
Remember me

Despite advances in the diagnosis and treatment, infective endocarditis (IE) remains a major public health challenge [1]. Strategies for prevention are important to reduce mortality and morbidity, but the outcome of infective endocarditis depends mainly on timely recognition and appropriate treatment. Accurate, prompt diagnosis often proves difficult because of the diverse clinical manifestations [2, 3]. Echocardiography is the first-line imagining modality in patients with suspected IE which can detect the presence of IE as well as assess the functional and structural damage to cardiac structures [2, 4]. Its findings have prognostic implications and help with the decision-making process regarding medical or surgical treatment [2,3,4,5]. Echocardiography may be normal or inconclusive in up to 30%, [5] particularly when there is prosthetic material present or in cases of complex congenital heart defects [6, 7].
Other imaging modalities, such as nuclear imaging, computed tomography (CT), and magnetic resonance imaging (MRI) have been shown to be complementary in demonstrating valve involvement as well as endocarditis on distal structures [8,9,10]. A multimodality imaging approach was introduced in 2015 and modified in the current ESC guidelines and in the modified Duke criteria [1, 11].
We aim to describe the use of multimodality cardiac imaging in the diagnosis of infective endocarditis with specific reference to transthoracic and transoesophageal echocardiography, cardiac computed tomography, cardiac positron emission tomography and cardiac magnetic resonance imaging, using several cases from our institution to illustrate the complimentary role of each modality.
Prevention: clinician and patient educationThe high risk of adverse events associated with IE makes it critical to optimize preventive strategies. Clinicians should identify patients at elevated risk. Current guidelines indicate that patients with previous IE, prosthetic heart valves or with any material used for cardiac valve repair or congenital heart disease (CHD) are at increased risk of IE. Patients with rheumatic and non-rheumatic heart valve disease, CHD with isolated valvulopathy, cardiac intravenous electronic devices (CIED) and hypertrophic cardiomyopathy, instead, are considered at intermediate risk. Additional extracardiac factors, such as extremes of age and immunocompromised states, may increase predisposition to IE [1].
Healthcare providers should provide individuals at the highest risk with personalized infection prevention counselling and support. Patient education is the cornerstone of prevention [12]. The relevance of professional regular oral care and attentiveness to skin hygiene (i.e. wound care) should be highlighted. Those at intermediate and high risk should be discouraged from getting tattoos and piercings [1]. Most importantly, patients should be educated about IE signs and symptoms and advised to seek urgent medical attention and early antimicrobial therapy in case of possible or confirmed infection [1,2,3].
Appropriate risk stratification is recommended but remains challenging. It has been widely demonstrated that unregulated antibiotic prescription leads to the development of multi-resistant bacterial species which are difficult to eradicate. [13] Antibiotics have side effects and can have serious adverse effects for individuals, such as anaphylaxis. At present, antibiotic prophylaxis is recommended by the ESC in patients considered at high-risk of endocarditis (as outlined above) in patients undergoing ‘at risk’ dental procedures including dental extractions, oral surgery or procedures requiring manipulation of the gingival or periapical region of the teeth [1]. The recommendations from the American Heart Association and American Dental Association are very similar [14]. Whilst recommendations and guidelines may vary, prophylaxis may also be considered in intermediate risk individuals and an individualized assessment is advised [1]. Prophylaxis may be considered in high-risk patients undergoing invasive procedures of the respiratory, gastrointestinal, genitourinary, skin, or musculoskeletal systems [1]. For cardiac procedures, pre-operative screening for nasal carriage of Staphylococcus Aureus and subsequent treatment is recommended before elective cardiac surgery or transcatheter valve implantation [15]. Exclusion of potential sources of sepsis should be considered two weeks prior to cardiac procedures where possible (i.e. in elective cases). Peri-operative antibiotic prophylaxis and optimal pre-procedural aseptic measures are recommended before CIED implantation, surgical or transcatheter implantation of a prosthetic valve or other foreign material [16,17,18]. Prompt therapy with organism sensitive antimicrobial pharmacotherapy should be prescribed for any clinically apparent infection [1].
