
Remember me
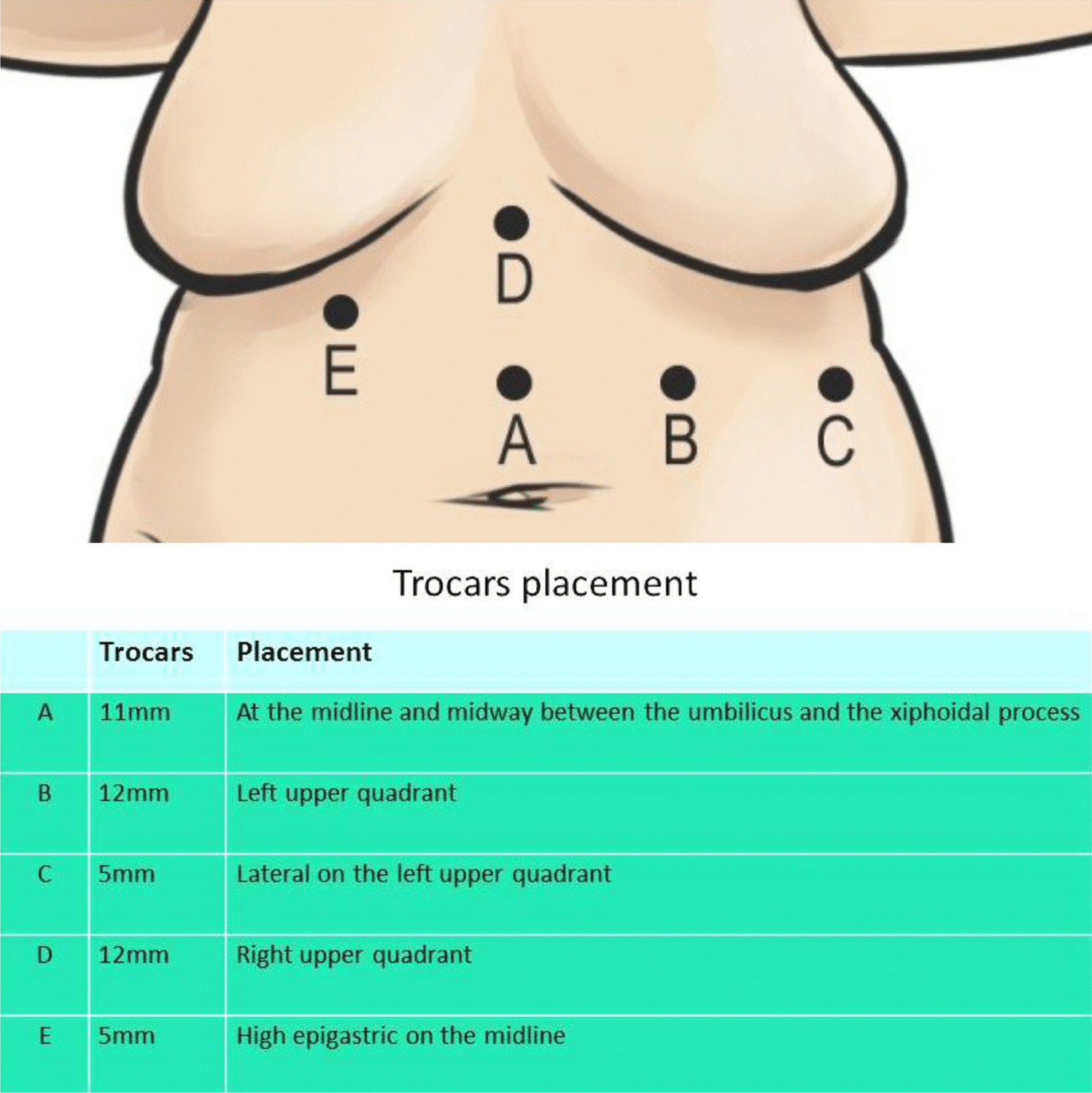
The procedure was performed laparoscopically with the patient in the supine, split-leg position and in reverse Trendelenburg. A five-port technique is employed (Fig. 1). Adhesiolysis was first carried out to expose the right crus, which was separated from the caudate lobe. The left lobe of the liver was retracted to expose the hiatus. Dissection of the esophagus and stomach from the right and left crura was performed, followed by mediastinal dissection to achieve adequate esophageal mobilization. The previous Nissen wrap was taken down using a harmonic scalpel, preserving the vagus nerve and gastric blood supply. At least 3–4 cm of esophagus was mobilized intra-abdominally without tension.
Fig. 1
Trocars placement positions
A hiatal hernia repair was then completed. A gastric pouch was created around a 36 Fr gastric lavage tube, and a stapler was used to complete the pouch toward the angle of His. The ligament of Treitz was identified, and a jejunal loop was brought up antecolically, rotated, and anastomosed to the gastric pouch 100 cm distal to the ligament. A gastrojejunostomy was performed using a 45-mm linear stapler, ensuring correct alignment of the afferent and efferent limbs to avoid torsion. Stapler openings were closed with absorbable sutures. The Roux limb measured 100 cm in length.
A linear 60-mm stapler with a white cartridge was used to create a side-to-side jejunojejunostomy. The resulting enterotomy was lifted using three holding sutures (PDS II 4/0, Ethicon, USA) and closed longitudinally with a stapler. The remaining blind loop of the biliopancreatic limb was transected and removed using a similar linear stapler. A methylene blue leak test was negative. No intraoperative complications occurred.
Postoperatively, the patient was prescribed proton pump inhibitors for six months. She was discharged on postoperative day 3, remained asymptomatic, and had a BMI of 24.5 kg/m2 at six months. At 12 months, she achieved 89% excess weight loss with no recurrence of GERD.
Comments (0)