Acinic cell carcinoma is a relatively rare malignant salivary gland neoplasm [8]. Cases of metastasis of acinic cell carcinoma have been reported to the lungs, cervical lymph nodes, and to the orbit [2, 6, 13,14,15]. However, as per the authors’ literature review, this is the first case study of metastatic acinic cell carcinoma to the heart.
Although acinic cell carcinoma is considered a low-grade salivary gland neoplasm, it is known to locally recur and metastasize. Case reports of acinic cell carcinoma with distant metastasis have identified lymph node involvement, perineural invasion, and lymphovascular invasion as prognostic predictors that aid in choosing a treatment plan, with the presence of any of these features supporting consideration of adjuvant therapy and more rigorous surveillance [2]. Lymph node metastasis, one of the major prognostic parameters in acinic cell carcinoma, has been reported in up to 10% of cases, despite being considered a low-grade salivary gland malignancy [6].
Currently, there is no specific histologic grading system for acinic cell carcinoma. High-grade transformation of acinic cell carcinoma was first described by Stanley et al. in 1988. It was defined as “areas of dedifferentiated high-grade adenocarcinoma or undifferentiated carcinoma” with associated areas of low-grade acinic cell carcinoma [10]. This and subsequent studies found that increased adverse outcomes are associated with so-called high-grade acinic cell carcinoma [11]. However, the definition of high-grade acinic cell carcinoma has not been consistent [11].
Xu et al. proposed a grading system that includes 4 histologic features: tumor necrosis, mitotic index, fibrosis at invasive front, and tumor borders [11]. In this grading system, acinic cell carcinoma was considered to be low grade for the following parameters: no necrosis or tumor fibrosis, no infiltrative front, and less than or equal to 1 mitoses/ 10 high power fields [11]. Intermediate grade was considered to be 2–4 mitoses/10 high power fields, or infiltrative tumor borders, or fibrosis at an invasive front [11]. High grade was considered to be greater than or equal to 5 mitoses/10 high power fields or tumor necrosis [11]. Using this grading system, high-grade acinic cell carcinomas carried a worse prognosis when compared with low-grade and intermediate-grade acinic cell carcinomas. If we applied this grading system to the case described in this report, the original tumor in the parotid gland would have been considered to the high grade due to the extensive tumor necrosis. This study also identified tumor size, older age, lymphovascular invasion, nuclear anaplasia, necrosis, and advanced pT and pN stages as independent factors for adverse prognosis [11]. The median age of those with low and intermediate grade tumors in this study was 46 years old, while the median age for high grade tumors was 62 years old [11]. The median tumor size for low and intermediate grade tumors was 2.5 cm, and the median size for high grade tumors was 3.0 cm [11].
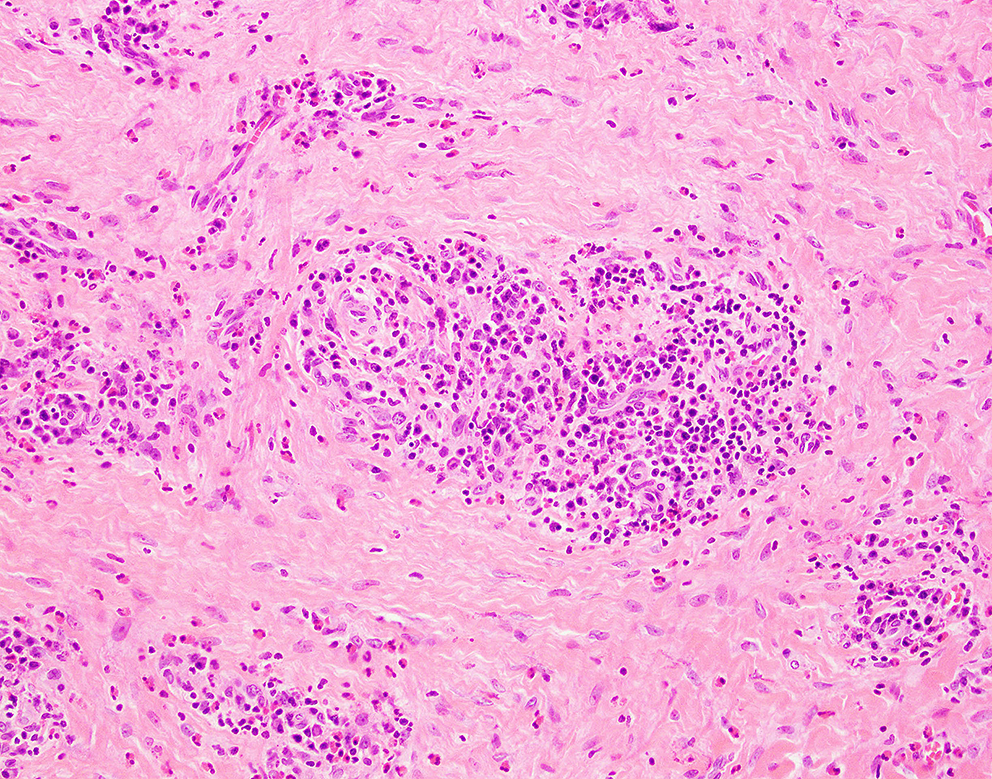
While there is no formal grading system for acinic cell carcinoma in the current AJCC Cancer Staging System and WHO classification of salivary glands, there is the inclusion of the presence or absence of high-grade transformation, which is defined as marked cytologic atypia, histologically distinct areas, atypical mitoses, increased mitotic activity, and tumor necrosis [12]. In this case, the primary parotid gland tumor possessed high-grade features in the form of significant tumor necrosis, although it possessed a relatively low mitotic rate of 2/2 mm2. Thus, histologic grading of the parotid gland tumor may have predicted an adverse prognosis.
