Data
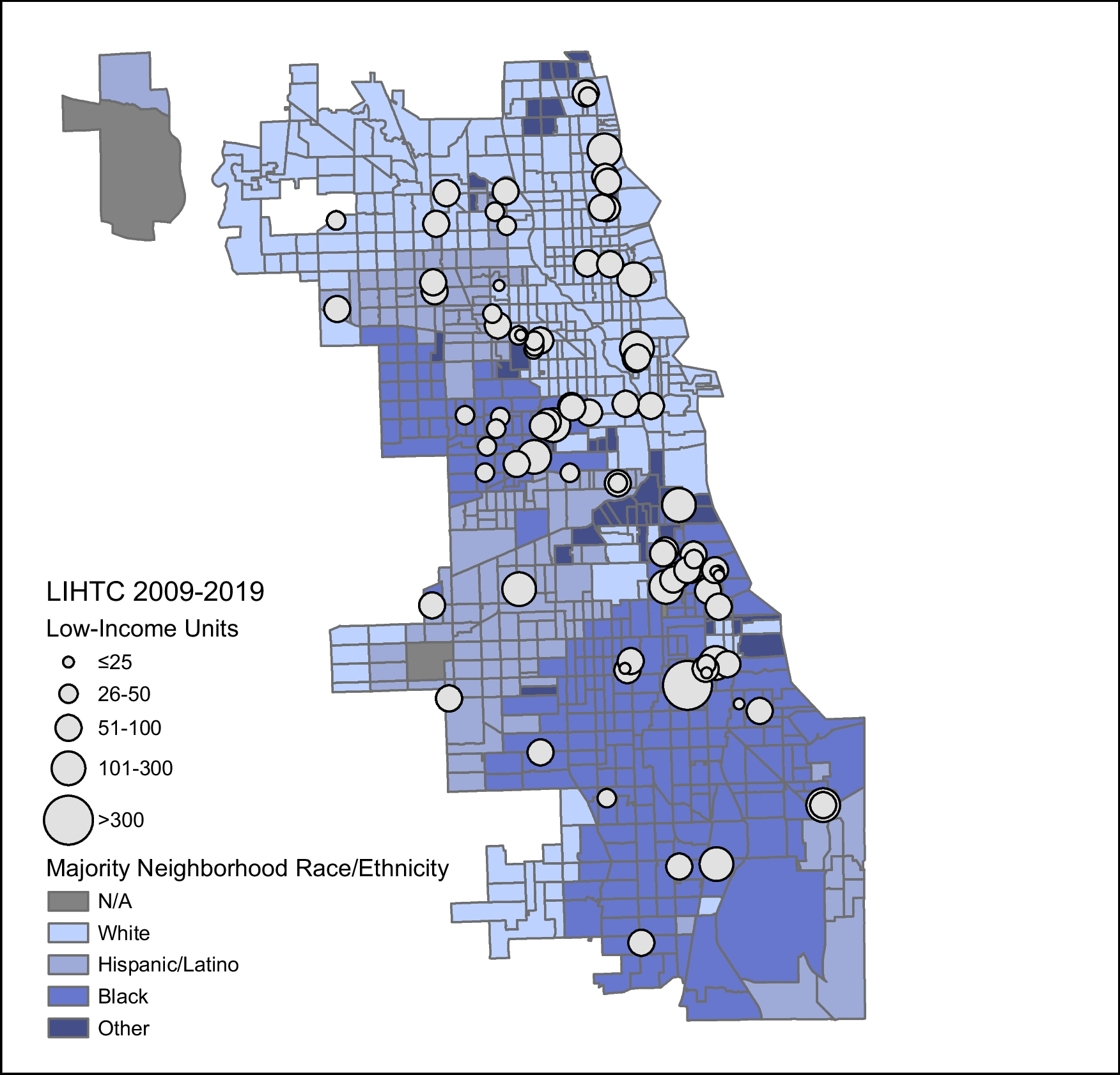
We conducted a retrospective cross-sectional study of adult outpatients at an urban academic medical center in Chicago, IL from 2018 to 2019 to examine whether LIHTC housing moderated associations between race/ethnicity and elevated blood pressure. Patients were included if they had a residential address in Chicago and at least one outpatient encounter. For housing data, we utilized a database of LIHTC developments maintained by the U.S. Department of Housing and Urban Development. We included LIHTC developments placed into service from 2009 to 2019 in Chicago, IL. For neighborhood characteristics, we used data from the 2015–2019 American Community Survey (ACS) 5-year estimates.
