The education of young surgeons is a critical issue that requires serious attention and support in today’s rapidly evolving field of UGI surgery [6,7,8]. General surgery residents should gain familiarity with esophageal and gastric surgery and should have the opportunity to pursue this subspecialty during their careers. This necessitates training in preoperative patients’ assessments, therapeutic decision-making, patient selection for surgery, surgical techniques, and postoperative care. To achieve these goals, a structured curriculum is essential. Unfortunately, the diversity in surgical education and training across Europe has not been adequately addressed so far. Our survey aimed to gather insights from both trainees and trainers to provide an overview of current practices and identify potential gaps and solutions. In comparison to previous surveys, this study provides a snapshot of training in UGI surgery throughout Europe, focusing in various aspects of patient management and extracurricular activities [9,10,11].
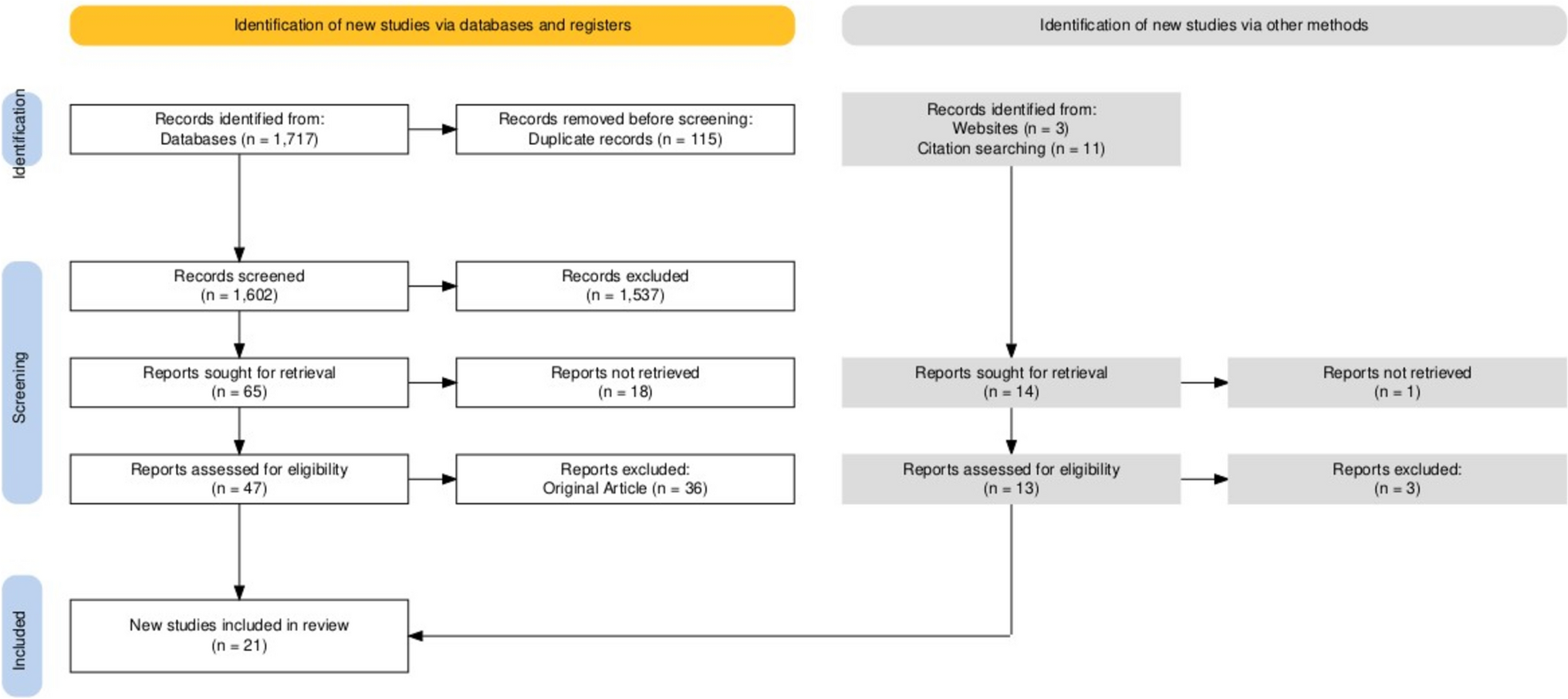
We collected 207 responses from 117 trainees and 90 trainers across 18 European countries. Both trainees and trainers shared some concerns about the scarcity of complementary training, suggesting that online and video resources could be particularly beneficial especially in low-volume centers. Neither UGI endoscopy nor esophageal functional studies are integrated into the routine surgical practice of the residents. In contrast, multidisciplinary discussions with gastroenterologists were reported to be generally effective. Regarding interventional endoscopy, most residents lack training opportunities despite being often involved in managing postoperative complications. Only about 20% reported being able to perform interventional endoscopic procedures such as esophageal stent placement, stricture dilation, and EndoVac placement.
