
Remember me
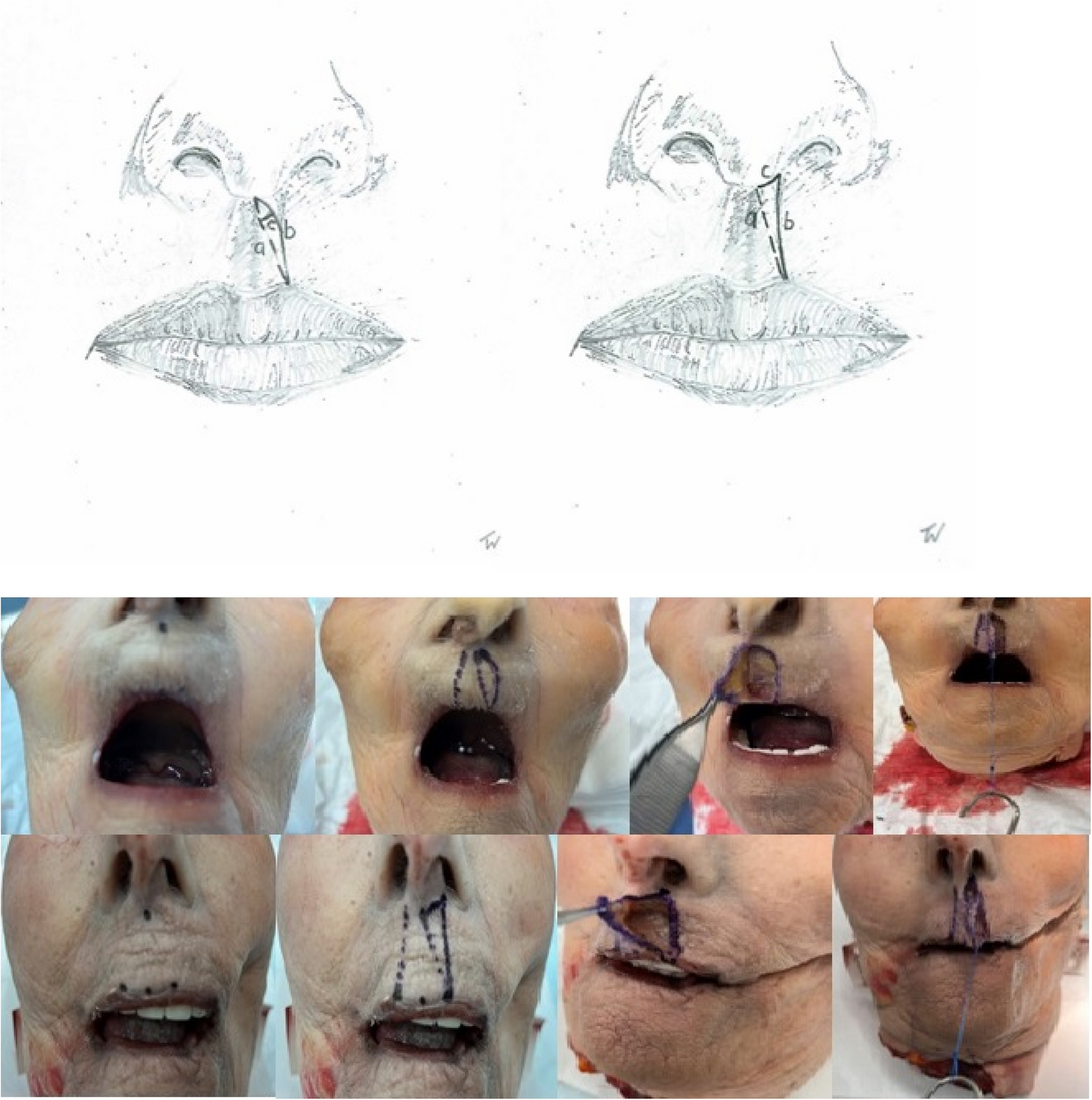

After screening the relevant literature, we conducted a cadaver study to gain theoretical insights into the physical properties of skin distraction. No previous study has demonstrated, in a cadaveric model, the extent of lip lengthening achievable with Millard’s technique compared to others. Ten intact adult cadaveric heads, without any signs of trauma, were obtained from the willed donor program at the affiliated medical university cadaver lab. Age and nationality were unknown. Pediatric heads were unavailable; therefore, the effect of aging skin on elasticity could not be measured. When searching actual public databases for studies on biomechanical properties of the skin, we found a recent comprehensive review paper on this topic with the main result that aging skin becomes thinner, stiffer, less tense, and less flexible. Skin tension measured during in vivo uniaxial load and elasticity modules are higher in children than in elderly adults. Mean ultimate skin deformation before bursting is 75% for newborns and 60% for the elderly [12]. From this, we conclude that there is a certain comparability between the skin of old and young people. All specimens were fresh-frozen and defrosted immediately before dissection. In five of the ten specimens, standard Millard advancement-rotation flaps were dissected under loupe magnification on the left side of the philtrum. In the remaining five specimens, back-cut incision flaps were raised as part of our designated Z-back-cut cheiloplasty. We measured the length of the incision lines in Millard’s advancement-rotation flap (see Fig. 1a–c, left) and our back-cut incision (see Fig. 1a–c, right) under varying tension forces (see Fig. 1, below). Line a runs from the center of the lower base of the columella in a straight line to the highest lateral point of the Cupid’s bow. Line b runs from the same starting point to the identical end point, but according to Millard’s incision technique, and line c represents the maximum distance between these two lines of the left part of Fig. 1. On the right side of Fig. 1, line a is identical, while c represents the line from the starting point of line a along the lower base of the columella to its lateral edge with an extension to the highest point of Cupid’s bow, line b. These tension forces were derived from our own clinical experience during unilateral cleft lip repair. The measurements were taken twice per different tensile stress using an elastic stainless-steel ruler with 0.5 mm marking increments. However, measurements were only taken to an accuracy of 1 mm to reduce bias. Cadaver measurements were done exclusively by the corresponding author to reduce inter-observer variability.
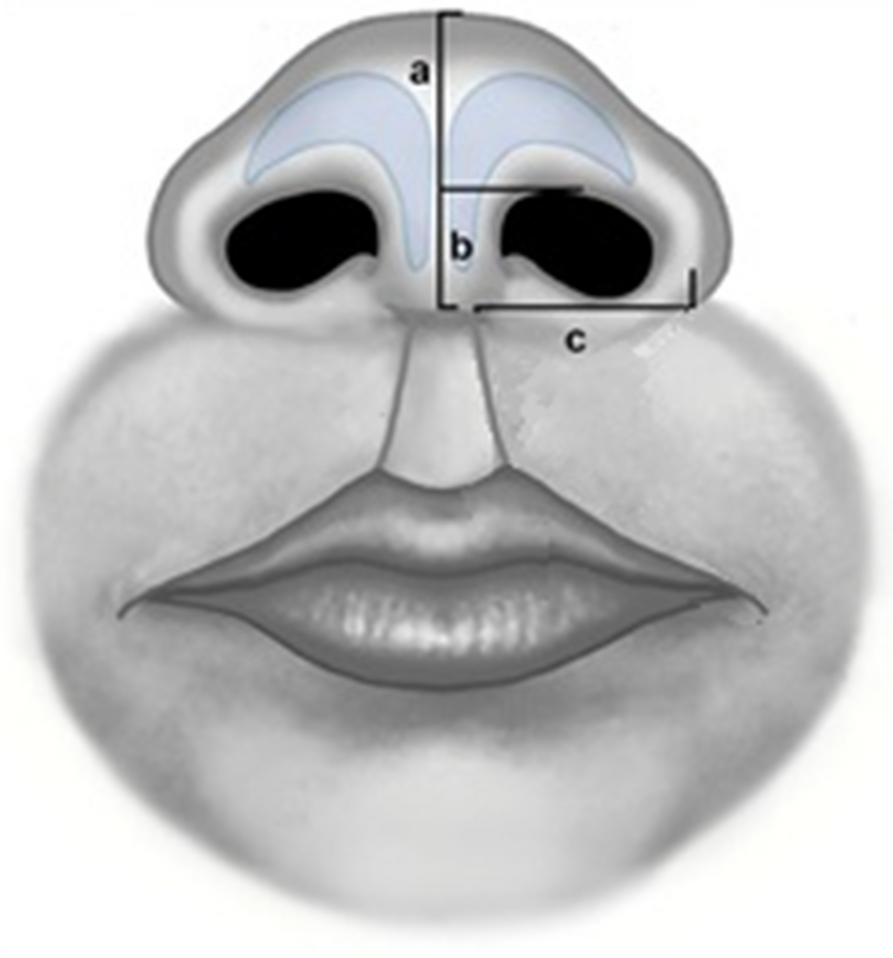
Fig. 1