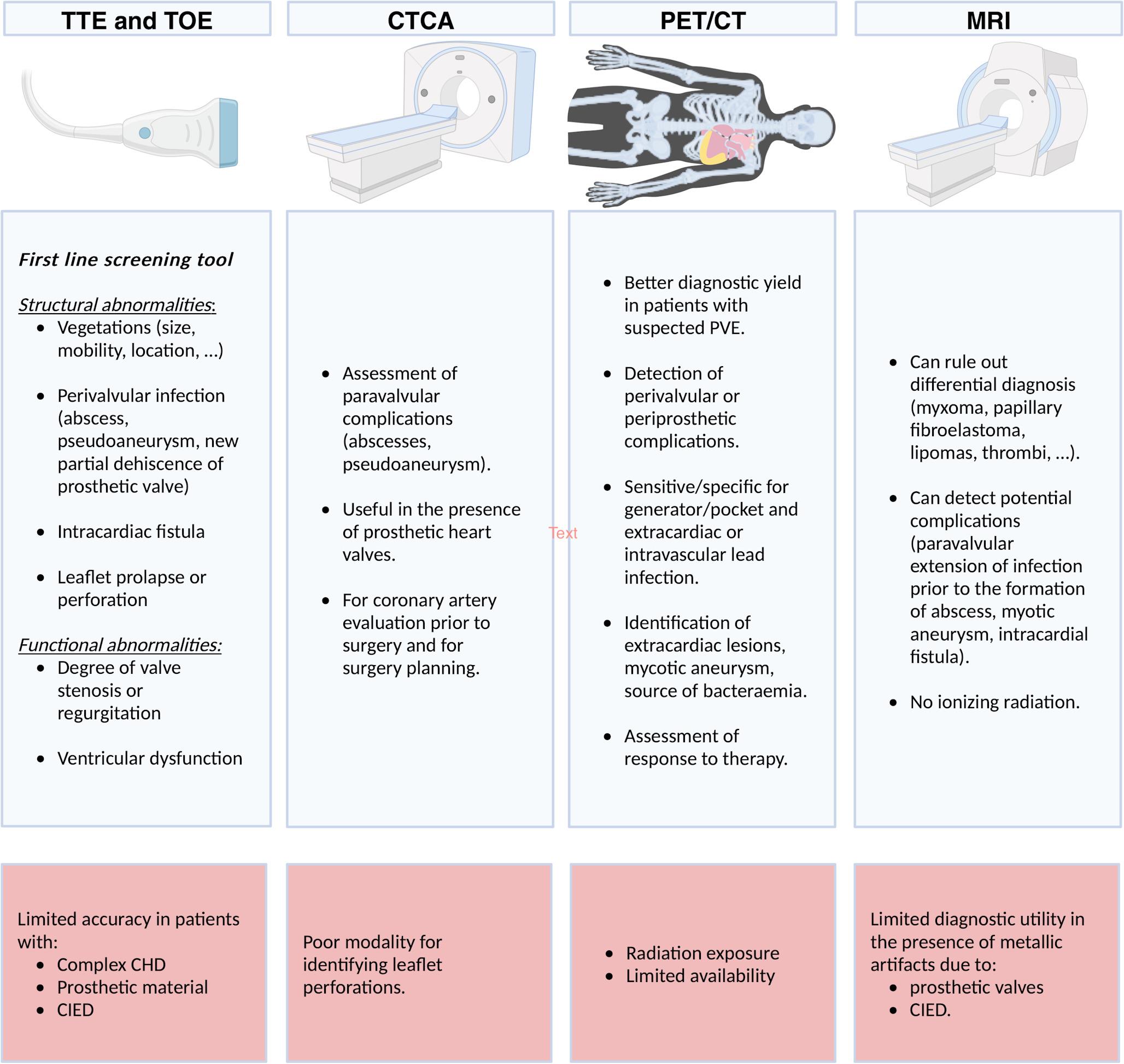
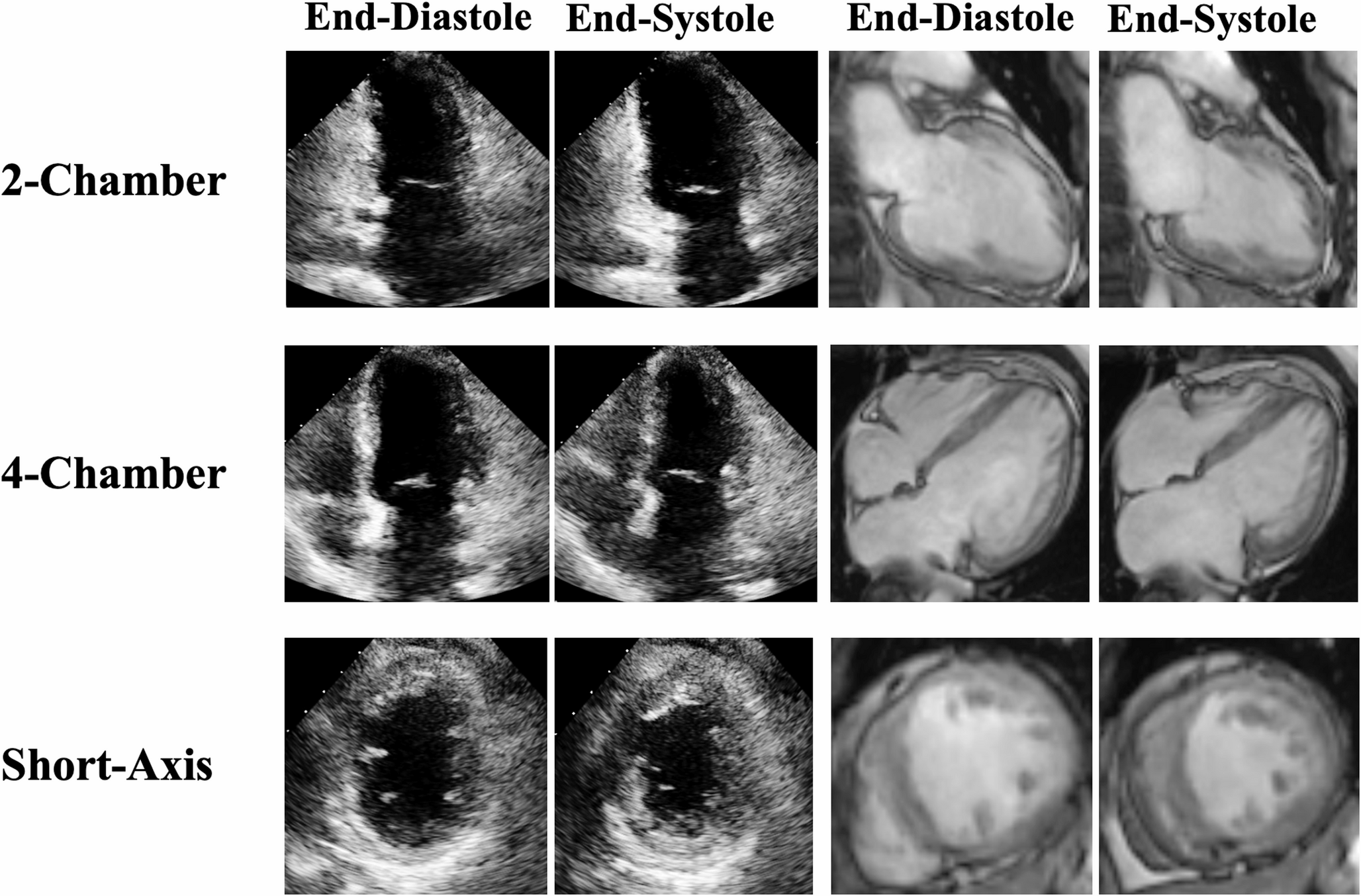
EchocardiographyEchocardiography is the pivotal imaging modality in diagnosing suspected IE and should be performed as a first-line screening tool [1]. Echocardiography can assess structural cardiac abnormalities, such as; the presence, number, size, shape, location, echogenicity, and mobility of vegetations. Echocardiography can assess for perivalvular infection (abscess, pseudoaneurysm, new or partial dehiscence of a prosthetic valve), intracardiac fistulae and leaflet prolapse or perforation. Echocardiography can assess for functional abnormalities; the presence and severity of native or prosthetic valve stenosis or regurgitation and ventricular dysfunction [19].
The initial assessment of patients with suspected IE is performed with transthoracic echocardiography (TTE) [20] (Fig. 5A and Fig. 7). Its sensitivity to detect vegetations on native valves is about 70%, but drops to 50% in prosthetic valves due to the acoustic shadowing of artificial leaflets [4]. In the early postoperative period, the presence of perivalvular haematoma and oedema may also lead to misinterpretations. TTE is limited in the assessment of perivalvular complications. The sensitivity of TTE for diagnosing abscesses is 30–50%, which increases to 80–90% with transesophageal echocardiography (TOE) [20, 21]. Abscesses are more frequent on prosthetic than native valves and in the aortic than the mitral position. TTE has limited sensitivity (about 25%) to detect small vegetations (< 5 mm) or vegetations associated with intracardiac devices [22].