Khan et al. conducted a study utilizing data from the Surveillance, Epidemiology, and End Results (SEER) database to identify risk factors that affect survival in patients with acinic cell carcinoma [12]. This study graded tumors as well-differentiated, moderately differentiated, poorly differentiated, and undifferentiated. The study found that the variable with the highest hazard ratio for death compared to the other variables is high tumor grade, as defined by the criteria for high-grade transformation in the current AJCC Cancer Staging System [12]. Thus, this study highlights the significant negative impact of histologic grade on prognosis for patients with acinic cell carcinoma.
Poorly differentiated and high-grade variants of acinic cell carcinoma are known to have increased rates of recurrence and metastasis, usually via hematogenous spread [9]. These high-grade and poorly differentiated variants have a reported recurrence rate of about 35% with a trend for late recurrence, going up to 30 years after initial presentation [13]. Spencer et al. describe a woman who experienced multiple late recurrences of acinic cell carcinoma, with lung and intracranial metastasis occurring 32 years after the initial diagnosis [14]. In a retrospective study with 2362 cases of acinic cell carcinoma of the parotid gland, both high histologic grade and regional metastasis, discussed above, as well as advanced tumor stage, tumor size greater than 3 cm, and age over 70 years old, were all linked to a worse prognosis [16].
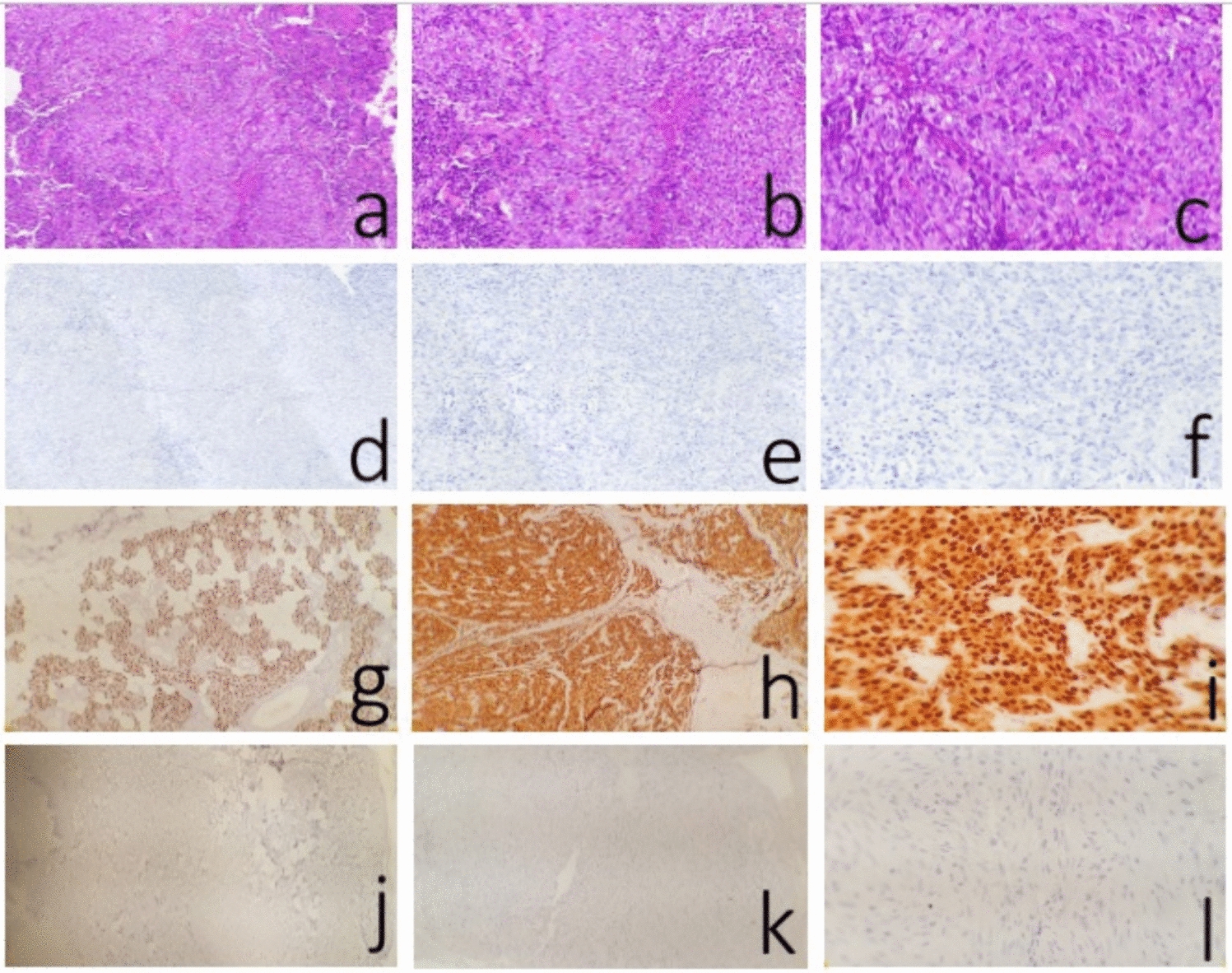