Incision lines in our cadaver model; left according to Millard (line b) and right with a straight line with a back-cut (line c and b). Drawing of Millard incision, back-cut incision, and tension force lengthening test. Starting point of line a on the left: Center of the base of the columella. End point of line a on the left: highest lateral point of the cupid’s bow. Line b on the left: identical start and end points. Line c on the left represents the maximum distance between line a and line b. Line a on the right is identical to the left side, starting point of line c is as for line a, but runs along the lower base of the columella to its lateral edge and extends caudally to the end point of line a on the right
As force increased, line a asymptotically approached line b; therefore, no further measurements of line c were conducted in the Millard group. The resulting length of the back-cut technique under tensile stress was calculated as line a, roughly derived from the sum of line b and c. Results were presented in tabular forms (see Tables 1 and 2). Data visualization and statistical analysis were performed using the software package R [13]. We found a lip lengthening effect of the back-cut incision up to 35% compared to the Millard design. Figure 2 supported by the cadaveric findings, we introduced our incision pattern in clinical practice. The Institutional Review Board classification was stated “exempt”, as known surgical techniques were used in combination.
Table 1 Lengthening in the craniocaudal direction of the lip with the Millard techniqueTable 2 Lengthening in the craniocaudal direction of the upper lip with the back-cut techniquePatientsPatients with partial or complete unilateral cleft lip or cleft lip/alveolus/palate were selected. Surgery was performed by the first author using the technique described below. Individuals with complete cleft lip and palate were treated similarly to those with unilateral cleft lip. Postoperative follow-up adhered to our cleft team protocol. However, due to the COVID-19 pandemic, delays occurred in treatment and follow-up beginning in January 2020 (patients characteristics see below).
Gender
Date of birth
Date of operation
Age at the operation (month)
Type of cleft
Follow-up on cleft team
Complications
Male
May 2023
March 2024
10
Complete lip/bone/palate left
April 2025
Complete dehiscence of the soft palate and partial dehiscence of the lip caused by an infection
Male
December 2022
August 2023
8
Partial lip/bone left
September 2023
None
Female
October 2022
August 2023
10
Partial lip/bone left
December 2024
None
Female
February 2023
November 2023
8
Complete lip/bone left
January 2024
None
Male
March 2000
February 2024
23 years
Complete lip/bone/palate right
November 2024
None
Female
January 2022
February 2023
13
Complete lip/bone/palate right
April 2024
Complete dehiscence of the soft palate and lost to follow-up since April 2024
Female
May 2022
May 2023
11
Complete lip/bone/palate left
November 2024
Postop. airway obstruction caused by a combined Furlow plasty
Male
August 2020
March 2021
11
Partial lip/bone left
February 2023
None
Female
September 2019
January 2020
3
Complete lip/bone/palate left with Simonard
December 2024
Mild hypertrophic scarring of the lip
Female
September 2019
October 2020
13
Complete lip/bone/palate left by microdeletion
January 2025
None
Female
