Neonatal septicemia is a common and potentially life-threatening clinical syndrome, which is characterized by systemic inflammatory reaction and the presence of pathogens in blood stream. Newborns are vulnerable to sepsis because their immune system is not fully mature and their resistance to various infectious pathogens is weak. Clinically, early identification and treatment of neonatal sepsis is very important, because delayed treatment will quickly lead to organ failure and death. PTEN and TLR4 are two key molecules in the pathological mechanism of neonatal sepsis. PTEN is a multifunctional enzyme, which not only regulates cell growth, division and survival, but also regulates immune and inflammatory reactions [7, 8]. TLR4 is a pattern recognition receptor in the immune system, and its main function is to recognize pathogens and activate the host’s natural immune response. In sepsis, TLR4 recognizes the specific molecular pattern of pathogens, triggering a series of signal transduction events, leading to the production and release of inflammatory factors [9, 10]. Therefore, the expression levels of PTEN and TLR4 in serum may reflect the biological state and immune response of neonatal sepsis. Monitoring the level of these markers is not only helpful to evaluate the severity of the disease, but also may provide important information for predicting the clinical outcome.
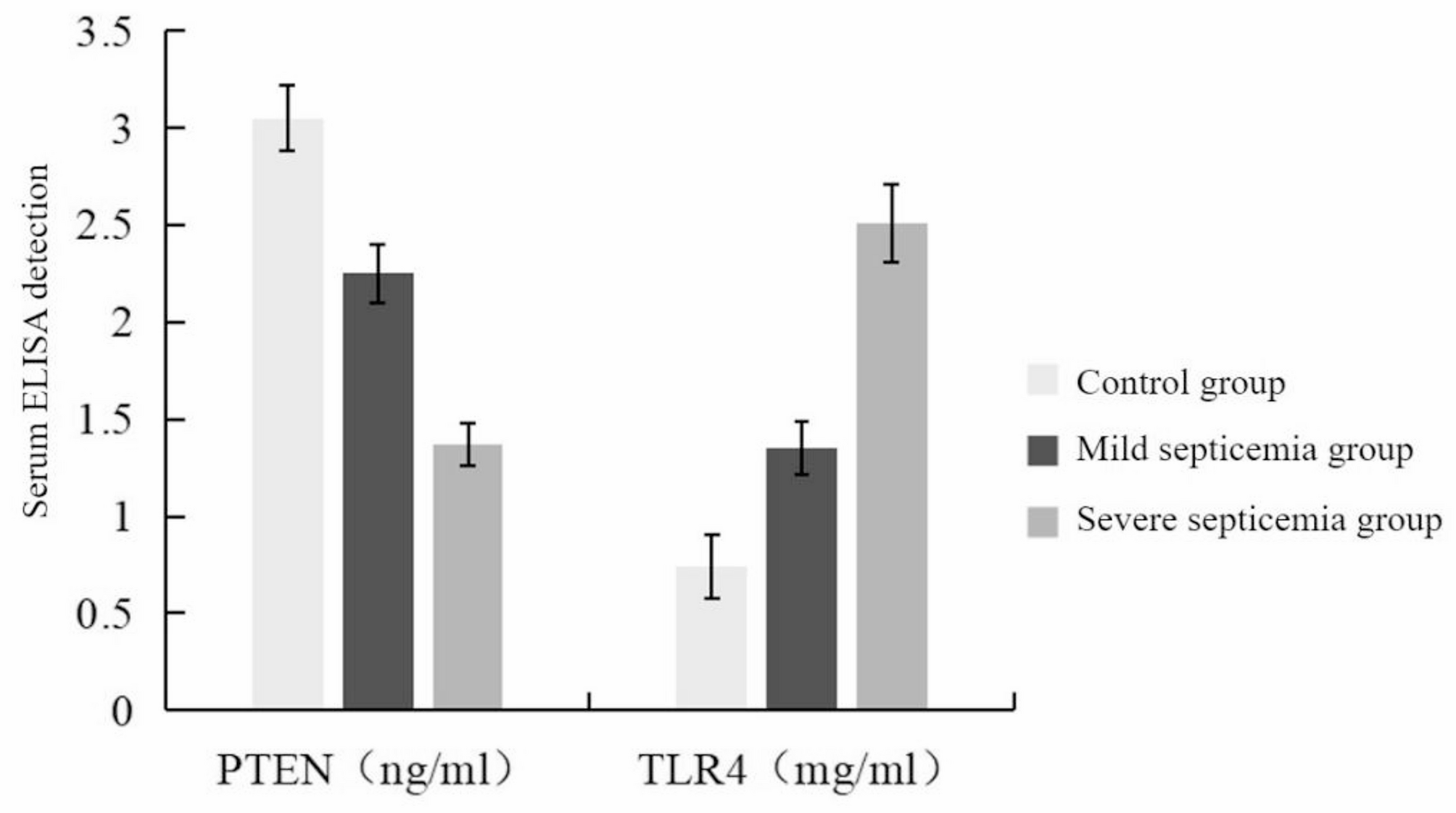
In this study, we deeply discussed the relationship between the expression levels of serum PTEN and TLR4 and the severity and prognosis of neonatal sepsis. It was found that the inflammatory indexes PCT, CRP, HBP and WBC were higher in newborns with severe and mild sepsis than control group, which was consistent with the traditional view that these indexes could reflect the inflammatory state of neonatal sepsis. PTEN and TLR4 have different expression patterns in neonatal sepsis. The significant decrease of PTEN in newborns with severe and mild sepsis suggests that PTEN may play a protective role in cell response to inflammation. PTEN usually plays an important role in cell proliferation, survival, and signal regulation. Especially in the PI3K/Akt pathway, it can regulate the cell’s response to external signals, and the weakening of PTEN activity may cause its overactivation, leading to immune system overreaction and subsequent tissue damage [11, 12]. This imbalance of immune response may be particularly significant in severely ill newborns, because they are more prone to serious inflammation and organ dysfunction. Compared with the down-regulation of PTEN, the up-regulation of TLR4 provides insights on how the body recognizes and responds to septicemia pathogens. The rise of TLR4 indicates the activation of the host immune system and the enhancement of pathogen recognition ability, which is a natural defense response aimed at eliminating invasive pathogens [13,14,15]. However, the over-activation of TLR4 signal may also aggravate inflammation and lead to immunopathological damage, thus worsening the severity of the disease.