We additionally conducted secondary analyses to examine whether LIHTC housing was associated with higher access to health-promoting resources in the neighborhood. For neighborhood resources, we used 2017 data from the National Neighborhood Data Archive (NaNDA) [22], the most recent year published of the publicly available dataset. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for observational studies [23]. This study was approved with a waiver of informed consent by the University of Chicago Institutional Review Board.
Main Measures
The primary dependent variable was elevated blood pressure, obtained from electronic health records. We used objective blood pressure measurements instead of diagnostic codes to limit unmeasured confounding due to underdiagnosis or incomplete electronic health records. Thus, our variable does not necessarily reflect a clinical diagnosis of hypertension but includes all blood pressure measurements for a given individual, with variation in diagnosis, treatment, and control over time. We defined elevated blood pressure as a diastolic blood pressure ≥ 90 mmHg or systolic blood pressure ≥ 140 mmHg, i.e., stage II hypertension as defined by the Joint National Committee (JNC) [24]. We additionally conducted sensitivity analyses defining elevated blood pressure at lower (≥ 130/80) and higher (≥ 160/100) thresholds, based on clinically meaningful criteria.
The primary independent variable was self-reported race/ethnicity. We created a categorical variable for race/ethnicity, which included White (referent), non-Hispanic Black, Hispanic or Latine, unknown/patient declined, or other. The primary moderator of interest was the presence of LIHTC. We created a binary variable indicating whether patients lived in a census tract with or without LIHTC units. We incorporated this variable into the model as an interaction term with race/ethnicity. To account for variability in development size, we also used the median number of LIHTC units as a cutoff and conducted analyses comparing no LIHTC units, < 90 LIHTC units, or ≥ 90 LIHTC units in a census tract.
We adjusted for patient age, sex, insurance status (self-pay, Medicaid/dual eligible, Medicare, private), earliest year of LIHTC placement (2009–2019), and tract-level poverty (defined as > 20% of households below the federal poverty line [FPL]) [25]. Adjustment for tract-level poverty was necessary to address confounding related to any preferential allocation of LIHTC based on neighborhood socioeconomic status, although LIHTC developments were nearly evenly distributed across poor and non-poor neighborhoods during the study period (52.2% versus 47.8%, p = 0.11). We initially included neighborhood racial composition as a theoretical confounder, but multicollinearity testing demonstrated a variance inflation factor of 5.61 for Black patient race and Black neighborhood racial composition. Neighborhood racial composition was thus removed from final models.
Statistical Analysis
Descriptive statistics were calculated for all patients and census tracts. This study used mixed-effects hierarchal logistic regression to examine elevated blood pressure as a function of race/ethnicity (model 1) and race/ethnicity-LIHTC as a multiplicative interaction effect (model 2), nested at tract and patient levels. All models adjusted for the aforementioned confounders.
Analyses were conducted using Stata IC, version 17 (StataCorp LLC). Maps were created using ArcGIS Pro, version 2.2.0.
Neighborhood-Level Resources
A secondary analysis utilized information from NaNDA, which included tract-level counts of ambulatory health care, grocery stores, gyms/fitness centers, and social services. We examined subtypes within social services, including services for children/youth (e.g., adoption centers, foster care placement services, youth centers), seniors/people with disabilities (e.g., senior centers, adult day care centers, disability support groups), individuals/families (e.g., suicide crisis centers, substance use disorder self-help centers), and vocational services (e.g., job training and counseling). For each resource type, we created quartiles using the number of resources in each tract to describe resource availability as scarce, low, medium, or high within each tract.
We used ordinal logistic regression to analyze neighborhood resources as a function of LIHTC. The dependent variable was a 4-level ordinal variable of the level of resource availability (described above). The independent variable was a binary variable indicating whether LIHTC units were present or absent in a census tract. We adjusted for tract-level age (mean), sex (% male), poverty (binary; > 20% households below the federal poverty level), and racial/ethnic composition. For tract-level racial/ethnic composition, we created a categorical variable which classified tracts as majority Black, Hispanic/Latine, White, or “other” race/ethnicity, with more than 50% of a single race/ethnicity comprising a majority.



Comments (0)