December 2021
August 2022
7
Partial lip/bone left
June 2024
None
Female
February 2020
February 2021
11
Complete lip/bone with ocular hypertelorism
August 2023
Hypertrophic scarring as a consequence of a postoperative wound infection of the lip with sec. corrections, lost to follow-up since October 2023
Male
May 2020
November 2024
5
Partial lip left
November 2022
None
Male
November 2019
November 2024
12
Partial lip/bone right
February 2025
None
Male
November 2003
January 2024
20 years
Complete lip/bone right
January 2024
Lost to follow-up since January 2024
Male
March 2024
January 2025
10
Bilateral complete lip/bone/palate
February 2025
None
Male
July 2024
Februayr 2025
6
Complete lip right
March 2025
None
Drawings and surgical techniqueThe incision design is illustrated in Fig. 2. Initial steps include marking of Cupid’s bow, the subnasal, the lateral base of the columella on the cleft side, and an additional perpendicular marking 2 mm cranial to the cleft-side peak of Cupid’s bow in the white roll of the vermilion border under loupe magnification. From this point, a line is drawn just outside the vermilion border toward the nasal sill, with a back cut extending to the marked lateral columella base. From the Noordhoff point (the point along the lateral lip where the vermillion height is at its greatest and the white roll is well formed but becomes less distinct toward the cleft as the progressive deficiency of the orbicularis oris muscle), the incision is extended outside the vermilion border towards the cleft sill, incorporating a small Fisher’s triangle (as small triangular pennant skin flap above of Noordhoff point) cranially in the lateral white roll. A medial triangular skin flap is added at the nostril base. The dry/wet line of the vermilion is marked bilaterally. Small distal triangular flaps of the dry vermilion skin are created for additional lip volume. For complete clefts, two mucosal vermilion flaps are dissected to close the nasal floor. In incomplete clefts, they can be discarded. The orbicularis oris muscle and its subdivisions, such as the depressor septum nasalis muscle, are released from the base of the columella, nasal ala, and the alveolar cleft of the maxillary bony segment with a single or double mucosal incision at the oral vestibular sulcus. The vestibular mucosa is sutured with interrupted Vicryl 4.0 sutures, followed by cranial-to-caudal adaptation of the orbicularis oris muscle with PDS 4.0 and Vicryl 4.0 sutures. Skin closure begins at the vermilion border using Monocryl 6.0. The contralateral relaxing back-cut incision is positioned precisely in the sulcus of the contralateral white roll for Fisher’s pennant flap placement. The small flap is trimmed and sutured into place, followed by nostril closure. The triangular flaps of the Z-plasty at the columella base are adjusted to size before final closure. Excess mucosa is resected before placing steristrips across the suture line. In complete cleft lip and palate cases, primary rhinoplasty following McComb’s method (with blunt mobilization of the nasal skin around the