Studies have also identified molecular alterations with potential for prognostic implications. The genes most altered in acinic cell carcinoma of the salivary gland are CDKN2A, PTEN, and TP53. Dogan et al. showed a statistically significant worse prognosis in those patients with CDKN2A/B alterations, with associated higher-grade morphology and increased risk of distant metastasis [18]. A study demonstrated that over 90% of acinic cell carcinoma cases contain translocation t(4;9) (q13; q31), resulting in the upregulation of nuclear receptor subfamily 4 group member 3 (NRA4A3) [7, 17]. This transcription factor can be detected using an antibody to neuron-derived orphan receptor 1 (NOR-1), which showed strong nuclear staining in our case. However, currently there are no available therapies targeting this molecular alteration.
In our case, the patient’s metastatic acinic cell carcinoma was found to harbor a BRAF mutation, which occurs in approximately 4–5% of all acinic cell carcinomas. This molecular alteration offers the opportunity to use a BRAF inhibitor for treatment; however, the prognostic or therapeutic value of BRAF mutations has not been established in acinic cell carcinoma [18]. The 10-year survival of acinic cell carcinoma drops from 99.15% (local disease only) to 31.52% with distant metastasis [19]. Thus, distant metastasis of acinic cell carcinoma is a significant poor prognostic factor for this disease.
Due to the rarity of metastatic salivary gland cancers, there are no large clinical trials to determine the optimal treatment. Vidyadhara et al. detail a case of simultaneous metastasis of acinic cell carcinoma to the lymph nodes, lungs, and spine, and suggest the importance of postoperative radiotherapy if there is incomplete resection of the primary tumor [8]. A study of 301 patients undergoing excision of major salivary glands for cancer at Memorial Sloan-Kettering between 1985 and 2009 showed 20% of salivary gland carcinomas had distant metastasis with most being to the lung (49%) or bone (40%) [4]. In this study, 16% of acinic cell carcinomas developed distant metastasis.
