In general, various factors influence how information technology is used in healthcare organizations, just like in any other business. Appropriate tactics must be considered to address the obstacles and make technology implementation easier. Among these tactics, the human-related aspects, like users’ perceptions and knowledge of technology, are crucial. Users’ favorable opinions of technology might make information technology adoption go more smoothly and effectively [22].
4.1 The practice of telemedicine
In the current study, approximately 50% of physicians used telemedicine. Of these, around 70% mainly used text messages like WhatsApp, followed by phone calls and video conferences. Similarly, nearly 72% of Saudi Arabian professionals always communicate with patients via social media or email [20].
During the COVID-19 pandemic, a variety of guidance and tools emerged for the scale-up of telemedicine services. Across this time span, population knowledge and learning have expanded significantly; this has led to optimizing the implementation of telemedicine services [23]. A US study revealed that 73.8% of oncologists were satisfied with the adoption of telemedicine, and after the COVID-19 pandemic, this percentage increased to 81.5% [24]. A considerable percentage of our physicians were satisfied with the telemedicine system. In agreement, 78% of the Indonesian clinicians were satisfied with the new type of care [25]. The satisfaction can be attributed to the benefits of digital health technologies, including enhanced access to secondary care advice and guidance, as well as clinical decision support tools, standardized care according to best practices, and automated checks [26]. Most of our physicians (61.2%) who did not practice telemedicine reported that they would like to use telemedicine themselves. In agreement, the majority of Saudi Arabian physicians expressed favorable opinions on telemedicine and expressed a willingness to use it in their clinical settings [20]. Also, in China, most medical professionals and staff were open to implementing and advancing telemedicine technology [27].
However, 40% of our physicians also reported problems obtaining consent via telemedicine and with the diagnosis. In concordance, a KSA study in Riyadh reported that about one-half of the doctors thought telemedicine diagnoses were incorrect because there were no physical examinations [28]. Even if technology has made it possible to preserve continuity of care, the “lack of personal touch” is still regarded as a significant disadvantage when evaluating the patient’s clinical state [29].
The current study revealed that male physicians were significantly more users than females. This higher usage among males may be attributed to their greater IT skills and, consequently, higher digital literacy. A South American study supports this suggestion, reporting that males had 3% higher IT skills than females [30].
In our study, the other sociodemographic characteristics exhibited no statistically significant differences between users and nonusers, with nearly the same percentage among both physician groups. However, physicians working in rural areas were slightly more users than urban ones. In agreement, an American study on a nationally representative random sample of 5000 family physicians in primary care showed that rural family physicians were twice as likely to use telehealth as urban family physicians. Rural physicians were more likely to use TM to take advantage of specialist expertise, expand their scope of practice, and reduce the feeling of isolation experienced by rural physicians [31].
Most users were those with “enough and saving income” and the married ones. Senior physicians with more than 10 years of experience were more users. A USA study using the 2021 National Electronic Health Records Survey (NEHRS) dataset concluded that after the COVID-19 pandemic, the majority of professionals regardless of their socioeconomic status have begun integrating telemedicine into their daily routines because, in the first place, technology enables doctors to provide care across geographic boundaries and reach a larger patient population, including those with restricted access to healthcare services. Also, doctors may serve more patients in less time, optimize scheduling, and enhance workflow by using virtual consultations to reduce the time spent on in-person visits. In addition, telemedicine may make it possible for doctors to keep an eye on their patients from a distance. This would allow for proactive and ongoing care management, which might result in early health problem diagnosis, prompt interventions, and better patient outcomes [32].
Our surgical specialists were more users than medical. In contrast, studies reported wide use of telemedicine among medical specialties as [33, 34]. However, telemedicine can be applied to surgical care in various ways. Surgeons can use telehealth to conduct pre- and postoperative surgical consultations, administer remote monitoring, and provide surgical education [35].
At the employees’ level, our results demonstrate that 38.2% of the employees have used telemedicine, and 63.1% expressed a willingness to use it in the future. In agreement, telehealth services were utilized by 35.1% of Egyptians overall, and 43% expressed willingness to use them again [7].
Our results concluded that 71.7% rated their experience with telemedicine as acceptable and 23.6% as good. An Australian survey study recorded similar findings, with 61.9% of respondents stating they had a “better” experience implementing telemedicine than the conventional medical appointment scheduling system [36].
