Study design and participants
The methods of UPBEAT have been published previously [17]. In brief, between March 2009 and June 2014, 1555 women were recruited with maternal age ≥16 years, singleton pregnancy at 15+0-18+6 weeks’ gestational age, and body mass index (BMI) ≥ 30 kg/m2; women were excluded if they were taking metformin, or had diabetes mellitus or another condition (e.g., chronic hypertension currently treated with antihypertensive therapy) that increased the risk of adverse pregnancy outcomes. One participant was excluded after enrolment in another trial.
Intervention
Following written, informed consent, women were randomised to a complex behavioural intervention, focusing on a healthy diet and physical activity, or to standard antenatal care.
Outcomes and data collection
Antenatal registration data (including measurement of BP and proteinuria) were recorded from clinical records. Study visits were conducted at trial entry between 15+0-18+6 and then again at 27+0-28+6, and 34+0-36+6 weeks’ gestation, including blood collection for cardiovascular markers.
BP was measured according to a standardised protocol, using the automated Microlife BP3BTo-A BP monitor (Microlife, Widnau, Switzerland) validated for use in pregnancy and pre-eclampsia [18], with an appropriately-sized cuff. The last BP before delivery was recorded from clinical records.
The co-primary outcomes were gestational diabetes mellitus (GDM) and large-for-gestational age infants of which neither differed between trial arms, although the intervention (vs. usual care) resulted in less gestational weight gain and more physical activity [16].
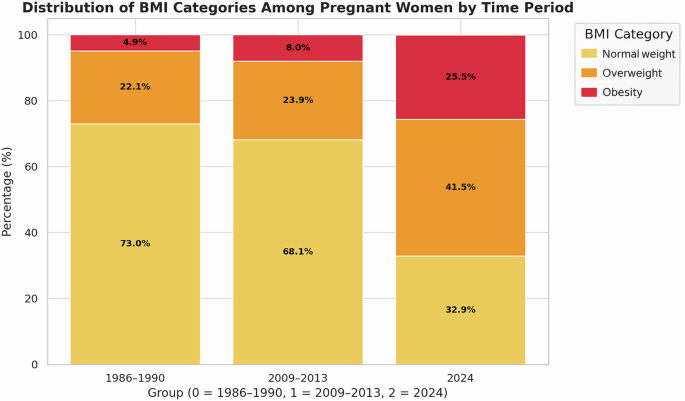
Outcomes were abstracted from clinical records after birth. Pre-eclampsia was defined as gestational hypertension (i.e., systolic BP [sBP] ≥140 mmHg or diastolic BP [dBP] ≥90 mmHg, measured twice, at least four hours apart at ≥20 weeks) and new-onset proteinuria (i.e., ≥300 mg/24 h, dipstick proteinuria ≥2+, or a spot urine protein:creatinine ratio ≥30 mg/mmol) [16]. The World Health Organisation (WHO) classifies obesity as a BMI ≥ 30 kg/m2, with obesity further subdivided into obesity class I (BMI 30–34.9 kg/m2), obesity class II (BMI 35–39.9 kg/m2) and obesity class III (BMI ≥ 40 kg/m2) [19].
Ethical approval for UPBEAT was granted by the NHS Research Ethics Committee (reference 09/H0802/5). All methods were performed in accordance with the relevant guidelines and regulations.
This secondary analysis
Use of UPBEAT data for this project was approved by the UPBEAT Scientific Advisory Committee (Research Application Form reference 077). In this analysis, we included UPBEAT participants with data on BP from at least one study visit and the adverse pregnancy outcomes of interest. We sought to investigate whether adjusting BP thresholds for pregnant women with obesity would improve the prediction of adverse maternal and perinatal outcomes.
