Although oral cancer is one of the diseases that can be detected in the early stage through routine clinical examination of the accessible oral cavity, most of the cases are recognized in the late stages of the disease [14]. Early detection of oral cancer would result in more efficient and timely management and is considered a key factor in reducing the mortality and morbidity of oral cancer. Dentists can play a major role in implementing oral cancer detection and prevention measures that could improve the survival rates of oral cancer patients [19]. However, inadequate knowledge regarding oral cancer has been widely documented in current research among general dental practitioners from developed and developing countries [16]. Moreover, a lack of awareness of oral cancer risk and clinical signs may prohibit dentists from delivering preventive advice [19].
Thus, the current investigation was intended to assess the level of awareness, knowledge, attitude, and practice towards oral cancer among Egyptian dentists. An anonymous questionnaire was used to encourage the participants to express their actual behavior regarding the different questionnaire items. This had an impact on the reduction of information bias.
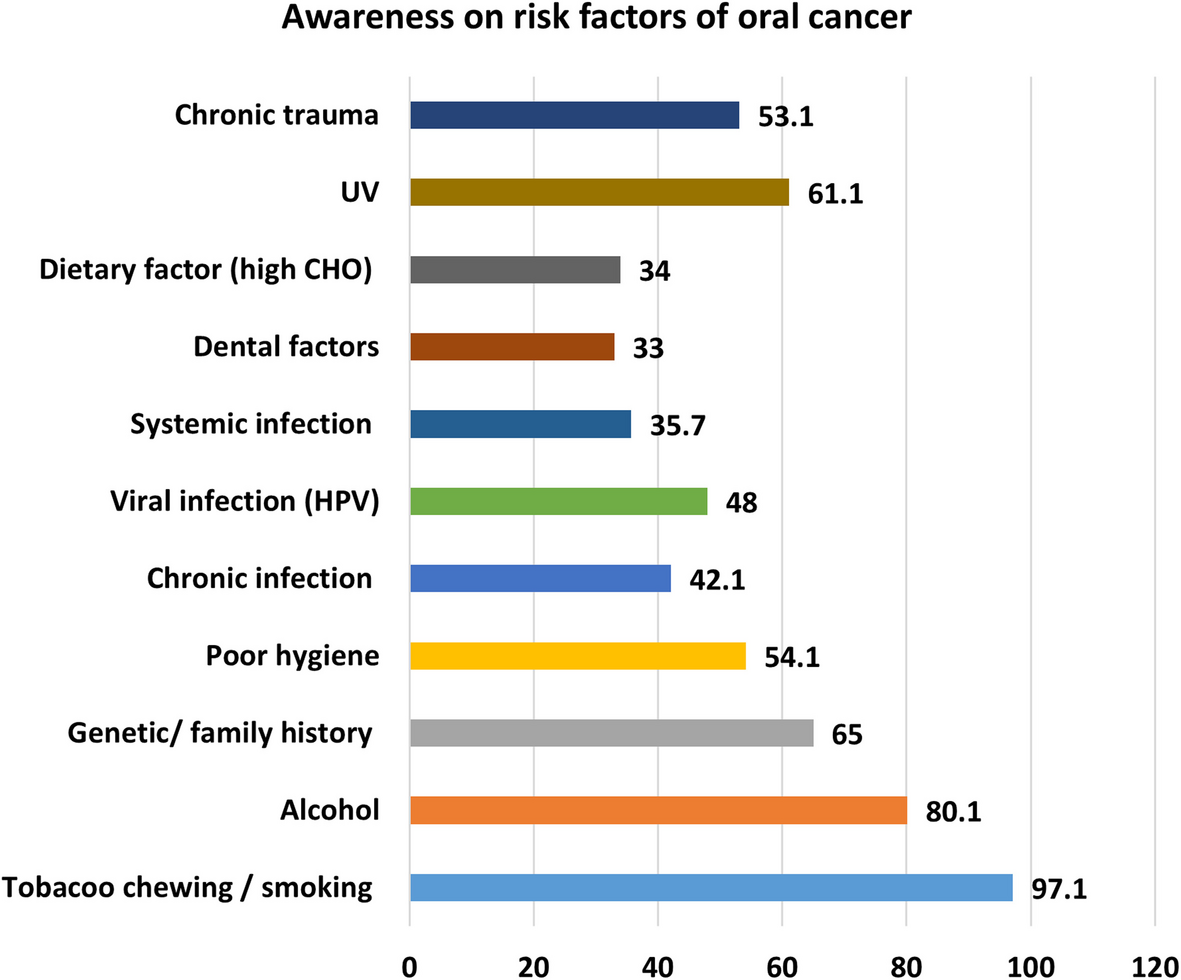
In the current study, data concerning awareness of oral cancer risk factors revealed that 97% of participants believed that the risk of getting oral cancer increases with increasing age, Additionally, tobacco chewing/smoking, alcohol consumption, and family history were the commonly recognized risk factors of oral cancer by 97.1%, 80.1%, and 65% of participants respectively. Tobacco use is the most important risk factor for oral cancer [20], and its identification by the majority of participants points out that their knowledge is consistent with the contemporary understanding of the etiology of oral potentially malignant and malignant lesions reported by several studies [11, 21, 22]. However, other factors such as viral infections, dietary factors, bad oral hygiene, and dental and systemic factors were not acknowledged beyond one-third of the participants. Thus, although 82% of participants recommended that dentists should warn their patients to avoid OC risk factors, this percentage is not as impressive as it would seem because a smaller percentage of dentists appeared to be aware of the whole range of risk factors to give their patients comprehensive advice. It is well-established that oral cancer is largely related to lifestyle, and as healthcare providers, dental practitioners should be well aware of these factors and play a central role in providing information about the benefits of changing lifestyle habits [7, 11, 23]. Also, defining the patients at risk is important as an alert for more careful examination and follow-up. Awareness of the clinical presentations of oral cancer showed that the most acknowledged clinical presentations by the participants were non-healing ulcers (85%), red lesions (84.1%), white lesions (81,1%), and induration (71%). Such results were encouraging as they conformed to previous literature [24].
