
Remember me

Prospective study of 32 patients with unilateral CL presenting to Ain Shams University hospitals between January 2019 and July 2022.
Included in the study were patients ages 3 months—1 year of age of both genders with unilateral CL.
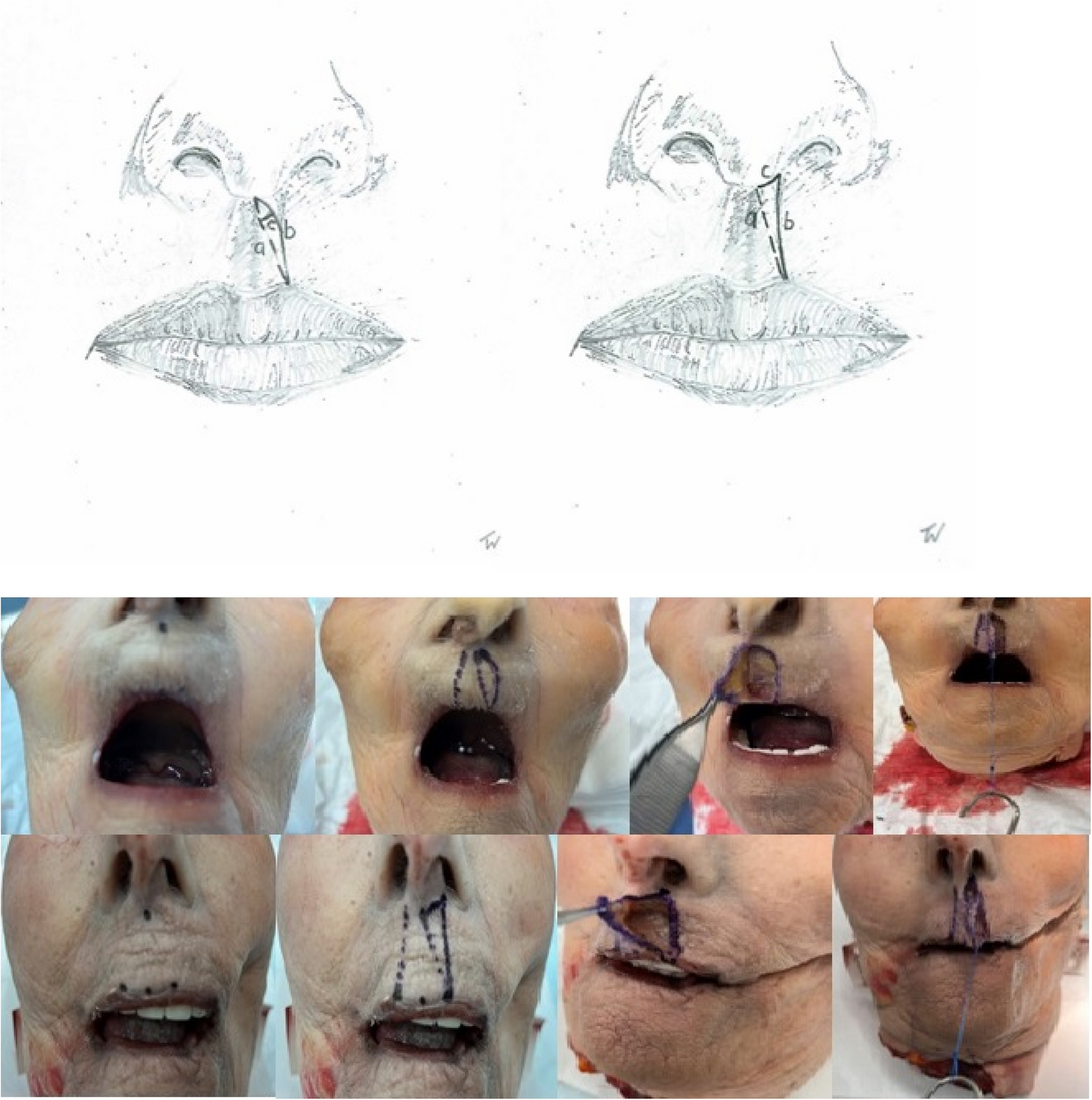
In all patients, primary rhinoplasty was performed at the time of lip repair. Lip repair was done by Tennison-Randall technique [13, 14]. Rhinoplasty was performed by dissection of the cleft side LLC and alar cartilage in the supraperichondrial plane to completely free it from the skin, nasal mucosa and abnormal attachments, through the lip repair incisions, plus extended columellar incision and alar rim incisions if needed, to allow for cartilage manipulation and skin redraping, then multiple suspension sutures were used with PDS 5–0 Ethicon® to reposition the LLC, and suspend it, allowing shifting of the alar dome at the genu, starting the sutures at the nasal mucosa, through the cartilage, then tying the sutures over a bolster in the direction of the nostrils. (Video 1). A nasal retainer was inserted after skin closure, and maintained for 3 months.