lower latera) is performed, with a silicone nostril retainer placed for 6 to 8 weeks. The technique may also be suitable for secondary lip revision in adults (see Figs. 3, 4, 5, and 6). To date, a total of 17 patients with a partial or complete cleft lip have been operated on using the technique described here in the last 4 years. So far, one secondary revision has been performed; according to our cleft team protocol, these are in most cases-only performed in adolescence, sometimes in combination with rhinoplasty.
Fig. 2
Incision pattern on a left partial cleft lip, complete cleft lip, and intraoral lines at the intraoral lip sulcus
Fig. 3
Above: complete cleft lip and palate left at 4 months of age with presurgical taping, intraoperative drawings with immediate result and 6 months postoperative at the age of 1.5 years with a postoperative wound infection caused by continuously nostril retainer manipulation by the child and partial dehiscence at the alar base with scar contraction. Below: Z-back cut cheiloplasty at the age of 24 with preoperative, intraoperative, and postoperative photos at 6 months including the drawing pattern
Fig. 4
No increase in the length chance of line a in Millard’s incision line. Increase of lengthening of line a in the group of back-cut incision compared to line b in Millard design with 1N and 2.5N tension force. No further lengthening of both lines with 5N. With increasing tension, line a approximates line b in Millard’s technique, while lines b+c approximates line a in the back-cut technique. Lower Part: Percentage gain in length between the two incision patterns
Fig. 5
Operated upper lip at the age of 9 months, intraoperative result and 7 weeks postoperatively with our technique by partial cleft of the lip and alveolus
Fig. 6
Partial cleft of the left upper lip with closure by Z-back cut-cheiloplasty preoperatively at 2 weeks of age, direct intraoperatively at the age of 10 months and at 6 weeks postoperatively
Our tension force studies demonstrated insufficient lengthening of Millard’s advancement-rotation flap compared to our back-cut incision (see Fig. 4). Between 2.5 N and 5 N tension, no further lengthening occurred; thus, statistical analysis at 5 N was omitted. Comparisons between the two incision patterns at 1 N and 2.5 N showed no significant elongation with Millard’s incision, whereas the back-cut technique produced a significant increase. The results were highly statistically significant (p < 0.001, Student’s t-test). This suggests that Millard’s technique does not appear to achieve the expected skin lengthening via rotation and advancement. In contrast, an incision along the philtral column with a back-cut at the cleft-side columella base, as part of a Z-plasty, significantly enhances lengthening. Furthermore, the resulting straight line reassembles the lateral border of the philtrum more accurately. The resulting defect of the back-cut incision at the lateral base of the columella can be filled up with the cutaneous triangle of the contralateral side of the cleft as part of a Z-plasty.
Comments (0)