There have been only five reports of hepatic FNH occurring after liver transplantation [15, 16]. The age at FNH occurrence ranged from 2 to 62 years, with four patients being male and one female (Table 1). The time from liver transplantation to FNH development ranged from 15 to 118 months, and the mass diameter at diagnosis ranged from 1.3 to 6.7 cm. Two of the five cases had two FNHs (Table 1). The causes of liver transplantation included biliary atresia, hepatitis B, hepatitis C, and HCC. At diagnosis, the background liver fibrosis included cirrhosis in one case and chronic hepatitis in three cases (one case not mentioned). Pathologically, this case showed a mild fatty liver and mild inflammatory cell infiltration in the portal area, but no fibrosis.
Table 1 Clinical features of cases of focal nodular hyperplasia after liver transplantationTransplant-induced vascular changes, such as intraoperative vascular manipulation and vascular anastomosis, are thought to cause hepatic FNH after liver transplantation [15, 16]. Wanless et al. reported that impaired liver perfusion releases platelet-derived growth factors from hepatocytes, which can cause hyperplasia of hepatocytes [3]. They also noted that a major abnormality of FNH is an increase in regional arterial blood flow [3]. Kumagai et al. concluded that FNH begins with thrombosis of the hepatic artery or portal vein, leading to local hepatic ischemia or necrosis, followed by reopening of the hepatic artery and transient tissue hyperperfusion, which results in nodule formation [17].
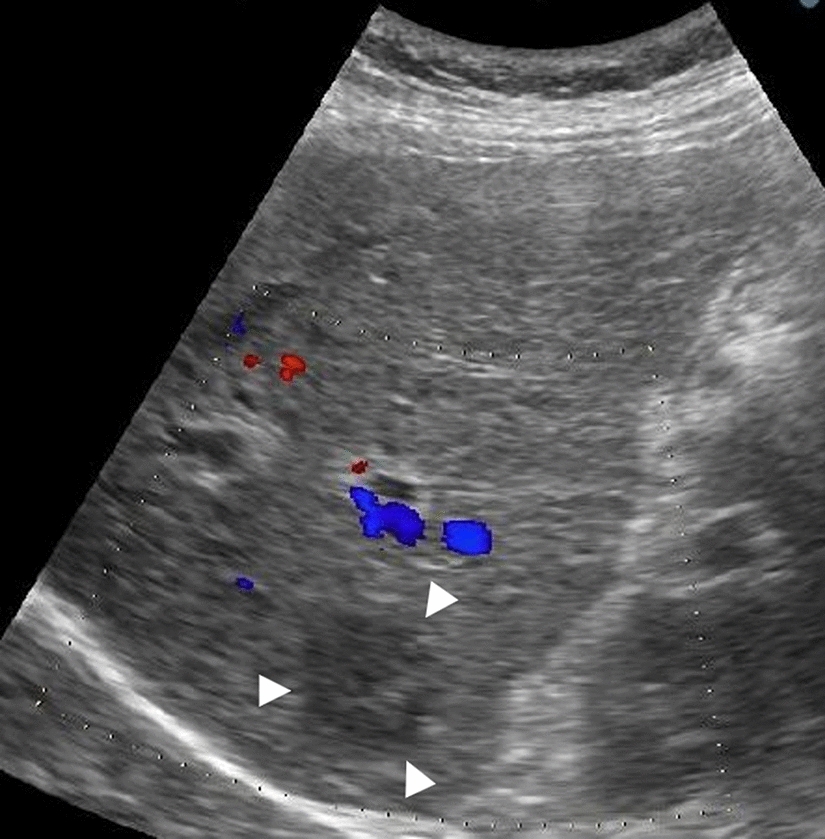
Three of the five previously reported cases of hepatic FNH occurring after liver transplantation had a history of portal vein thrombosis (PVT), which is considered a contributing factor to FNH development [15, 16]. However, there was no obvious history of PVT in this case. Ra et al. noted that the occurrence of FNH after living donor liver transplantation is plausible [15]. This is likely because living-donor liver transplantation involves more extensive manipulation of liver vessels than brain-dead donor liver transplantation, making it more susceptible to thrombosis [18]. Additionally, post-liver transplant patients face an increased risk of coagulation abnormalities, rejection, and infection, which may further contribute to thrombosis [19]. In this case, the patient experienced recurrent cholangitis associated with stenosis of the bile duct anastomosis. A needle biopsy was performed and no obvious thrombus was found in the specimens. However, thrombus formation in the small portal vein and hepatic artery may have contributed to the development of FNH. Furthermore, CECT performed one year after transplantation revealed a hyperattenuating lesion in the liver, which was undetectable on B-mode US but was identifiable as a tumor two years later. The liver biopsy specimens did not have enough of the background liver; therefore, it was difficult to state that immunosuppressant and rejection affected intrahepatic blood flow and development of FNH in this case.