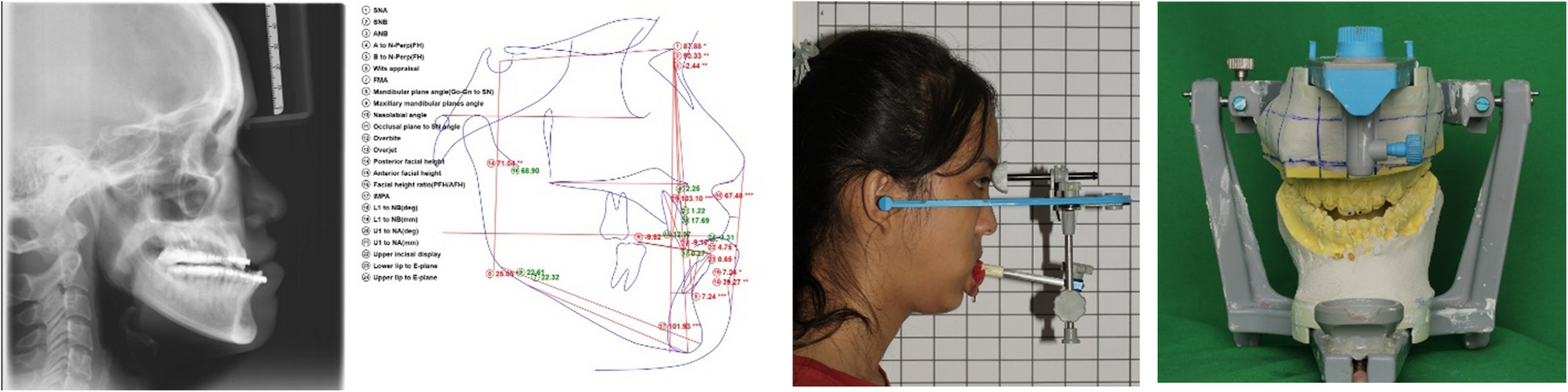
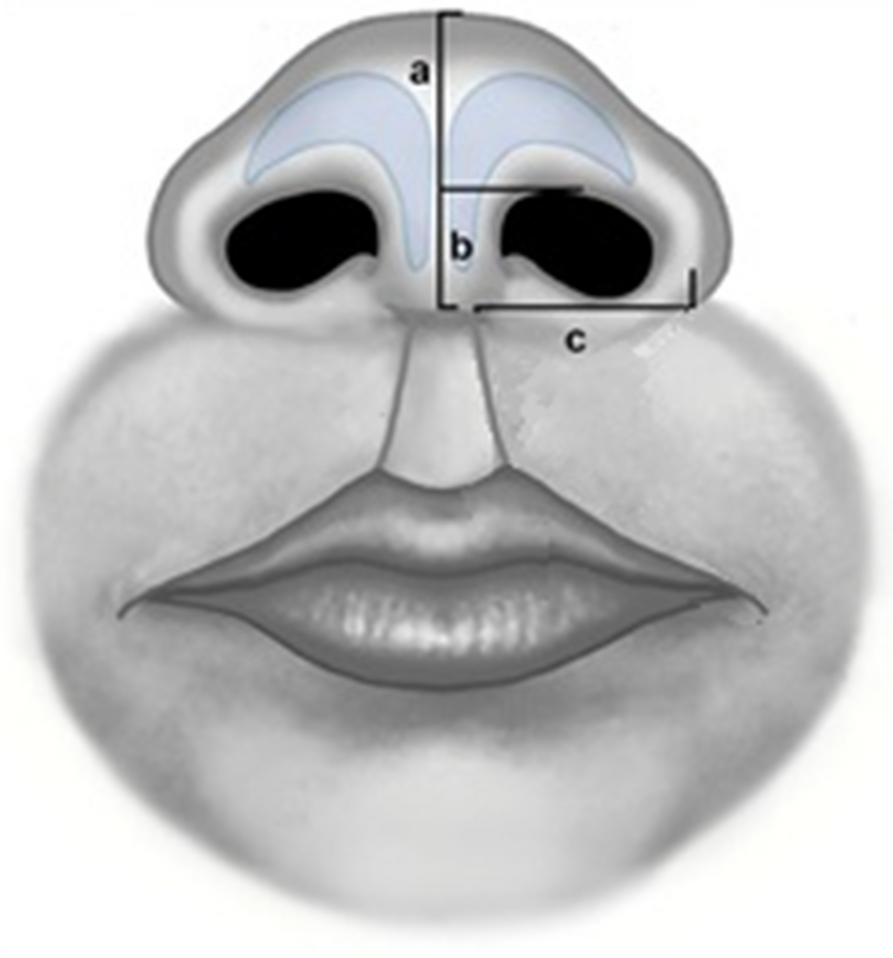
Evaluation of results was done by photographic assessment, anthropometric measurements, and parents’ satisfaction. All patients underwent the following measurements bilaterally to compare cleft side to normal side [15], 6 months post-operatively, as shown in Fig. 1:
(a)Nostril dome height: Measurement from the lateral border at the base of the columella to the highest point on the nasal dome.
(b)Columellar length: Measurement from the lateral border of the base of the columella to the highest point of the nostril at the same level.
(c)Alar width: Measured from the lateral border at the base of the columella to the most lateral point of the ala in a line perpendicular to the axis of the columella.
Fig. 1
Anthropometric measurements of nasal dimensions. a Nostril dome height (b) Columellar length (c) Alar width
These measurements were selected because they reflect the symmetry and centralization of nasal tip, the correction of columella to match non-cleft side and the correction of widened ala and horizontal nostril shape to match the non-cleft side [16]. Measurements were performed by two separate operators.
Parents’ satisfaction was assessed through a 5-point Likert Scale regarding their satisfaction with the cosmetic appearance of the repaired nasal deformity post-operatively, in which 1 meant very dissatisfied, 2 meant dissatisfied, 3 meant neutral, 4 meant satisfied and 5 meant very satisfied.
Statistical analysis was done by SPSS 16.0 statistical software package. Results are presented in the form of percentage for qualitative data, mean and standard deviation in case of quantitative variables. Statistical analysis for pre- and postoperative findings was performed using Mann–Whitney U Test.
The results were considered statistically significant if P value was below 0.05.
Comments (0)