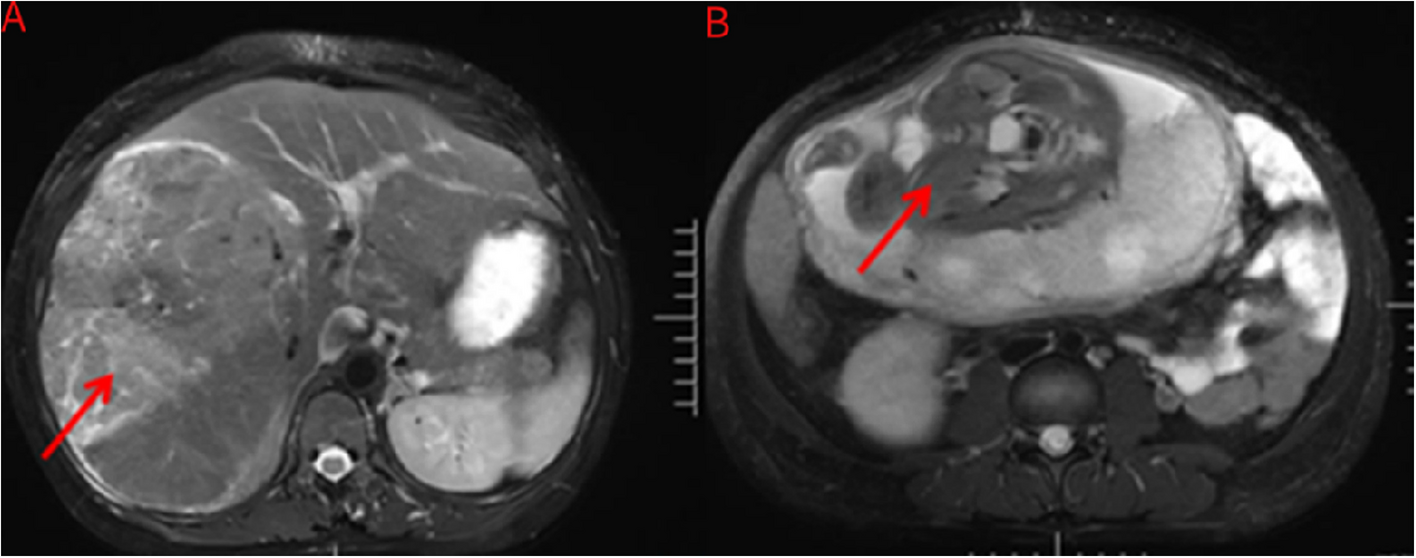
The early diagnosis of HCC during pregnancy poses significant challenges due to its insidious onset. Implementing multiple auxiliary examinations for pregnant patients can enhance the detection rate of HCC. To mitigate potential adverse effects of radiographic imaging on the fetus, B-ultrasound and MRI are considered optimal modalities for preoperative diagnosis of hepatocellular carcinoma in this population. In this case report, the patient underwent an abdominal ultrasound, which revealed a large HCC. Subsequently, abdominal CT and MRI were performed. These imaging techniques proved valuable in determining the origin of the HCC, assessing the extent of tumor invasion, and facilitating differential diagnosis from various organ tumors.
Several studies have shown that pregnancy clearly has an adverse effect on the prognosis of HCC [6,7,8]. HCC becomes more aggressive during pregnancy, primarily due to two main etiologies: estrogen elevation and immune suppression during pregnancy. Accordingly, estrogen has been demonstrated to enhance hepatocyte mitosis, increase hypervascularity, and elevate free radical levels. Additionally, it may reactivate the hepatitis B virus and diminish humoral immunity. During pregnancy, large amounts of human chorionic gonadotropin, estrogen, and placental lactogen secreted from the placenta are believed to promote the growth and reproduction of cancer cells, thus aggravating the aggressiveness of the underlying HCC [9]. Moreover, gestational immune suppression may be an enabling factor for tumor progression [10]. Thus, the pregnancy was terminated as soon as possible for hepatocellular carcinoma patients.