Fig. 1
70-year-old female with prior surgical aortic valve replacement, presenting with acute limb ischemia and Pseudomonas Aeruginosa bacteremia, raising concern for possible infective endocarditis. Figure 1: top panel: transesophageal echocardiogram images with an echodensity on the aortic valve (arrow) suspicious for a vegetation, though the assessment was limited by artifacts. The bottom panel: gated cardiac CT imaging, clearly visualizing the vegetation (arrow). CT ruled out aortic root abscess or paravalvular infection. The patient was treated with appropriate antibiotics for infective endocarditis. This case underscores the utility of CT in clarifying equivocal echocardiographic findings in endocarditis management
Fig. 2
Images of a 44-year-old gentleman with a history of valve-sparing aortic root replacement for an aneurysmal aortic root approximately 9 years ago, followed by mechanical aortic valve replacement (AVR) 5 years later. He presented with heart failure, and his transthoracic echocardiogram revealed severe paravalvular aortic regurgitation. Transesophageal echocardiogram confirmed severe paravalvular regurgitation and valve dehiscence. A subsequent CT coronary angiogram confirmed valve dehiscence and an aortic root abscess which was culture negative. Top panel: transesophageal echocardiogram images depicting valve dehiscence and severe paravalvular aortic regurgitation (arrow). Bottom panel: CT demonstrating valve dehiscence and the aortic root abscess (arrow). The patient was referred for surgery
The 2023 European Society of Cardiology (ESC) Guidelines on IE recommend TOE in all patients with suspected IE, due to its higher sensitivity (about 90%) in detecting vegetations and evaluating perivalvular complications (Figs. 1, 2, 3, 4A and 6) relative to transthoracic echocardiography. This recommendation includes those patients with a TTE suggestive of IE, apart from isolated right-sided native valve IE where a good quality and conclusive TTE has been performed [1]. TTE in right sided native valve IE, often provides comprehensive assessment due to the anterior position of the right heart, but sometimes it is necessary to use non-standard echocardiographic views to visualize the right ventricular inflow and outflow tract (Fig. 7), Eustachian valve and posterior leaflet of tricuspid valve [23].
Fig. 3