In newborns suffering from neonatal septicemia, there is a certain correlation between the significant decrease of serum PTEN level and the increase of TLR4 level and mortality. These results may provide important biological information for clinicians, and help them to evaluate the disease risk of newborns more accurately, so as to formulate more effective intervention measures [16, 17]. For example, in the early stage of neonatal sepsis, if the level of PTEN is decreased and the level of TLR4 is increased, the doctor may predict that the condition may deteriorate and adjust the treatment strategies accordingly, such as strengthening monitoring, using immunomodulatory drugs early or carrying out life support treatment in time. Similarly, the increase of traditional inflammatory indexes such as PCT, CRP, HBP and WBC also reflects the existence of systemic inflammation, which go space the poor prognosis of neonatal septicemia patients. Their levels may reflect the severity of infection and the strength of the body’s response to infection to some extent [18,19,20]. Although these traditional indicators are helpful for the initial evaluation of diseases, the combination of new biomarkers such as PTEN and TLR4 may be more refined for the evaluation of diseases, and it is expected to provide more comprehensive information for clinical decision-making. Through the joint evaluation of these markers, we can understand the immune status and pathological process of neonatal septicemia more comprehensively, thus promoting the implementation of personalized medicine.
Pearson correlation analysis revealed that PTEN was negatively correlated with inflammatory markers, while TLR4 was positively correlated. These findings provided powerful clues for us to understand the role of these two molecules in the inflammatory process [21, 22]. ROC curve analysis provides quantitative evaluation for the diagnostic value of PTEN and TLR4. The AUC value of both of them is much higher than that of traditional inflammatory markers, which suggests that they may play a key effect in the early identification of neonatal sepsis and the monitoring of disease progress. The high AUC value of PTEN may represent its protective role in prognosis, while the high AUC value of TLR4 may indicate the severity and progress speed of the disease. Clinically, this discovery may help to develop new diagnostic tools, so that doctors can identify high-risk newborns earlier through the changes of serum markers, so as to take corresponding intervention measures.
This suggests that evidence-based strategies can be developed based on serum PTEN and TLR4 expression levels in newborns with severe sepsis. From this, it can be concluded that a three-level evidence-based management strategy is proposed for critically ill LOS newborns. Level 1 (upon admission): Immediately test for PTEN/TLR4. When PTEN < 1.37 ng/mL and TLR4 > 2.51 mg/mL, it suggests that the SOFA score may rapidly deteriorate and should be transferred to the NICU for combined use of antibiotics and immunomodulators [23, 24]. Level 2 (treatment monitoring): PTEN should be rechecked every 24–48 h. If it does not recover to > 1.5 ng/mL within 72 h, it is considered that there are drug-resistant bacteria or fungal infections, and the antibacterial spectrum needs to be expanded [25]. Level 3 (prognostic evaluation): newborns with TLR4 > 2.8 mg/mL on the 5th day had a mortality rate of 75% (the mean of the death group in this study was 2.86 ± 0.20), and potential adverse outcomes should be communicated with family members in advance [26]. According to the expression levels of PTEN and TLR4 and the results of bacterial culture and drug sensitivity test, appropriate antibiotics were selected for treatment.




Comments (0)