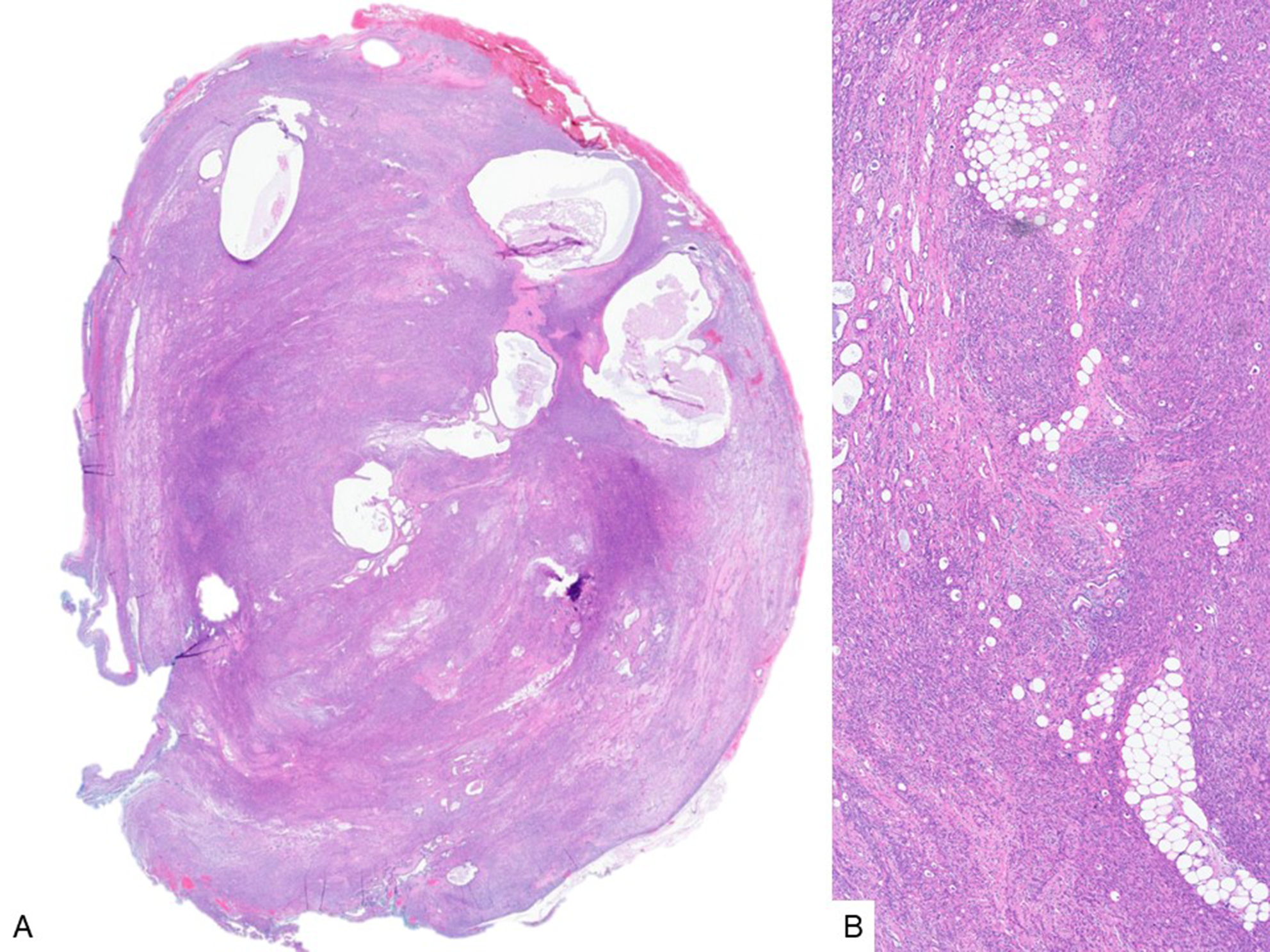
The heart’s unique lymphatic organization protects it from metastasis. Still, metastatic disease is more common than primary tumors of the heart [20]. Metastases are the most common neoplasms of the heart with an incidence between 1.5 and 20% among autopsies of cancer patients [21, 22]. Tumor spreads to the heart via direct spread, bloodstream, lymphatics, and intracavitary migration through the pulmonary veins. Some tumors have displayed higher rates of metastasis to the heart, such as melanoma and mediastinal primary tumors [20]. Metastasis of salivary gland carcinomas to the heart is particularly rare. A few cases of metastatic epithelial-myoepithelial carcinoma of the parotid gland to the heart have been reported [23]. Buchanan et al. describe a case of a woman with metastasis of epithelial myoepithelial carcinoma of the parotid gland to the right heart, which was identified by transthoracic echocardiography [23]. Kishida et al. describe a case of metastatic mucoepidermoid carcinoma to the heart [24]. Foglietta et al. present a case of polymorphous adenocarcinoma of the minor salivary glands with metastasis to the right ventricle [21]. Table 1 provides a summary of prior literature describing salivary gland carcinoma metastasis to the heart.
Table 1 Summary of prior literature on salivary gland carcinoma metastasis to the heartTo our knowledge, this case report is the only published account of a case of acinic cell carcinoma metastasis to the heart. Due to the significant prognostic significance of distant metastasis in salivary gland carcinomas, this is a unique case of a patient that presented with metastasis to the heart 8 years after initial diagnosis. Because of the rarity of these cases, it is important to highlight the disease course in cases of salivary gland carcinoma with distant metastasis.
In conclusion, conventional acinic cell carcinoma is typically of low aggression; however, in cases of acinic cell carcinoma with high-grade features, such as tumor necrosis or high mitotic index, there is increased risk of distant metastasis. Definition of high-grade features of acinic cell carcinoma can help to stratify patient’s risk to identify patients more likely to have distant metastasis.



Comments (0)