67-year-old gentleman presenting with a 4-day history of malaise, fatigue, and fevers. History of 25 mm Mosaic tissue aortic valve replacement 6 years prior to this presentation. Blood cultures were positive for Methicillin-Sensitive Staphylococcus Aureus (MSSA). Transthoracic echocardiogram revealed thickened valve leaflets and abnormal thickening along the posterior aortic root with an echolucent space, suspicious for an aortic root abscess. These findings were confirmed on CT coronary angiogram, which also showed significant thickening of the aortic root, particularly at the non-coronary and left coronary cusp positions. The patient was referred for surgery, during which frank pus was drained from beneath the non-coronary cusp. The top panel (A, B, C) shows transesophageal echocardiogram findings suspicious for an aortic root abscess with thickened aortic valve leaflets. The bottom panel shows CT coronary angiogram images demonstrating aortic root thickening consistent with the abscess
Fig. 4
45-year-old female who initially presented with Enterococcus faecalis native valve endocarditis, severe aortic regurgitation, and acute heart failure. She underwent emergent mechanical aortic valve replacement (19 mm) and ventricular septal defect (VSD) repair with a bovine pericardial patch. Approximately 6 months later, routine echocardiography (Fig. 4A) revealed abnormal flow and a paravalvular space with communication from the aortic root to the pulmonary artery, raising suspicion for a fistula. CT coronary angiography (Fig. 4B) confirmed an aortic root pseudoaneurysm, which communicated with both the pulmonary artery and the left ventricular outflow tract (LVOT). The patient was referred for re-do surgery. This case highlights the incremental value of CT coronary angiography in identifying aortic root pseudoaneurysm. The pseudoaneurysm was possibly due to reinfection, although the patient was culture-negative at the time of representation
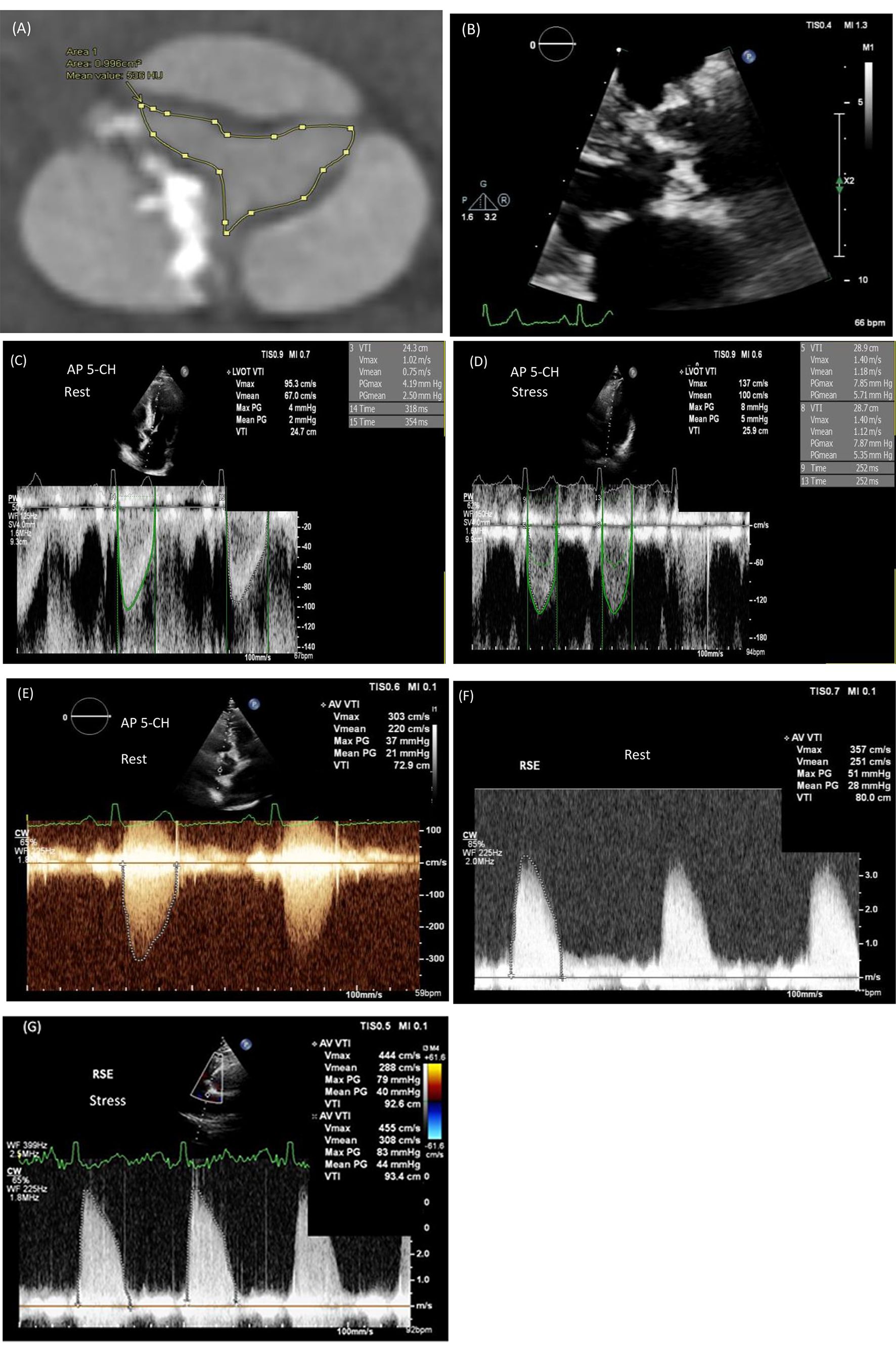
Fig. 5
63-year-old gentleman with prior mechanical aortic valve replacement and a supra-coronary ascending aortic graft five years prior, presenting with Methicillin-Sensitive Staphylococcus Aureus (MSSA) bacteremia and suspected mechanical aortic valve endocarditis. Transthoracic echocardiogram revealed no vegetation but did show an echolucent space around the ascending aorta graft. Transesophageal echocardiogram could not be performed due to grade D esophagitis and ulcers. The patient was also found to have multifocal cerebritis and small cerebral abscesses on CT brain imaging. A subsequent CT cardiac angiogram revealed a perigraft collection around the ascending aorta graft with two small pseudoaneurysms at the site of the anastomosis between the native aortic root and the supra-coronary ascending aorta graft junction, correlating