
Remember me
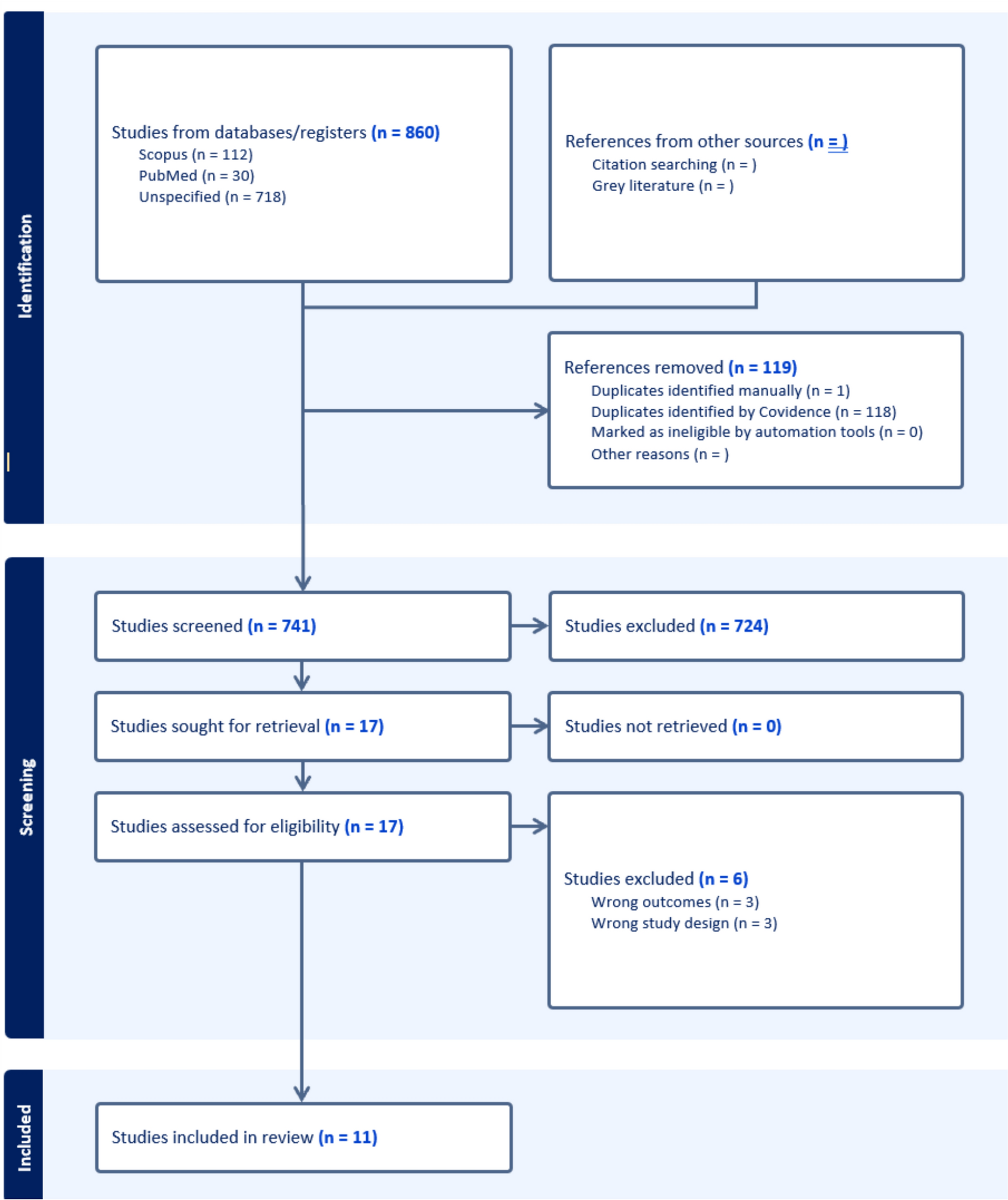

The search resulted in the identification of 860 articles. Following the removal of duplicates, 741 studies underwent title and abstract screening, of which 17 studies were deemed relevant. Of the 17 studies, 11 studies were eligible to be included in this review (n = 11) (Table 2). Studies were excluded due to not reporting suicide outcomes (n = 3) or due to incorrect study design (i.e., editorials, qualitative studies) (n = 3). The component studies consist of 2 case–control studies, 3 cohort studies, 4 cross-sectional studies, and 2 chart review studies. See Fig. 1 for further information on the study screening process.
Table 2 Characteristics and Main Results of Included StudiesFig. 1
Study Screening Process. Study screening and figure generation was conducted on Covidence
Risk of bias resultsWhen considering the case–control studies, both studies received a quality rating of “good” and were deemed to have a low risk of bias; however, one area of concern was not reporting a sample size justification (Supplementary Table 1) [2, 17]. From the cohort and cross-sectional studies, four studies received a quality rating of “good” while the other three were “fair” (Supplementary Table 2). Some concerns were similar to the case–control studies wherein sample size justifications, power descriptions and effect size estimates were not provided [6, 11, 13, 35, 39]. An additional domain that may introduce a potential bias is inadequate reporting of the blinding integrity of the assessors, which was present across all of the cohort and cross-sectional studies. Two included studies are chart reviews, which could not be evaluated for their risk of bias as there is no validated and established risk of bias tool designed to assess chart review studies [20, 36]. However, an area that may introduce potential bias is adequately reporting sample selection and inclusion criteria as well as choosing an adequate time frame to observe outcomes of interest.
