1, 2024) and the impending legalization of cannabis, this study focused on THC-related contacts. Across the 2012–2022 period, there was an annual increase of 13.2% (p <.00001) in primary or secondary THC presentations, aligning with global data [38,39,40,41]. In a subsequent analysis restricted to 2019 THC monodiagnoses 86.9% received only a THC-related ICD-10 F12.x diagnosis, while most emergencies occurred in patients between the ages of 15 and 29 years, and dropping markedly from age 35 years or above. Although there was a trend toward higher case numbers up to age 20–24, age parameter did not significantly explain this study’s findings, contrasting several global results [38, 41, 42].The majority were younger patients, and no significant gender differences emerged, contrary to other recent studies [38, 40, 41].
Overall, this study indicate that THC-related emergency contacts primarily affect adolescents and young adults. Preventive measures should therefore be specifically targeted at these age groups. EDs thus play a key role in both public health and prevention. Whether, and to what extent, these rates will continue to rise following the legalization of cannabis remains a subject of ongoing scientific discussion [39].
Specific analysis of F32.x presentations at EDs in 2019
Affective disorders are highly relevant in EDs, particularly regarding suicidal tendencies in severe depressive syndromes [43,44,45]. According to the World Health Organization (WHO), approximately 322 million people worldwide are affected (> 4.4% of the global population), marking an 18% increase in the last decade alone [46]. Concerning Germany, the WHO estimates over four million people suffer from depression, although global data on milder depressive syndromes in ED outpatients remain scarce [25, 47]. This study therefore analyzed first-time depressive episodes (F32) presenting in the ED, assuming minimal coding imprecision.
Between 2012 and 2022, F32 diagnoses (primary and/or secondary) do not significantly explain case number trends, yet they indicate a growing burden of depressive episodes. Though this study`s results are not statistically significant, they align with other studies emphasizing the ED’s role in psychiatric presentations [2, 3, 48]. Parkmann et al. discuss “pull” factors (e.g., accessibility) and “push” factors (e.g., perceived need) that drive ED utilization [49]. Overall growth was steady, with only a slight dip around 2020, likely reflecting pandemic-related disruptions [29, 32, 33], before continuing its upward trend.
One plausible explanation is an actual increase in the prevalence of mental health conditions. Alternatively, individuals with these conditions may be increasingly opting to seek care primarily through the ED, rather than through other healthcare pathways. However, due to limited data, it remains unclear which factors are primarily driving this trend. During 2019, across 21,511 F32 cases, 7,082 (32.9%) were single F32.x diagnoses, indicating that approximately 33% were primarily depressive episodes. Most occurred in younger adults, peaking at ages 20–24, whilethe 15–34-year age group comprised ~ 65% of cases, aligning with previous studies [46,47,48]. These elevated incidence rates could reflect social stressors, life transitions, or increased mental health awareness [50,51,52]. Beyond the age of 25 years, case numbers dropped, potentially suggesting under-diagnosis or competing health concerns. Females predominated males in case incidences by over 23%—though without statistical significance, consequently contradicting broader literature pointing to such higher female prevalence [52, 53].
Specific analysis of F41.x presentations at EDs in 2019
Anxiety disorders significantly impact both routine outpatient care and emergency services, with 4.4% of the global population affected in 2021 [54]. In Germany, 4.74% of the population had a one-year prevalence of anxiety disorders in 2022, while Thom et al. (2024) reported 6.7% in outpatient settings—placing anxiety disorders third among mental illnesses, after affective and substance use disorders [35]. These findings underscore a growing burden on healthcare systems, yet research on nonurgent anxiety ED patients remains scarce. One study from this group [55] aligns with Thom (2024), confirming F41.x among the top three outpatient mental disorders [35]. In this goup´s sample, F41.x was most prevalent, surpassing F12.x and F32.x. Notably, in 2019, across 38,713 patients being studied, 38% with an F41.x diagnosis presented with a monodiagnosis, reflecting earlier work by Marchesi and Biancosino [47, 56]. A statistically significant 5.7% annual growth in F41.x cases from 2012 to 2022 underscores the need for targeted prevention and effective treatments. Contrasting to Thom et al. [35], EDs in Germany appear to be a primary access point for anxiety disorders, which aligns with this goup´s 2023 results [25].
This study´s data also demonstrated that emergency cases typically peak among younger adults (up to 24 years) prior to declining with age. Adolescents (15–19 years of age) presented a marked increase, echoing Boyer et al. and Benarous et al. [57, 58] investigations on heightened risk during transitional phases. The ED may thus serve as a first point of contact for anxiety or panic attacks. Regarding gender distribution, 5,682 males (in comparison to 8,870 females) aligns with broader global trends. Overall, these latest underscores the ED’s crucial role in acute care and secondary prevention for individuals with anxiety, especially those seeking help for the first time.
Various causes for the increase in nonurgent emergency contacts are described in the literature, some of which are also transferable to mental health patients. Many of the factors discussed are also considered possible starting points for countermeasures.
The only study in Germany to date examing the nonurgent mental health presentation at the ED addressing this issue, highlights an insufficient availability of outpatient psychiatric services [25]. In the catchment area of the ED examined, only a few psychiatric practices were available for approximately 250,000 to 300,000 inhabitants. One proposed solution was a coordinated system of open consultation hours across existing practices, without the need for appointments, to improve access for individuals experiencing mental health crises.
Targeted public education to enhance mental health literacy—such as clarifying what constitutes a psychiatric emergency—also appears beneficial. This could take the form of awareness campaigns, similar to previous initiatives focused on depression and suicidal behavior [59].
In addition to expanding low-threshold services and increasing public awareness, improved coordination within the regional healthcare system may offer further benefits. Strengthening the gatekeeping role of general practitioners, combined with clear pathways between emergency departments, specialist clinics, and outpatient providers, would be a crucial element in this effort.
Limitations
This study provides, for the first time, a nationwide overview of ambulatory psychiatric ED patient cases, over a 10-year observation period. The use of billing codes (Notfallziffer) allowed for clear identification of ED contacts. However, uncertainties arose from its retrospective design, particularly regarding the classification of primary and/or secondary diagnoses, which did not always allow for unambiguous determination of the main reason for ED presentation. Emergency contacts without subsequent inpatient admission were classified as outpatient cases and, based on this operational definition, were assumed not to meet the criteria of a psychiatric emergency. As no individual case validation was conducted, this approach constitutes an approximation and should be interpreted within the limitations of aggregate data analysis. To enhance diagnostic specificity, the authors conducted a more detailed analysis of individual diagnoses. Although only a subset of patients with the three primary diagnoses (F12.x, F32.x, and F41.x) were captured with data on age and gender, the authors firmly believe such findings still provide meaningful insights. Furthermore, coding practices could have varied across institutions and over time, potentially impacting the accuracy of both primary and secondary diagnoses. This study was also unable to account for factors such as comorbidity severity, which could influence presentation patterns. Lastly, gathered data did not capture broader sociodemographic variables that could further elucidate the context of psychiatric emergencies in this setting. Furthermore, only patients with statutory health insurance were included on a nationwide level. Patients with private health insurance could not be included. In addition, no comparison was performed against standard (or routine) care, so it remains uncertain whether the observed increase reflects a higher prevalence rate, or an actual rise in service utilization.


Comments (0)