with the echolucent space seen on echocardiography. FDG-PET imaging confirmed infection with FDG uptake around the graft. Figure 5A shows a side-by-side comparison of the perigraft echolucent space on standard echocardiography, echocardiography with Definity contrast, and CT coronary angiogram (A, B, and C, respectively). Figure 5B reveals the ascending aorta pseudoaneurysm and perigraft collection in both short-axis and long-axis images, as well as FDG uptake on PET imaging in this region. The patient was referred for surgery
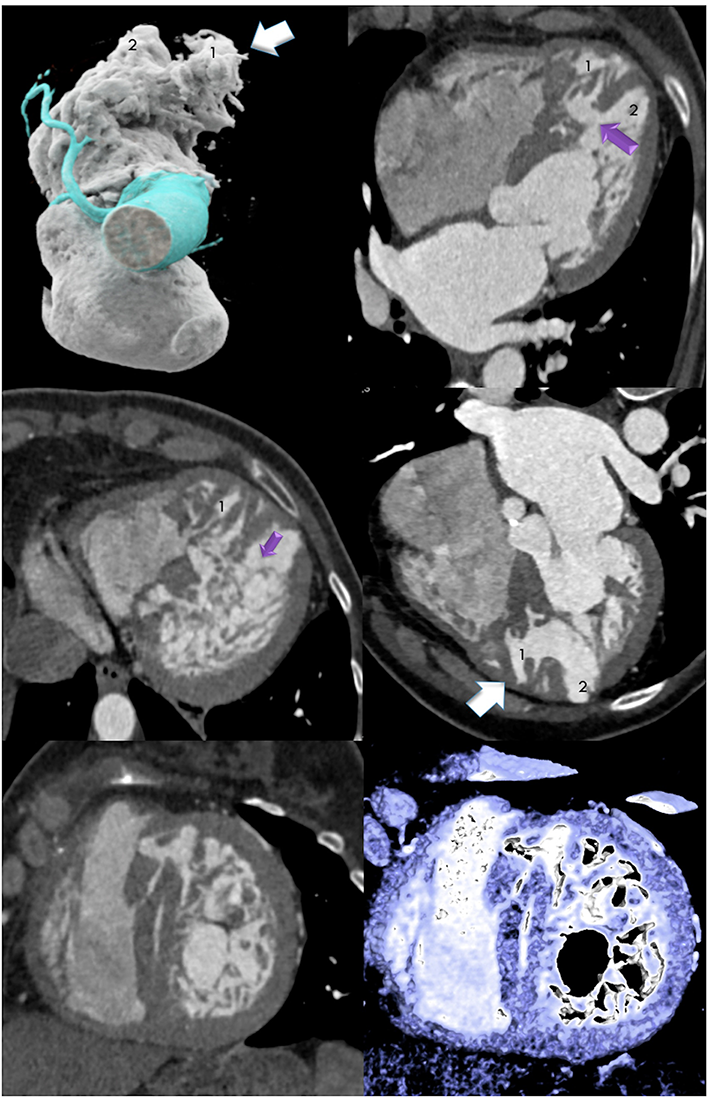
Fig. 6
61-year-old gentleman presenting with subacute infective endocarditis. He had a three-week history of night sweats, chills, and rigors, along with a three-to-six-month history of exertional dyspnea and chest tightness. Transesophageal echocardiogram revealed thickening of the aortic valve, mobile vegetations, and moderate aortic regurgitation. A CT coronary angiogram, performed as part of his surgical workup, confirmed thickening of the aortic valve leaflets, a central coaptation defect. Panel A shows an abnormal echodensity attached to the aortic valve. Panel B shows the aortic regurgitation jet on long-axis images of the transesophageal echocardiogram. Panel C shows the filamentous density attached to the thickened aortic valve on CT. Panel D reveals the thickened bicuspid aortic valve with a raphe between the left and right coronary cusps and central malcoaptation as the site of the patient's aortic regurgitation
Evaluation with the combination of both TTE and TOE was superior in identifying morphological valve abnormalities, septum defects, and fistula formation compared to other imaging modalities in 46 patients with suspected IE. In addition, echocardiography provides a reliable assessment of ventricular function [24]. Echocardiographic evaluation of vegetation size and mobility is important to predict embolic events and guide the indication and timing of surgery, as well as follow-up during the peri-operative and post-operative period. Several conditions, such as papillary fibroelastoma, myxomatous mitral valve disease or thrombus may be mistaken for a vegetation when assessed with echocardiography (Fig. 7). TOE is the gold standard for vegetation detection and measurement of its length, with 2D-TOE limited in selecting the true maximal dimensions. Real-time three-dimensional TOE (RT3D-TOE) allows for a thorough analysis of vegetation size and morphology and assessment of perivalvular lesions (abscess, valve perforation, prosthetic valve dehiscence) with volumetric reconstruction [25].