BP was classified according to the highest antenatal BP, using 2017 ACC/AHA criteria: ‘Normal’ (sBP <120 mmHg and dBP <80 mmHg). ‘Elevated’ (sBP 120–129 mmHg with dBP <80 mmHg), ‘Stage 1 hypertension’ (sBP 130–139 mmHg and/or dBP 80–89 mmHg), and ‘Stage 2 hypertension’ (sBP ≥140 mmHg and/or dBP ≥90 mmHg). ‘Stage 2 hypertension’ was further categorised into ‘non-severe’ (sBP 140-159 mmHg and/or dBP 90-109 mmHg) and ‘severe’ (sBP ≥160 mmHg and/or dBP ≥110 mmHg).
The main outcomes of interest were preterm birth (PTB), postpartum haemorrhage (PPH), birth weight <10th centile (small-for-gestational age, SGA), and neonatal intensive care unit (NICU) admission; none of these differed by trial arm in UPBEAT [16]. PTB was birth at <37+0 weeks’ gestation. PPH was an estimated blood loss ≥1000 mL. The following maternal core outcomes in hypertensive pregnancy were unavailable: stroke, eclampsia, blindness, pulmonary oedema, respiratory failure, hepatic haematoma or rupture, acute kidney injury or dialysis, elevated liver enzymes (aspartate or alanine transaminase >40IU/L), platelet count <100 × 109/L, and intensive care unit admission. The following fetal/neonatal core variables were unavailable: respiratory morbidity.
For each trial participant, maximum antenatal BP was categorised according to the 2017 ACC-AHA criteria. Baseline demographics and past medical and obstetric history were summarised for the trial cohort overall, and according to the ACC-AHA BP categories; frequencies and percentages were used for categorical variables, and medians and interquartile ranges (25th, 75th centiles) for continuous variables.
Statistical analysis
To assess the association between maximum BP and adverse pregnancy outcomes, we calculated adjusted risk ratios (aRR) using robust Poisson models. Confounders were: maternal age (yr), BMI (kg/m2), ethnicity (White British, Black, Asian and Other), parity (nulliparous/multiparous), smoking status (yes/no to ongoing in current pregnancy), alcohol use (yes/no to ongoing in current pregnancy), previous pre-eclampsia, and previous GDM; these were selected as variables related to BP level and outcomes, without being on the causal pathway.
The relationship between BP category and adverse outcomes were assessed in two ways. First, each BP category was treated as mutually exclusive from the others, and the risk ratio (RR) and 95% confidence interval (CI) [20] was calculated for each BP category relative to ‘Normal’ BP, using generalised estimating equations with a Poisson link function [21]. Second, analogous models were fit, but the lower limit of each category was treated as a BP cut off for the diagnosis of an abnormal BP, in the way that 140/90 mmHg is currently used; for example, for ‘Stage 1 hypertension’, the RR for each outcome was compared for women with sBP ≥130 mmHg and/or dBP ≥80 mmHg, and women with sBP <130 mmHg and dBP <80 mmHg. This analysis was repeated, adjusting for UPBEAT trial intervention group, maternal age, BMI at booking, ethnicity, parity, smoking status, alcohol use, previous pre-eclampsia, and previous GDM.
Also, for each new threshold for abnormal BP, diagnostic test properties were assessed, using sensitivity, specificity, and positive and negative likelihood ratios (+LR and -LR respectively). +LR was calculated as sensitivity/, and -LR as /specificity. LRs were considered diagnostically useful if +LR were ≥5.0 or -LR were <0.2 [22].
A sensitivity analysis was undertaken, restricting analyses to BP measurements taken under standardised conditions at study visits (and excluding BP measurements taken in routine clinical care, at antenatal care booking and again close to birth). We examined the impact on the association of each BP category (vs. ‘Normal’ BP) with adverse outcomes, as well as the diagnostic test properties of the BP threshold associated with each category.
All analyses were undertaken using R statistical software, with 95% confidence intervals (CIs) considered significant if they did not cross 1.0. No adjustment was made for multiple comparisons. As a secondary analysis of an existing dataset, no sample size calculation was undertaken.

Comments (0)