The current results revealed that most of our employees rated the time given by their healthcare provider during a tele-visit as acceptable. Most participants reported that the doctor helped them easily understand the instructions, their privacy was respected while using telemedicine, and they were satisfied with the doctor they dealt with and the doctor’s treatment. More than half of the participants would recommend telemedicine to a friend or family member. In agreement, in a 2022 study conducted in the USA, patients’ experiences with telehealth appointments were just as good as or better than those of regular office-based visits. Tele-video visits were thought to be substantially better than office visits in terms of reports on doctor communication, care coordination, global rating, and referrals to family and friends [37]. Similarly, over 80% of Pakistani patients expressed satisfaction with their interactions with doctors via telemedicine [38]. Digital health technologies (DHTs) contribute to increased patient satisfaction and trust, particularly when dealing with sensitive medical circumstances (such as sexual or mental health difficulties) [39].
At the employee’ level, a statistically significant difference was observed between users and nonusers of telemedicine regarding residence, where urban users were more than rural. In addition, enough income and better Internet use skills had a significant effect. Our findings align with the concept of the “digital divide,” which describes the disparity between populations with and without access to contemporary communication and information technology [40].
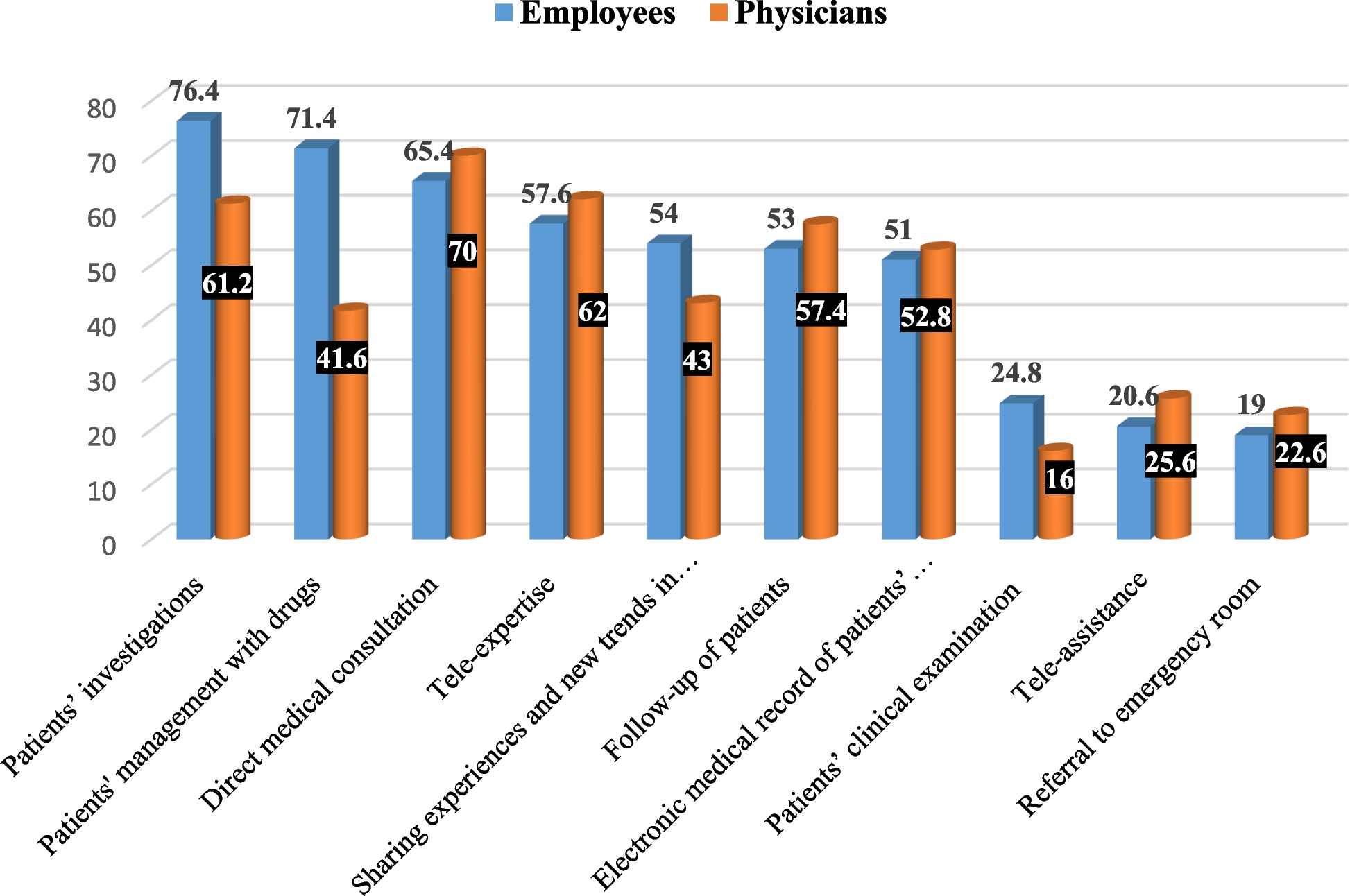
Applications of telemedicine from the perspective of the employees included patients’ investigations communicated through the Internet, patients’ management with drugs, direct medical consultation between patient and physician, second opinion consulting (tele-expertise), sharing experiences and new trends in medicine in surgery with specialists in other countries, and follow-up of patients through the electronic technologies. In agreement, an Egyptian study reported that Egyptian patients used telemedicine mainly to follow up on their laboratory results [21]. In China, teleconsultation, remote education, telediagnosis of medical pictures, tele-electrocardiography, and telepathology were the top 5 telemedicine services used in China’s tertiary hospitals [41].
