This study supports the prognostic value of the impact of ISR on postoperative functional recovery even in cases of signal reduction exceeding 50% compared to predissection values.
Indeed, according to our results, the detection of ISR ≥ 31% between the minimal and the maximal values of signal recovery following LOS has been related to normal VCM in POD-1. Moreover, all patients who experienced intraoperative recovery, regardless from the values, present normal VCM within 30 days from the surgical procedure.
The relevance of these findings relies on the potential for appropriate modulation of surgical strategy, which may help to avoid ST when specific intraoperative recovery parameters are documented.
If the type of LOS is known to be predictive of postoperative recovery of laryngeal motility[24], with Type II LOS associated with a more favourable prognosis compared to Type I LOS[25] and even signal reductions exceeding 50% are well-known to frequently correlate with the postoperative detection of VCP[16], comprehensive data regarding ISR following LOS are currently lacking, predominantly consisting of isolated case reports or small case series[15, 26,27,28]. Among the available studies, Schneider et al.[28] addressed traction as the most frequent cause of intraoperative stress for the ILN and identified ISR rates, whether specific precautions are taken during the surgical procedure performed by means of C-IONM. Notably, traction injuries are reported to occur more frequently in the area of Berry’s ligament: this phenomenon is likely attributed to the variability in the anatomical relationships between the ILN, Berry’s ligament, and the adjacent vascular structures[29,30,31].
Given these considerations, a tension-free thyroidectomy has been proposed as a strategy for minimizing traction-related nerve stress, thereby reducing the risk of intraoperative ILN functional complications[32]. Indeed, even signal reductions exceeding 50% during intraoperative monitoring are known to be associated with a high probability of postoperative VCP[16]. Conversely, the likelihood of VCP is considerably lower for signal reductions below the 50% threshold. Additionally, even minor increases in latency (greater than 10%) may potentially be associated with VCP in the postoperative setting. This latency parameter is particularly significant when C-IONM is used during surgery[16].
Clearly, in contrast to I-IONM, continuous stimulation techniques may facilitate the early detection of signal reductions, thus enabling the adoption of timely precautions to avoid complete LOS[19], although the superiority in terms of cost-effectiveness of C-IONM over I-IONM has not been exactly assessed yet[33].
Among the signal reductions exceeding 50% compared to predissection values, various risk classes have been identified basing on the magnitude of the observed signal reduction[16]. Delving deeper, electromyographic variations detected through IONM are categorized into non-threatening changes, combined events, and LOS, basing on the associated risk for injury to the ILN[16].
Although only I-IONM has been employed in our clinical practice, we meticulously considered all the events characterized by a greater than 50% reduction in vagus nerve signal compared to predissection values, particularly when a partial ISR was documented but the amplitude remained below the 50% threshold.
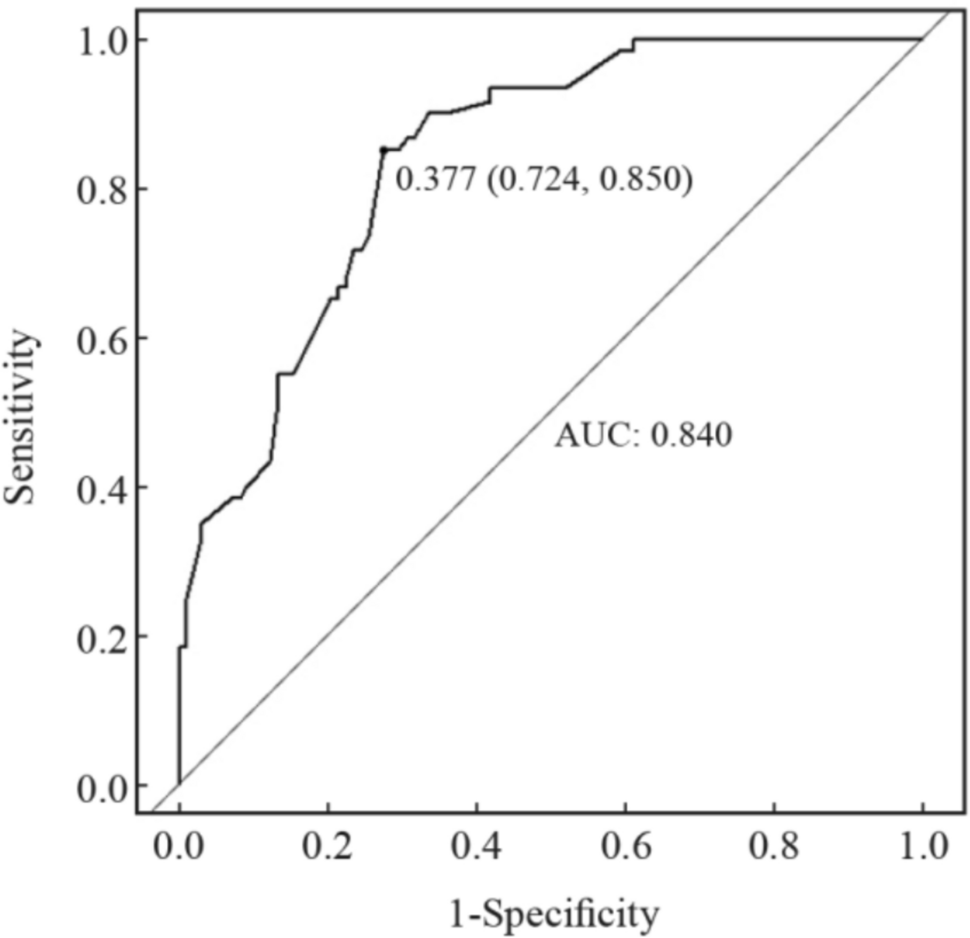