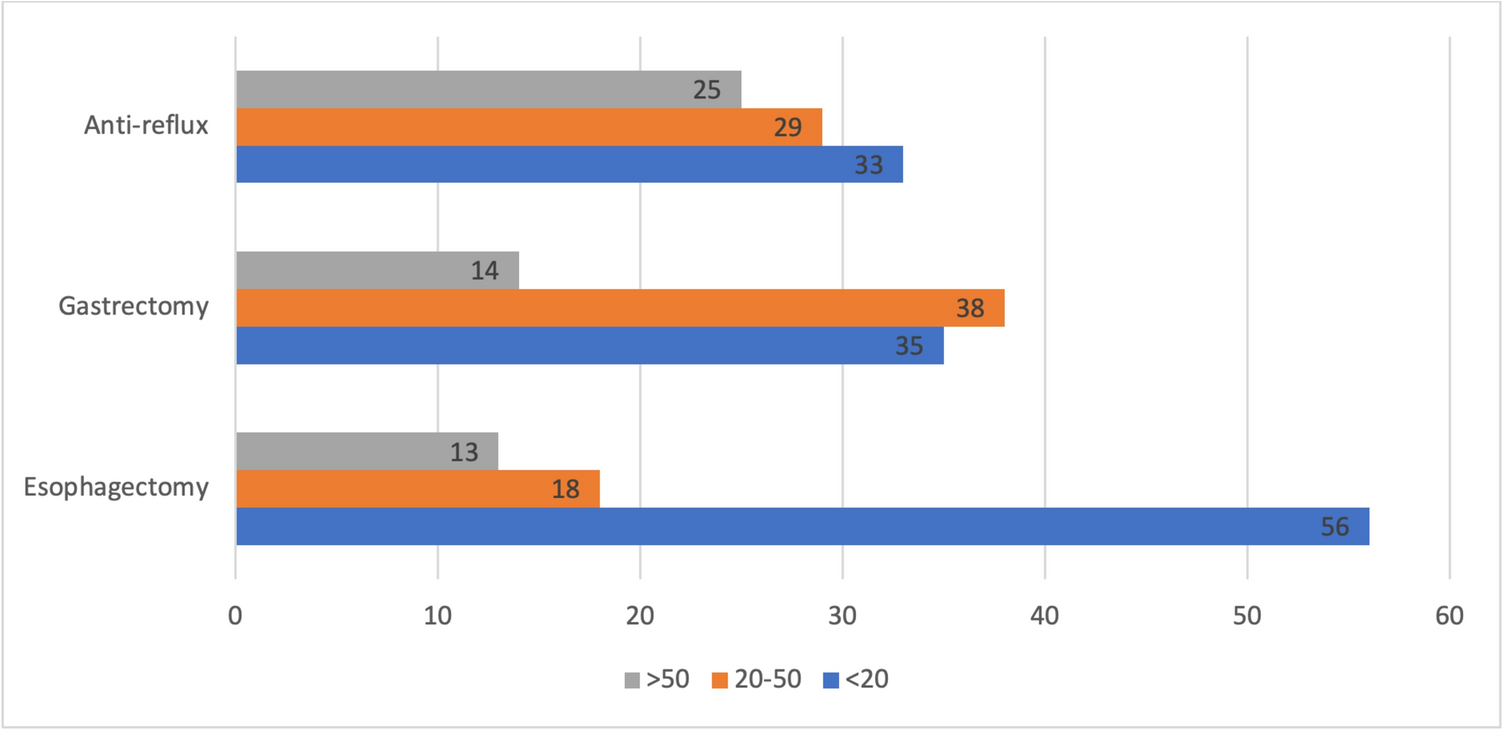
Both trainers and trainees were asked about the steps of various surgical procedures, the difficulties encountered, and the most appropriate tasks for independent performance. Interestingly, while 67% of trainers report that residents perform as first-hand surgeons in their practice, only 32.5% of residents agree. Also, crura dissection and gastric fundus mobilization are the steps residents feel confident to perform, and over 50% of trainers are willing to allow residents to take on these tasks. For gastrectomy, both trainers and trainees consider lymphadenectomy as the most challenging step, followed by digestive tract reconstruction after total gastrectomy. The most commonly performed steps by residents are greater and lesser curvature dissection, and reconstruction after subtotal gastrectomy. Similar patterns are observed in esophagectomy, where thoracic and cervical esophagus dissections, as well as the reconstruction phase, are considered difficult by both trainers and trainees. However, only 25% of residents feel confident in performing esophageal dissection, gastric mobilization, and fashioning of the gastric conduit.