In patients with complex congenital heart disease and the presence of prosthetic material, especially in the right heart structures or branch pulmonary arteries, the detection rate of vegetations is low even with the use of TOE [26]. Valve regurgitation may be suggestive of fistula formation or leaflet perforation. A regurgitant jet originating from the central part of a leaflet is highly suggestive of a perforation. In addition, a periprosthetic valve dehiscence with a newly detected regurgitation is highly suspicious of IE (Fig. 2). However, mild isolated periprosthetic regurgitation may also be observed in the absence of infection [27]. The severity of an acute regurgitation should be quantified with both modalities (TTE and TOE) combining anatomical, semiquantitative and quantitative parameters [28].
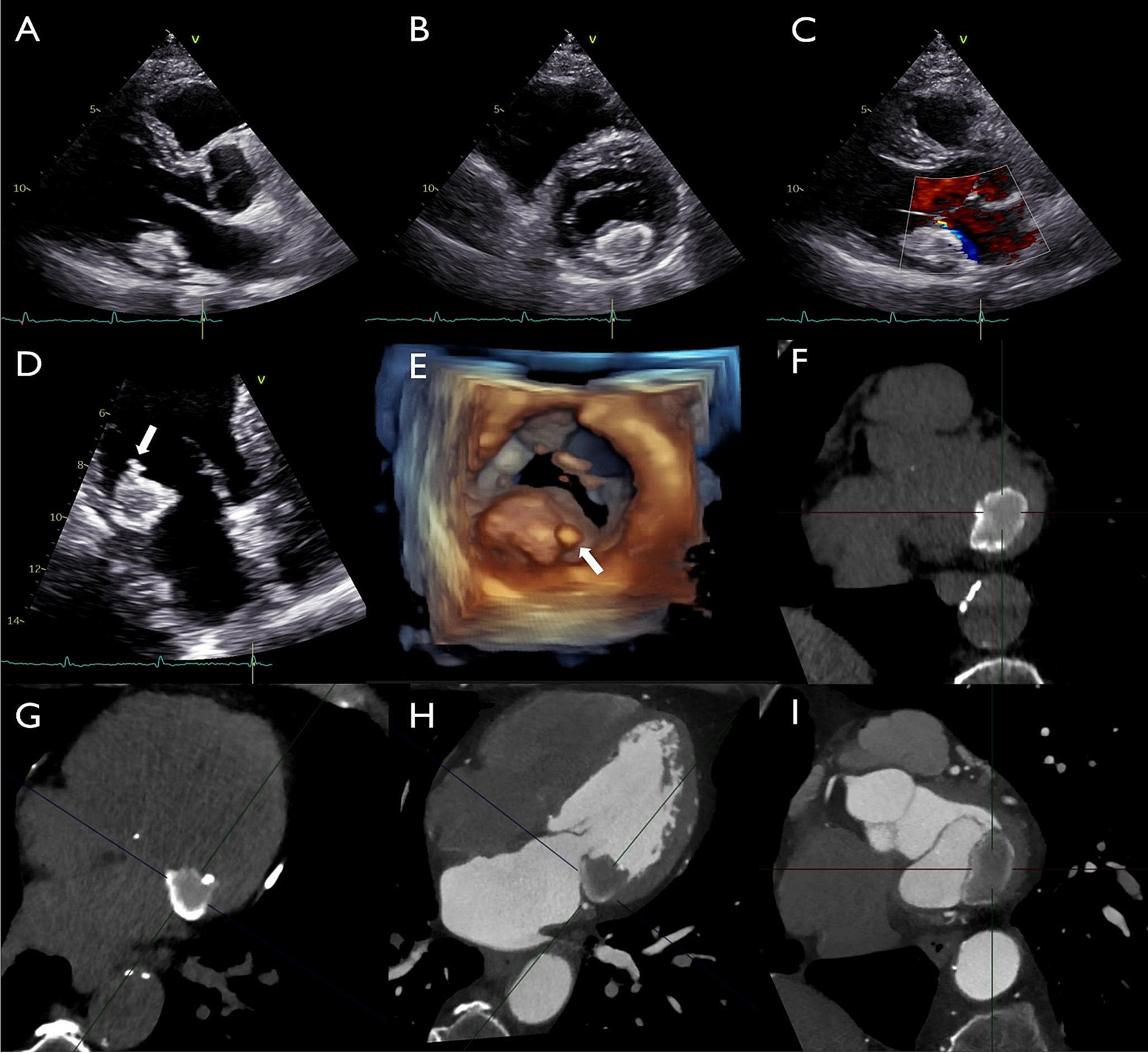
Fig. 7
42-year-old female presented with chest pain. CT coronary angiogram, performed to rule out coronary artery disease, incidentally revealed a rounded mass attached to her pulmonic valve leaflet (Image A). This finding was confirmed on transthoracic echocardiogram (RVOT view) (Image B). The differential diagnosis included a benign tumor or a vegetation, although endocarditis was thought to be less likely as the patient did not have any signs or symptoms of systemic infection. For further tissue characterization, the patient underwent cardiac MRI. SSFP bright blood imaging (Image C) showed the mass attached to the pulmonic valve. Edema-weighted imaging (STIR) (Image D) revealed increased signal intensity of the pulmonic valve mass, indicating increased water content. Late gadolinium-enhancement imaging (Image E) demonstrated diffuse gadolinium uptake within the mass, suggesting a fibroblastoma. This case highlights the tissue characterization capabilities of cardiac MRI using multiple sequences and emphasizes the ability of MRI to differentiate vegetation from a benign tumor, particularly when the echodensity has limited mobility. The patient opted for surgical removal of the mass, which was confirmed to be a pulmonary valve fibroblastoma.
