This study showed that a two-year multicomponent intervention failed to induce significant structural or functional cardiac changes in frail, sarcopenic older adults. We did not observe significant differences due to intervention on LV remodeling and in systolic or diastolic functions of RV and LV.
The sample considered in the present study is composed by subjects enrolled at the Frailty Clinic of University-Hospital of Parma site for the SPRINTT project (CARDIOSPRINTT) [2, 12].
The SPRINTT randomized controlled trial aimed to evaluate the efficacy of a multicomponent treatment, based on moderate intensity physical exercise and nutritional counseling (1.1–1.2 g/kg of protein daily intake) on mobility-disability incidence prevention, compared to a lifestyle education program in physically frail, sarcopenic older adults. The heart was not the primary target of the trial, which focused on the risk of motor disability. This goal was successfully achieved, as the control group exhibited a higher rate of mobility disability (52.7%) compared to the intervention group (46.8%, p < 0.005) [10].
In our population, MCI showed a greater improvement in SPPB compared with HALE confirming the results of the entire trial.
The CARDIOSPRINTT is an ancillary study focused on evaluation of cardiac adaptations in a population at high cardiovascular risk, in order to identify prevention strategies to reduce cardiovascular mortality. This target is not necessarily far from the main outcome of the original trial, given the existence of a close correlation between CV diseases, sarcopenia and frailty [2]. This is the reason why sarcopenia and frailty have been proposed as new CV risk factors in geriatric patients [13,14,15].
In a previous published work, we both evaluated at baseline the cardiac adaptations of the frail, sarcopenic older individuals and identified the determinants of left ventricular mass [12].
In addition, we demonstrated in the follow-up data at 24 months a significant correlation between LVM and SMM confirming the existence of the cardio-sarcopenia syndrome [2].
In the present paper, we longitudinally analyzed the impact of the two-year multimodal intervention on the cardio-sarcopenia syndrome, and did not find significant effects on the heart in the MCI compared with HALE.
To our knowledge, the effect of physical activity on cardiovascular structure and function in older people with frailty and sarcopenia has never been thoroughly investigated. The present study aims to fill the gaps on this topic and this represents a strength. In addition, the sample size, albeit not very numerous, was homogeneous for age, with physical frailty defined as a SPPB score between 3 and 9 and low ALM, as required by SPRINTT protocol [8, 9].
Several hypotheses may explain why the intervention failed to affect cardiac outcomes: first of all, the intensity of the exercise, designed in the LIFE study and adopted in SPRINTT, to prevent disability, was probably not enough to induce changes in the cardiac parameters within two years [11]. Furthermore, it is possible that the length of the study was not sufficient to determine long-term effect of physical exercise on the CV system. We should also acknowledge the wide variability of multimorbidity in this population, and the already mentioned different goals of SPRINTT and CARDIOSPRINTT [8,9,10]. Compared to the main SPRINTT trial, our sub-study aimed to test the effects of the exercise protocol on cardiac structure and function and not just the prevention of disability. These findings suggest that exercise programs should be tailored to the individual’s degree of functional impairment—more intensive for mildly frail, and lighter for severely physically impaired subjects.
However, the longitudinal analysis of this study clearly demonstrated the effects of the CV aging process in both ventricles [16, 17]. We observed significant and group-independent variations over time, of LV structure such as a significant decrease in end- diastolic (EDV) and end-systolic (ESV) volumes (respectively p < 0.001 and p = 0.003). We hypothesized that all these changes were the consequences of the progression of diastolic dysfunction, concept well-supported by the reduction of LV E’ wave (Epv: p = 0.042).
The impaired LV relaxation resulted in lower ventricular filling, i.e. preload, and thus LV volumes, and CO reduction (p < 0.001). However, LVM did not significantly change at follow-up compared with baseline.
Regarding LV systolic function, EF, a well-known pump function parameter, did not change but myocardial systolic waves (Spv: p < 0.001; Stvi: p < 0.001) were reduced over time suggesting a progression of systolic dysfunction. All these findings are in accordance with the concept of cardiac aging [16, 17].
The effects of aging were confirmed at the RV analysis by a reduction of S and E’ myocardial waves confirming the progressive impairment of systolic and diastolic function involving also this chamber.
Unexpectedly, RWT, an index of LV geometry, slightly decreased (p = 0.034) at follow-up, as would be expected in view of the aging progression of diastolic dysfunction leading to a change from eccentric to concentric remodeling [16]. This finding will require confirmation by future studies.
After adjusting for sex, BMI, SBP and age, almost all differences due to the time disappeared. However, a significant effect due to the time-group interaction was observed on LV for FS which increased in MCI and decreased in HALE (p < 0.001) suggesting an improvement of systolic function in the active group.
Although we did not show significant effects on cardiac remodeling and LVM induced by physical exercise, physical performance globally improved, as the median SPPB score changed from 7 [7–7.5] to 9 [7,8,9,10] in the general population with a greater increase in MCI group.