We performed a systematic literature search spanning from database inception to 2024 across four biomedical databases (PubMed, MEDLINE, Embase, Cochrane Library). The search protocol utilized Boolean logic to combine MeSH terms and title keywords: (pregnancy (Title) AND “hepatocellular carcinoma” (MeSH Terms)) OR (“hepatocellular carcinoma” (Title) AND pregnancy (Title)). Our systematic review of literature since 2010 (summarized in Table 1 [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]) revealed two critical findings: First, no documented cases exist of late-pregnancy HCC patients surviving beyond 2 years post-surgical resection. Second, comparative analysis with historical case reports demonstrates that delayed diagnosis and subsequent surgical intervention in pregnancy-associated HCC correlate with significantly reduced survival durations. Notably, our current case exhibits distinct clinical characteristics when juxtaposed with previously reported cases.
Table 1 The reports of hepatocellular carcinoma during pregnancyA staged surgical treatment protocol was performed based on the Barcelona Clinic Liver Cancer (BCLC) staging classification. The option of termination of pregnancy: fetus could not survive if the gestational week of less than 28 weeks; the fetus could survive if the gestational week of greater than or equal to 28 weeks, the patient underwent emergency cesarean section for huge HCC. In this case report, the cesarean section was performed at 34 weeks. Our case represents a unique clinical scenario in three aspects: First, the patient achieved the longest reported survival (2 years) following HCC resection during late pregnancy. Second, the combination therapy of Sintilimab and Lenvatinib post-surgery may have contributed to sustained remission, as evidenced by the absence of recurrence on imaging. Third, we introduced a mental health team during the entire surgery process—they used CBT to manage anxiety before surgery and provided emotional support after operations. This whole-person care method hasn’t been routinely used in previous cases like this.
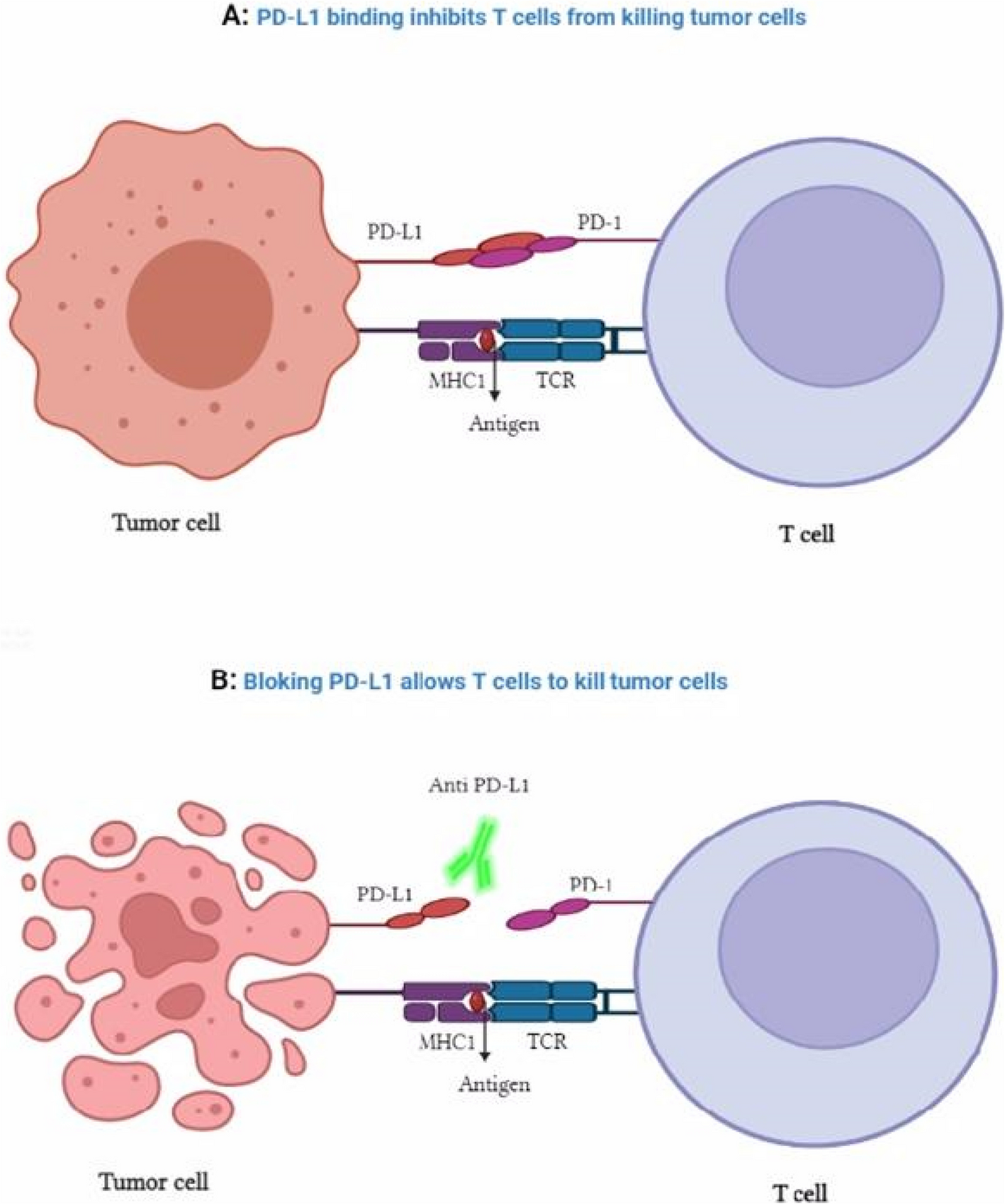