In case of intracardiac device-related IE, both TTE and TOE have limited diagnostic accuracy. Intracardiac echocardiography (ICE) is an emerging invasive imaging modality that detects device lead abnormalities and small vegetations attached to the leads and is useful to guide transvenous lead extraction and thus minimize the risk for periprocedural complications, such as pulmonary embolization or incomplete removal of vegetations [29].
The timing and echocardiographic mode (TTE or TOE) depend on the initial findings, type of microorganism, and initial response to antibiotics, according to the recent ESC guidelines [1]. In case of a normal or inconclusive TTE or TOE and high clinical suspicion of IE, echocardiography should be repeated within a week. There should be a low threshold for repeating TTE when a new complication is suspected with the option to further evaluate with TOE if required. Repeat TTE should be considered during follow-up of uncomplicated IE, to detect new silent complications and to monitor vegetation size. Echocardiographic evaluation of valve morphology and cardiac function is important at completion of antibiotic therapy or in patients who did not undergo surgery [1].
CT for IECTCA is an effective and readily available method of assessing cardiac valves and the surrounding heart for features of IE. CTCA is most useful when used in conjunction with other forms of imaging and in the presence of prosthetic heart valves where artifact from surgical material can limit the diagnostic performance of other imaging modalities including TTE and TOE (Figs. 1, 2, 3, 4, 5, 6, 7). CTCA also has a role when other forms of imaging are unavailable or contraindicated. CTCA can add valuable information where abscess or pseudoaneurysm formation is suspected. CTCA may aid surgical planning and in some cases, offer an alternative to invasive coronary angiography prior to surgery [30, 31].
A meta-analysis of 8 studies prior to 2019 found a pooled sensitivity of 64% with a specificity of 88% for detection of vegetations on CT. When using multiphase CT sensitivity increased to 86% [30]. More recent studies report a sensitivity of between 80–98.6% of CT for the detection of endocarditis in native valves, with a specificity of 60%−62.5%. In prosthetic valves, a sensitivity of 71.4–81.8% and a specificity of 50% has been reported for endocarditis detection by CT [31, 34].
The size of the vegetation has bearing on the diagnostic performance of CT with smaller vegetations (< 10 mm) having a lower detection rate [32,33,34,35]. CTCA reveals the size, location, and attachment characteristics of vegetations with the benefit of high spatial resolution achieved with this modality. Full heartbeat acquisition images can be helpful in assessing the motion of the vegetation.
CTCA is an excellent modality to assess for paravalvular complications of endocarditis (Figs. 1, 3, 4, 5). Particularly where abscess or pseudoaneurysm are suspected [32]. Abscesses appear as paravalvular collections with a characteristic low attenuation. Pseudoaneurysms are irregular shaped cavities in the paravalvular region, these are contiguous with the cardiac or aortic blood pool and may appear pulsatile on full heartbeat acquisition images [36]. Reported sensitivities and specificities for the detection of abscess or pseudoaneurysm by CTCA range from 60 to 100% and 75% to 92% respectively [30, 31]. This is in keeping with the pooled sensitivity (78%) and specificity (92%) for abscess or pseudoaneurysm detection from the meta-analysis from Oliveira et al. [
Comments (0)