A growing body of evidence clearly indicates the detrimental impact of low-grade inflammation on the cardiovascular system. Over the past two decades, extensive clinical and experimental research has unequivocally demonstrated that atherosclerosis represents a low-grade, sterile, inflammatory disease. Both systemic and localized inflammation play pivotal and indisputable roles in the genesis and progression of cardiovascular disease, spanning from endothelial dysfunction to full clinical syndrome [1].
Juvenile idiopathic arthritis is an important model of inflammation, where the impact of inflammation on vascular and myocardial functions can be studied.
Vlahos and colleagues reported that vascular function is impaired in patients with JIA [2], in addition to an increase in intima media thickness. The latter is more prominent in systemic-onset juvenile idiopathic arthritis (SO-JIA) and is correlated with inflammatory markers and adhesion molecules, which are upregulated in patients with JIA [3].
Despite the extensive research that has explored either macro- or microvascular functions and subclinical myocardial involvement in JIA, it is still unclear whether myocardial dysfunction in this inflammatory disorder is affected by microvascular dysfunction [4].
Strain or speckle tracking imaging allows segmentation of the myocardial tissue and detection and quantification of segmental motion. The latter can be achieved in longitudinal or circumferential planes, Global longitudinal strain is the average strain of all segments of the left ventricle and has slowly evolved to become an important measure of LV contractility in systemic disorders and in the context of follow-up of the effect of cardiotoxic medications. Detecting aortic relaxibility is an indirect measure of elasticity and vascular dysfunction. Using the STE circumferential software to quantify circumferential aortic motion has also been proposed as a good measure of vascular dysfunction [5].
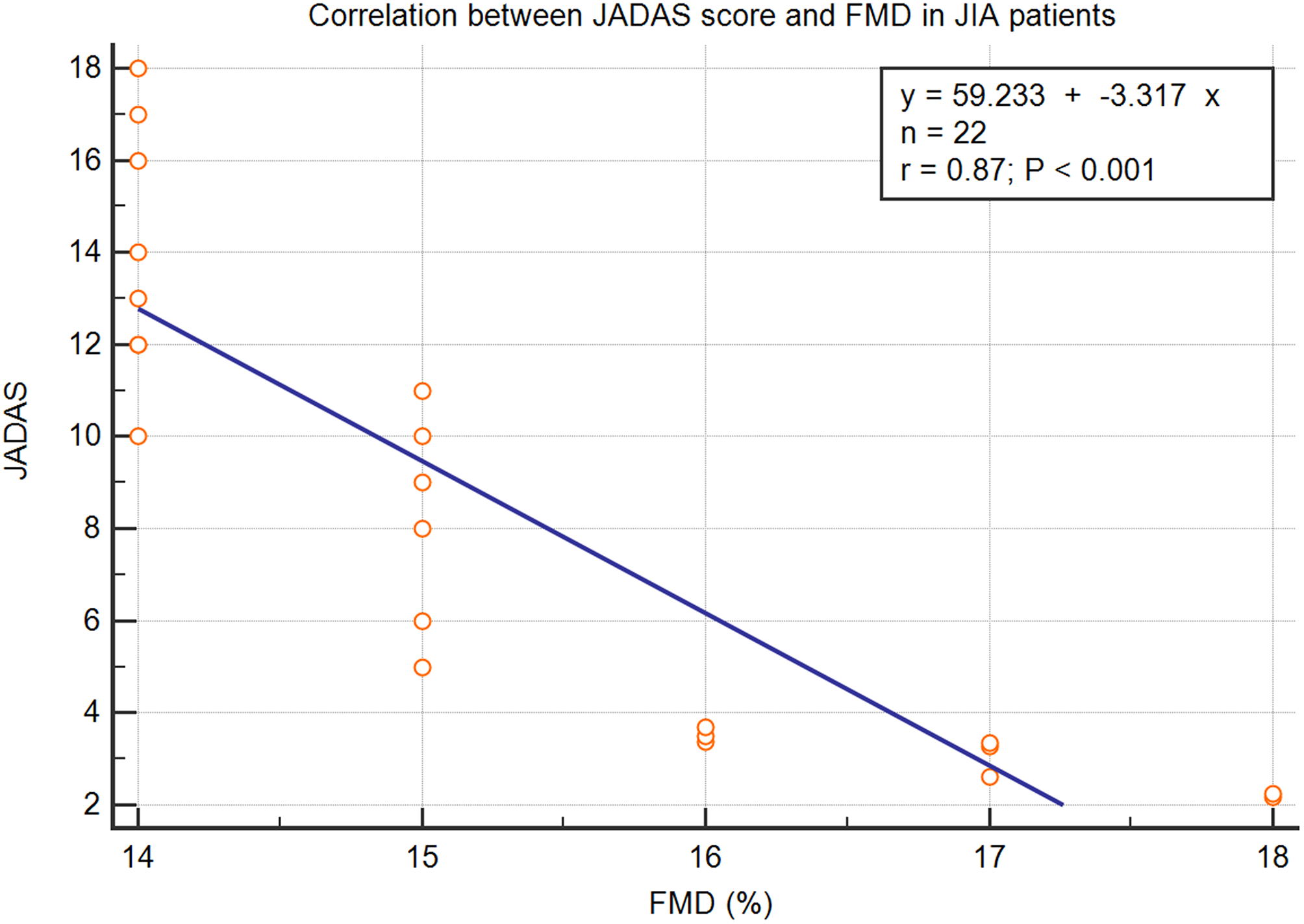
The primary role of large arteries is to reduce the transmission of pulsatility associated with the heart’s contractions by elastic recoil following systolic expansion. This process ensures a steady, rather than a pulsating, blood flow to various organs and tissues, including the coronary arteries. However, this buffering function diminishes as the aorta and its major branches become stiffer, as a result, the pulsatile energy is transmitted to the fragile microvascular vessels in the downstream organs and tissues. Damage to these microvessels can disrupt blood flow and trigger local inflammatory responses, ultimately harming organ function and raising vascular resistance over time. Thus, vascular stiffness is regarded as the first trigger of microvascular dysfunction. This is why it is important to measure aortic relaxibility via circumferential strain, and to correlate it with FMD as an established measure of vascular stiffness [6].
This study aimed to explore this phenomenon by testing vascular function via aortic strain and its relationship with myocardial function in a cohort of pediatric JIA patients.





Comments (0)