Data regarding the general attitude among studied participants displayed that 92% of them acknowledged the important role of dentists in the early detection of oral cancer, however, only one-third of participants declared their routine examination of lymph nodes. Also, a similar percentage reported routine screening of the oral mucosa for signs of OC. These two responses look contradictory. Although most of the participants declare the importance of the dentist’s role in the early detection of oral cancer, we find a good percentage refraining from screening and lymph node examination. This highlights the practitioners’ lack of ability or motivation to carry out the screening [25]. Lack of training and lack of confidence could be the underlying causes. Unfortunately, these shortages in knowledge and practice are a real threat to the prevention and early detection of the disease and subsequently reducing its burden, considering that the majority of the global burden of oral cancer lies in the developing world [2, 3]. Similar findings have been reported in previous research [12, 26, 27]. Therefore, educational strategies should be aimed at providing current information on oral examinations, diagnostic techniques, and conditions associated with oral cancer. The proof for such an assumption came from the present results, where 25% of participants believed they were poorly informed about the prevention and detection of oral cancer, 58% of participants believed they were adequately informed, and only 17% thought they were well informed. In addition, 99% of participants thought that oral cancer awareness campaigns were needed and would be effective.
Sixty-nine percent of participants considered the tongue a high-risk site, followed by the floor of the mouth and the buccal/lip mucosa. This is in accordance with most available literature [28,29,30].
The relation between years of practice and OC awareness revealed significant differences between the categorized participants, mostly in favor of older groups. This was in some instances, logical as the questions around previous detection of oral potentially malignant and malignant lesions and taking biopsy, all of which can be more experienced with a longer duration of practice. However, it was so discouraging when the youngest group failed to practice oral screening, lymph node examination, and other skills that they have been recently taught as they have recently graduated, and nowadays, much care is put into inserting OC-related information and practice within undergraduate curricula. One of the important points showing no significant difference between groups with varying periods of practice was that dentists have an important role in the early detection of signs and symptoms of oral cancer, where all groups showed high percentages of approval, thus confirming a general consensus. Dental practitioners are in an ideal position to help people quit smoking because they are among the few healthcare professionals who routinely see “healthy individuals” [12]. Saleh et al. [20] found that many dentists were uncomfortable discussing OC risk habits with their patients and commented that this scenario was not unique to Malaysia [20]. Studies in the United Kingdom and European Union reported that most dentists do not determine their patients’ tobacco habits and provide cessation counseling [27,28,29], whereas, in the United Kingdom, only 30% of dentists provide brief cessation advice to their patients. A similar situation was reported in the United States of America, where 60% of dentists do not routinely advise tobacco users to quit [31].