With regard to the outcomes of our study, we sought to identify a cut-off value for ISR following LOS, that could serve as a predictor of postoperative recovery of VCM. In detail, we found ISR ≤ 31%, between the first and the last values of signal recovery after LOS, as the minimal cut-off with a 100% sensitivity, thus serving as a predictive factor for VCP (specificity 20.8%). Youden index identified 0.837, corresponding to an ISR ≤ 13%, as the best cut-off in terms of sensitivity (94.1%) and specificity (89.6%) for VCP.
In this context, it is to underline that literature data are only partially in line with our results. Indeed, if ISR below the range of 50% to 70% after LOS is acknowledged to represent a risk factor for postoperative paralysis[9, 16], a specific intraoperative recovery threshold that may reliably predict the absence of postoperative VCP, when ISR remains below 50%, has not been defined yet. Schneider et al.[9, 16] made the effort to identify a correlation between intraoperative evidence of signal recovery and postoperative laryngeal outcomes, by detecting < 50%ISR, after LOS, as a value associated with postoperative VCP in 70%−100% of patients.
This study is not without limitations. Firstly, our final analysis is confined to patients with documented partial ISR following LOS, which inherently resulted in a relatively small sample size. Furthermore, the monocentric and retrospective design of our study introduces additional constraints. Nevertheless, these limitations are counterbalanced by our rigorous patients' selection criteria. Another potential drawback is related to the use of I-IONM rather than C-IONM, which may offer more comprehensive insights into intraoperative nerve function. Moreover, I-IONM enabled an assessment of the "amplitude" parameter but precluded the evaluation of the "latency" parameter of the vagus nerve signal.
On the other hand, the strength of our findings relies in the extensive experience of our referral center, with a caseload of more than 2000 neck procedures annually, and in the multidisciplinary management of the endocrine disease. To our knowledge, this study represents the first attempt to define a cut-off for ISR for predicting VCM status in the postoperative setting. More specifically, we aimed to provide interval values between the first and last post-dissection vagus nerve signals when LOS followed by less than 50% ISR, facilitating the estimation of postoperative laryngeal motility.
Our findings suggest that ISR may represent a reliable predictor of the full recovery of VCP. A ≥ 31% ISR is associated with normal postoperative VCM, indicating that ST could potentially be avoided in this subgroup of patients. Conversely, a ≤ 13% ISR may correlate with postoperative hypomotility. For ISR values ranging between 13 and 31%, hypomotility may or may not be present.
When an adverse event occurs on the first side during a planned TT, the decision to proceed with the surgical dissection ultimately rests with the operating surgeon, who must accurately consider the specifics of the clinical case alongside its own technical expertise.
These findings may enhance our ability to predict early postoperative cord mobility, thereby allowing for potentially avoiding further surgical trauma whether a satisfactory ISR percentage suggests normal cord function in the postoperative setting. However, larger prospective studies employing similar protocols and extended follow-up durations are still necessary to definitively validate our results.

Comments (0)