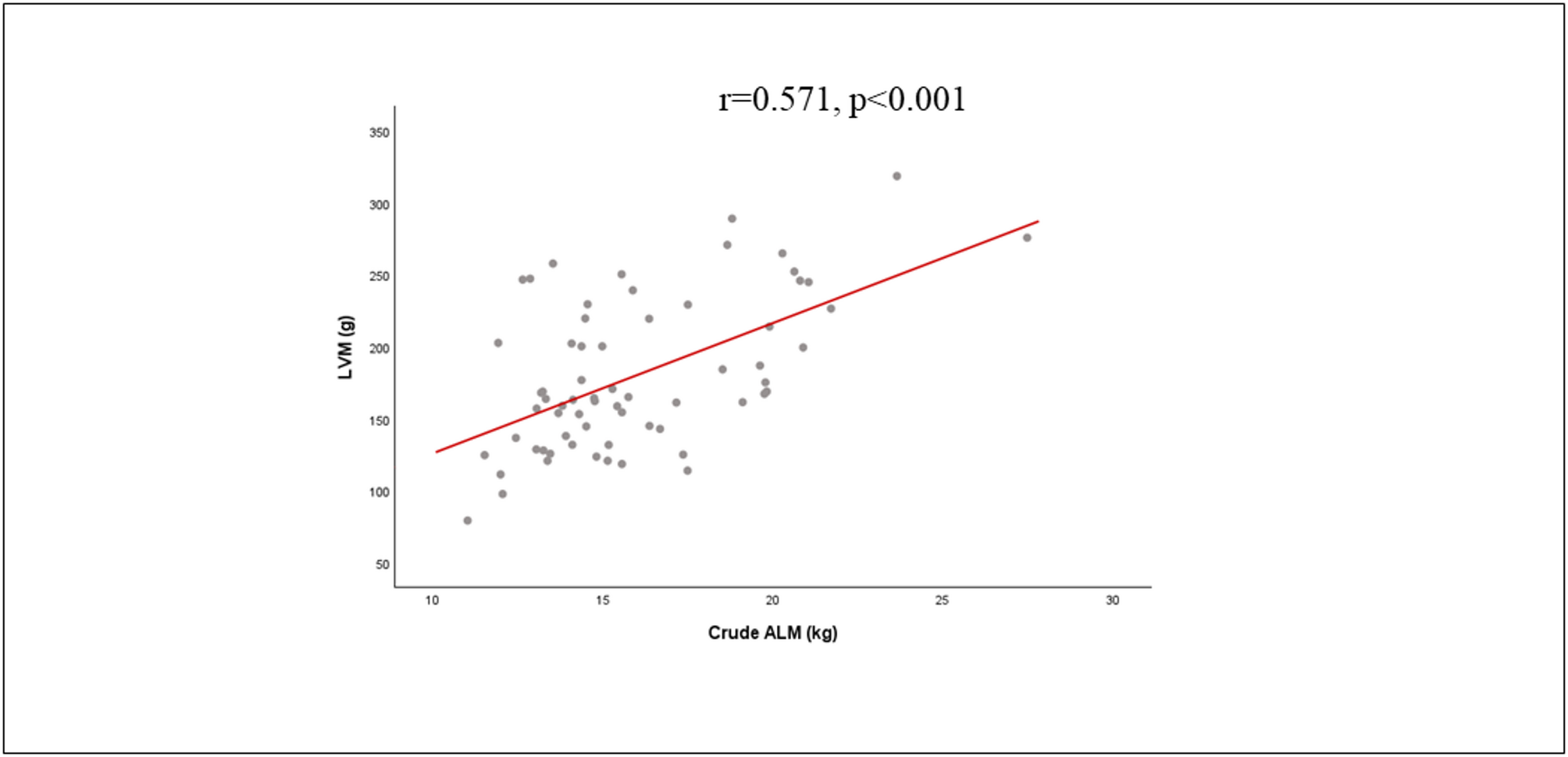
The cardiac -skeletal muscle axis was also analyzed longitudinally, and we confirmed the close correlation between LVM and SMM (r = 0.571, p < 0.001), previously demonstrated in the cross-sectional part of the CARDIOSPRINTT [2].
The cardio-sarcopenia syndrome, as firstly described by Keng et al. [1], is a novel entity in which a reduction in mass coexists in the skeletal and cardiac muscle. Compared with the study of Keng et al. [1], we assessed skeletal mass with DXA instead of BIA.
These results seem to disagree with data reported in the literature that have shown an increase in LV thicknesses and LVM in aging, changes attributed to cardiac adaptations resulting from increased aortic stiffness and consequent increase in systolic pressure. However, these observations were detected in a large population independently from other concomitant syndromes including sarcopenia.
It must be underlined that we demonstrated the existence of cardiac- skeletal muscle axis in the specific setting of sarcopenic and frail older adults not receiving much attention in the current literature. The specific setting and characteristics of the patients do not allow the translation of these results in all older people [1, 2]. However, after further confirmation in populations different from the CARDIOSPRINTT, the cardiac-skeletal muscle axis could become a specific target to multidomain interventions addressing cardiovascular aging. According to these preliminary results, sarcopenia should be added as a marker of heart’s health, highlighting the need for cardiovascular screening in sarcopenic patients.
Despite the potential strengths of the study, we should also acknowledge some limitations. First, the small number of participants evaluated in the CARDIOSPRINTT; second, the not optimal adherence to the study in the MCI: of the 46 subjects, more than 15% did not complete the entire program or attend it continuously. Several factors may have contributed to reduced adherence in the MCI group, including neuropsychological issues, social burdens, physical comorbidities (e.g., obesity, osteoarticular disease), and caregiving responsibilities.

Comments (0)