Previous research presented ideas regarding undergraduate teaching of screening for OC and oral potentially malignant diseases (OPMDs), aiming at increasing awareness and skills among graduated dental practitioners. Great scenarios were discussed, including problem-based learning, clinical case presentations, and virtual learning (which can compensate for the limited number of cases), besides the didactic part [32]. However, all suggestions were focused on Oral Pathology and Oral Medicine curricula. Although the described methods of teaching with all details included seemed outstanding [32], making it part of Oral Pathology and Oral Medicine curricula only makes it vulnerable to be considered by students as just a chapter in these curricula to be studied for the exams and then totally forgotten. Whether in Cairo University or the British University in Cairo, as well as in most dental schools in other Universities in Egypt, Oral Medicine curricula contain a limited part dealing with early detection of oral cancer. There is one lecture dedicated to the topic, including all techniques used up to date, and then in the clinics, only 20% of the sessions are dedicated to the skills required for screening for oral cancer, ending in a clinical assessment. Oral Pathology curricula have single chapters dedicated to oral cancer, of course, without any clinical application and without integration with Oral Medicine or Oral Radiology in that regard.
Actually, we need the practice of screening for OC and OPMDs to reach the level of skills that dentists acquire in general dental specialties, such as conservative and prosthodontics dentistry and exodontia. This necessitates a vertical distribution throughout all academic years with a merge from a preclinical to a clinical level, followed by scheduled practice during the internship year. Hence, we need an early start, perhaps with the curricula of general pathology and general surgery, where the process of carcinogenesis can be taught with reference to both its histopathology and clinical presentation through all its different stages till it reaches its full-blown picture of malignancy with its diverse forms and levels of differentiation. Then comes the part to be played by Oral Pathology and Oral Medicine staff. However, these two specialties are not to do it individually; it should take the form of integrated sessions, together with Oral and Maxillofacial Radiology and Oral and Maxillofacial Surgery staff. Throughout these sessions, risk factors, methods of screening, investigations, diagnosis, case referral protocols, and every single thing related to OC and OPMDs should be taught and supplemented with clinical practice [33]. Then comes the role of public health, where curricula should include an integral part related to tobacco cessation strategies, which should be practiced by students. Also, methods related to persuading patients’ persuasion into more healthy lifestyles and the evasion of all potential risk factors should be included. Students should be properly instructed that patient education concerning risk factors is one of the main duties of a dental practitioner. The internship year should include one whole round for practicing all that is learned before graduation, equivalent to practicing other dental specialties. After that, continuous education programs should always include workshops for the early detection of OC and OPMDs and implementing strategies to develop motivation and self-learning [34]. There should be an assessment for skills and competencies gained in this context held simultaneously during practice license exams for new graduates. An audit can even be added at the time of license renewal. This should be generalized, not only applied by some institutes and leaving out the rest. Ramirez-Amador et al. have even recommended the exchange of ideas and experiences among different countries to reach a unified, effective, and internationally accepted curriculum aiming at solid knowledge, awareness, and skills related to a very important competency, which is oral cancer early detection and dealing with any carcinogenic process in the oral cavity [32].
The primary limitation of this study is the study population, which was comprised mainly of dentists from Cairo. A future study should expand to include other dental schools and other areas of Egypt, as well as other oral health care providers in private clinics for a more comprehensive sample. Another possible limitation is the tendency of dentists to provide acceptable answers, which may differ from what they actually do, and this might bias the outcome. However, the anonymous nature of the questionnaire should have minimized this type of information error.


Comments (0)