Overall, a clear pattern emerged from this survey study. Trainers tend to be more permissive in allowing residents to perform certain steps, while residents lack confidence, possibly due to inadequate experience or lack of support and encouragement from trainers. The absence of a standardized curriculum and progressive training approach may contribute to this ambiguity and insecurity. Given that most surveyed residents are in their final residency years, the lack of confidence in performing basic surgical steps of UGI surgical procedures is concerning and signals the urgent need for a reform in education and training. Trainers should encourage residents’ participation in all aspects and phase of patient’s management at an early stage of the residency program [12]. While most trainers seem to encourage residents to engage in extracurricular activities, only one-third of trainees feel supported in this complementary training also because of the limited offer of dedicated training opportunities. Since hands-on training emerged as a preferred extracurricular activity, European surgical societies and University medical centers should promote and organize more of these events, ensuring equitable access to quality training for residents. The present survey identified the urgent need for a structured curriculum in UGI surgery as an essential complement to existing theoretical resources. Creating a library of instructional videos could help to fill identified gaps and allow trainees to understand complex interventions even in low-volume centers with no specialized UGI units [13]. In addition, there is a need to promote training in UGI endoscopy and functional studies of the esophagus [2].
Standardizing surgical training in UGI surgery is crucial. To address the current gaps, promoting a structured and incremental teaching approach can help residents to feel more confident and better understand the responsibilities involved in daily surgical practice. With adequate training and guidance, residents can eventually gain the ability to safely perform complex procedures [14,15,16]. Still, there is a lack of objective and robust data describing the operative experience of general surgical trainees outside the USA [17]. A previous national French survey study showed that a master diploma did not contribute to improve surgical training, whereas progressing in surgical autonomy was a driving factor to dissipate the feeling of dissatisfaction perceived by residents [18]. A worldwide survey focused on oncological UGI surgery showed that trainees spend much of their time observing or assisting particularly in esophageal resection, and more than half of the participants performed less than five UGI surgical procedures both in their residency and fellowship periods [10].
In the current era of “vocational crisis” in surgery and evolving technological scenario, it is important to provide more opportunities to improve the degree of satisfaction of the junior residents who should be encouraged to participate to regular pelvic trainer sessions, animal, and cadaver labs, and online video sessions. With the rising adoption of robotic surgery across Europe, standardized curricula will be fundamental for optimal training and certification, ensuring safety and consistent outcomes with this technology [19]. Also, in the near future, robotics and artificial intelligence with computer vision systems will likely enable residents to improve their technical skills and the quality of the surgical procedure by providing identification of anatomical landmarks and recognition of sequential steps of each surgical procedure [20, 21]. International guidelines and expert recommendations should shape the training pathway in this emerging scenario, emphasizing hands-on experience as a core component. However, there is a shortage of dedicated centers for such complementary training. Collaborative efforts among European experts, guided by the European Foregut Society (EFS) and the European association for Endoscopic Surgery (EAES), should create a comprehensive map of training centers that offer structured, hands-on educational opportunities. Lastly, the European Board of Surgery (FEBS) should certificate a minimum level of proficiency ensuring that recipients of the fellowship possess both the theoretical knowledge and practical skills necessary to excel in UGI surgery across Europe and beyond.
We recognize that the primary limitation of this study is the small sample size and the possible selection and recall bias. However, the present research serves as a cross-sectional overview of the European surgical education system and is intended to lay the foundation for developing dedicated guidelines for general surgical residency programs. Identifying gaps is beneficial only when efforts are aimed at finding solutions. Developing a competency-based curriculum alongside a multidisciplinary approach is vital for surgical residents. Expertise in surgery is achieved through practice, making high-quality education and training essential for adequately preparing the next generation of UGI surgeons and mentors [22,23,24].

Comments (0)