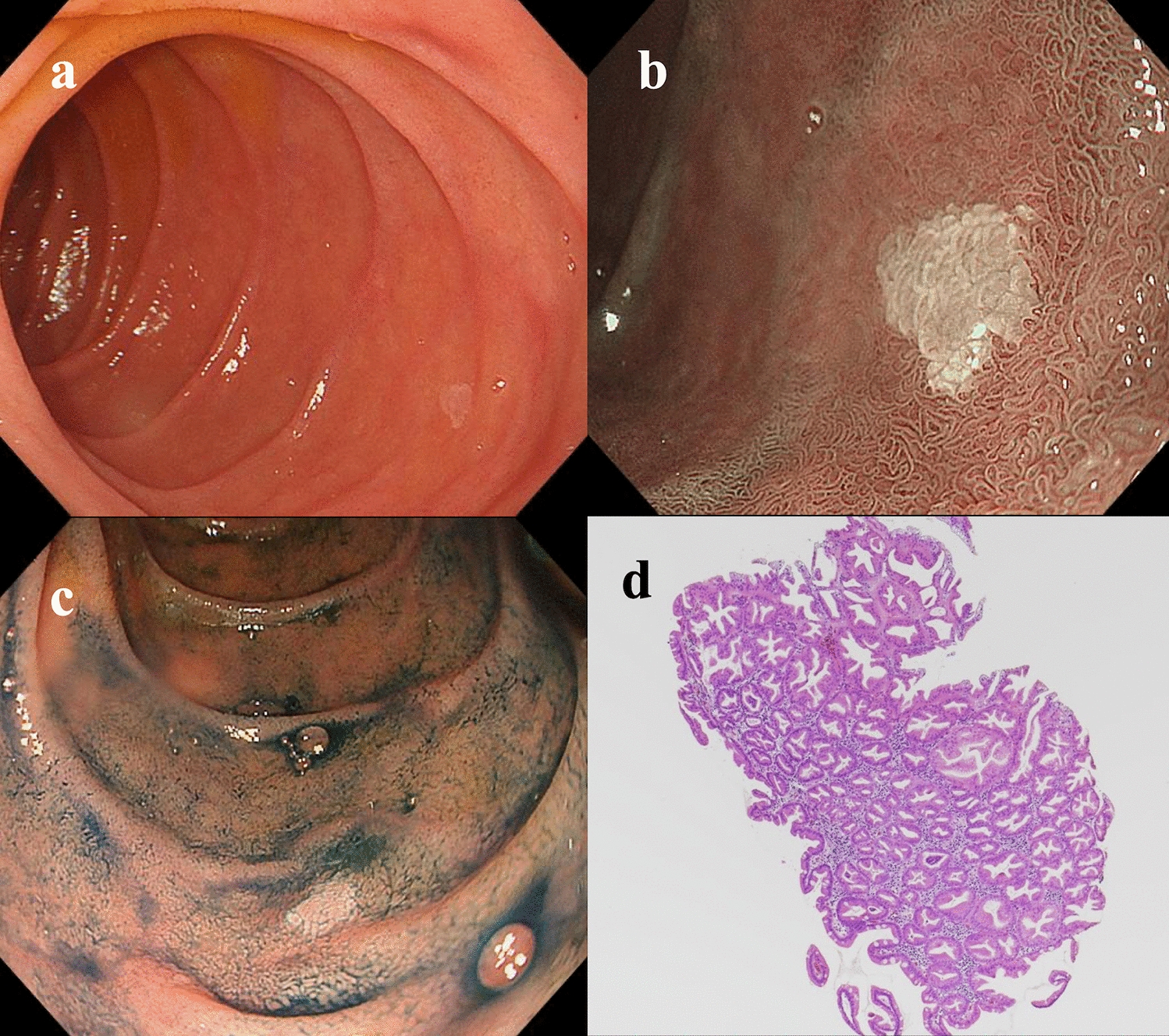
We believe that the increase in small muscular vessels observed in this case reflects the developmental process of FNH and provides valuable insights into its progression through imaging. In this case, FNH exhibited hypointensity in the hepatobiliary phase on EOB-MRI, which was atypical. Consequently, HCA or recurrence of HCC was also considered; however, the liver biopsy results confirmed the diagnosis of FNH. There were three lesions present and only the largest was diagnosed as FNH through liver biopsy. Therefore, careful follow-up with imaging studies is necessary for the other two smaller lesions. Since FNH, like HCC, appears hypervascular on imaging, it should be considered when new lesions are detected in the liver after transplantation. Furthermore, if imaging findings are atypical for FNH, as in this case, a liver biopsy is essential to establish the correct diagnosis. FNH is potentially more prevalent in liver transplant recipients than in the general population. Due to the lack of cases described, the diagnostic potential may be overlooked by pathologists and clinicians. FNH has not been acknowledged as a potential etiology of liver nodules post-transplant and warrants consideration in the differential diagnosis of hepatic nodules in transplanted livers.


Comments (0)