Sintilimab, a PD- 1 inhibitor, functions by blocking the PD- 1/PD-L1 signaling axis to reactivate T cell-mediated antitumor immunity. Lenvatinib, a multitargeted tyrosine kinase inhibitor, suppresses tumor angiogenesis and proliferation through inhibition of VEGFR, FGFR, and PDGFR pathways. Preclinical studies demonstrate that lenvatinib enhances intratumoral CD8 + T cell infiltration while reducing immunosuppressive regulatory T cells, creating an immunologically favorable microenvironment that potentiates PD- 1 inhibitor efficacy. This synergistic mechanism translates to significant survival benefits in advanced HCC, with combination therapy demonstrating superior progression-free survival and overall survival compared to monotherapies [27]. The 2024 guidelines endorse targeted-immunotherapy combinations (PD- 1 inhibitors + TKIs) as a promising adjuvant strategy following surgical resection, particularly for high-risk HCC cases with vascular invasion or suboptimal tumor differentiation [28]. The support and assistance provided by the clinical psychology team during this time play a crucial role in the overall treatment and rehabilitation of patients. Preoperatively, patients may experience anxiety and depressive symptoms due to fears and concerns regarding the surgery. The clinical psychology team assesses the psychological state of these patients and offers appropriate interventions, such as CBT, to help alleviate preoperative anxiety and enhance their confidence and preparedness for the procedure. Postoperatively, patients might face psychological issues stemming from pain at the surgical site, uncertainties about recovery, or worries about disease prognosis. The clinical psychology team can assist by managing pain effectively while providing emotional support that allows for emotional expression, thereby facilitating psychological recovery in these individuals [29]. Our research findings suggest that the presence of well-differentiated tumor characteristics in patients, combined with proactive and appropriate treatment strategies, as well as the involvement of a clinical psychology team in the therapeutic process, significantly contributes to achieving favorable clinical outcomes. Consequently, this approach has led to a notable extension of survival time for patients during late-stage pregnancy compared to other patients.
Our study has limitations inherent to single-case reports. The absence of long-term follow-up beyond 2 years precludes definitive conclusions about cure rates. Additionally, the role of adjuvant Sintilimab-Lenvatinib therapy in pregnancy-associated HCC requires validation through larger cohorts, particularly given potential safety concerns in postpartum women. Finally, the impact of psychological interventions, while promising, warrants standardized assessment tools to quantify their contribution to survival.


Comments (0)