4.2 Attitude regarding telemedicine
Our results revealed that about three-quarters of physicians had a positive attitude toward telemedicine. In concordance, the Saudi Arabian participants’ attitudes toward telemedicine were generally favorable [42]. Also, most of the Chinese study participants supported the new medical development [27].
At the employees’ level, they believed telemedicine saves efforts and money and provides better access to remote and underserved areas of healthcare. In agreement, an Egyptian study reported that more than half of the Egyptian participants thought that telehealth services may save them money and time [7]. Additionally, our results are in line with another Egyptian study conducted in the University Teaching Hospitals of eight governorates, which revealed that 73.5% of participants agreed or strongly agreed that telehealth can reduce hospital waiting lists, save time and money and transportation expenses, and provide speedier medical care [21].
4.3 Knowledge about telemedicine
The advantages reported by physicians in this study include being easy to use, reducing patient travel costs, and increasing importance during pandemics, e.g., COVID-19. In agreement, the Indonesian clinicians reported obtaining faster diagnoses, decreasing needless referrals, enhancing the skills of healthcare professionals, and boosting patient trust [25]. In the USA, the use of preoperative telemedicine consultations in an academic medical center in Los Angeles, CA, USA, resulted in a low case cancellation rate, high patient satisfaction, and patient cost savings [43].
At the employee level, increasing accessibility through digital health technology could be a key subject, particularly for hard-to-reach groups and during pandemics, as a means to guarantee continuity of care and accessibility [39].
However, our results indicated some potential barriers when using telemedicine, including the need for training for physicians and patients; some patients, especially the old ones, find difficulty dealing with technology; poor infrastructure and technical issues; and, lastly, the difficulty for patients in expressing their feelings and communicating with physicians and a lack of body language. In agreement, the implementation of telemedicine in Libyan hospitals is adversely affected by the lack of human resources, inadequate infrastructure, training requirements, and financial concerns [19]. Also, in Saudi Arabia, the primary concerns with telemedicine adoption are patient privacy, the high expense of equipment, inadequate training, and a lack of communication between clinicians and IT specialists [20].
Poor digital literacy and the possibility that DHTs would deepen current disparities and widen the digital divide are the primary weaknesses. The best people to benefit from the increasing number of DHTs being introduced are those who live in wealthy cities and have greater levels of education, health consciousness, and digital literacy. However, underprivileged rural populations, who stand to benefit the most from remote care tools, frequently are not able to make the most of them [44].
About one-third of our participants reported barriers regarding privacy, data security, and ethical concerns. Because sensitive health data is vulnerable to hackers, digital health presents significant privacy and security challenges. The possibility of data exploitation or misuse for purposes other than healthcare was one of the ethical issues that DHTs brought. This raises concerns about data ownership and whether patient consent was obtained [45].
Our findings were in line with another study conducted in Syria, which revealed a significant positive correlation between practice, knowledge, and attitude toward telemedicine [3]. In an exploratory study of telehealth utilization among the Egyptian population (2023), telehealth use and attitude showed a statistically significant positive association, indicating that as telehealth use increased, so did positive attitudes toward telehealth services [7].
Our results show that the main sources of information about telemedicine among physicians were the Internet, colleagues, and conferences. An Iranian study (2023) concluded that the most common sources of information on telemedicine are coworkers, continuing education, social media, and the Internet [46].
4.4 Study limitations
Our study’s cross-sectional methodology and convenience sampling technique make it impossible to draw firm conclusions about the relationships between the variables. Furthermore, our study did not include information about the various disorders that are best treated by telemedicine. Our study also does not inquire about the kinds of telemedicine technology, how they might be used, or how patients feel about telemedicine. We also conducted our research in Egypt, a developing nation. Therefore, the challenges we found might not apply to countries in other regions of the world and at various developmental stages. Further studies on telemedicine are necessary to provide patients with qualitative measurements of the quality of medical care they receive, evaluate the availability of healthcare services in other transitional nations, and determine whether these telemedicine adaptations are advantageous to patients, particularly those with mental health disorders and chronic illnesses. Additionally, it is necessary to assess whether these services require modification and to analyze their cost–benefit ratio.


Comments (0)