Association of PCOS with suicidality composite scoresWe identified five studies (n = 5) that reported on the association between PCOS and suicidality, but did not disaggregate between the different domains of suicidality investigated (Table 2) [13, 20, 29, 36]. Across the 13,112 participants within the identified studies, mixed results are reporting on suicidality in persons with PCOS. Specifically, Hussain et al. [13] and Scaruffi et al. [35] observed that persons with PCOS had higher rates of suicidal ideation and/or behaviour compared to the control group (8.0–8.18% vs 0–6.0%, respectively),however, the studies did not report on the strength of association of these results.
In contrast, Maya et al. [20] reported suicidality as a composite score of self-harm and/or suicidal ideation history wherein there were nonsignificant differences between persons with PCOS (n = 46) and the control group (n = 447) were observed (OR = 0.86, 95% CI = [0.32, 2.31]); a trend similarly observed by Trivedi et al. [39] (19.6% vs 18.3%, respectively, p = 0.74). Furthermore, when analyzed for the effects of gender on composite scores of suicidal ideation and/or behavior history in persons with PCOS, there were also nonsignificant differences between cisgender and transgender individuals (14.4% vs 36.4%, p = 0.08) [36].
Notwithstanding the mixed results, the presence of at least one psychiatric comorbidity was more commonly observed in persons with PCOS compared to the control group [13, 20, 35, 39]. In general, the most commonly reported psychiatric disorders within the PCOS group were MDD, bipolar disorder and any anxiety disorder (Table 2). As psychiatric disorders are strongly linked to suicide risk, further investigation is required to evaluate the strength of association between PCOS and suicide risk after adjustment for a psychiatric diagnosis.
Association of PCOS with suicidal ideationThree out of eleven of the included studies reported on the prevalence of suicidal ideation in persons with PCOS (Table 2) [2, 11, 41]. The association of PCOS with suicidal ideation was investigated across a total of 792 participants. Notably, Gomaa et al. [11] reported that across 60 participants, there were nonsignificant differences in lifetime history of suicidal ideation between persons with PCOS (43.4%) and non-PCOS (36.7%) participants (p = 0.60). Notwithstanding the nonsignificant difference in suicidal ideation history, the PCOS group had a higher prevalence of MDD diagnoses compared to the control group [11]. Contrastingly, in terms of recent suicidal ideation status, Williams et al. [41] indicate that participants with PCOS were more likely to have recent suicidal ideation compared to the control group (n = 418, t = − 4.21, p < 0.001, 95% CI = [− 0.730, − 0.266], d = 0.45). This was also replicated for current suicidal ideation status when comparing persons with PCOS and non-PCOS participants (11.1% vs 5.6%, respectively) [2]. The studies conducted by Williams et al. [41] and Almis et al. [2] did not measure psychiatric comorbidities in their samples.
Association of PCOS with suicidal behaviourSelf-injuryFrom the included studies, Williams et al. [41] reported on the prevalence of suicidal behavior, specifically non-suicidal self-injury (NSSI), in persons with PCOS compared to non-PCOS individuals (n = 418). While this study did not report on the prevalence of psychiatric diagnoses in their sample, NSSI was significantly more prevalent in the PCOS group compared to the non-PCOS group (t = − 2.04, p = 0.04, 95% CI = [− 0.746, − 0.013], d = 0.22]) [41]. Similar trends were also observed for future suicidal intention (t = − 2.33, p = 0.02, 95% CI = [− 0.598, − 0.051], d = 0.25) [41]. The foregoing result instantiates the need to investigate the prevalence of suicidal behaviour (e.g., self-injury, preparatory acts of suicide attempts, suicide planning, etc.) in persons with PCOS as well as the prevalence of psychiatric comorbidities in these individuals. Therefore, additional large, adequately-controlled clinical trials are required to further evaluate the prevalence and risk of self-injurious behaviours in PCOS populations.
Suicide attemptsFour of the eleven included studies reported on the prevalence and/or the risk of suicide attempts in persons with PCOS compared to controls (n = 476,953) (Table 2) [6, 11, 12, 19]. Individuals with PCOS (n = 49) were reported to have significantly greater odds of suicide attempt history compared to the control group (n = 49) (Odds ratio; OR = 8.3, 95% CI = [1.0, 70]), which may be attributable to the higher prevalence of any major depressive episode (OR = 3.8, 95% CI = [1.5, 8.7]) or recurrent major depressive episodes (OR = 3.8, 95% CI = [1.5, 9.5]) [19]. However, while individuals with PCOS were more likely to have attempted suicide in their lifetime (OR = 1.41, 95% CI = [1.31, 1.52]), Cesta et al. [6] in a retrospective cohort study of 268,235 participants reported that the association was no longer significant after adjusting for psychiatric diagnoses (adjusted OR = 1.05, 95% CI = [0.98, 1.14]). The foregoing result was similarly observed by Gomaa et al. (2023) wherein there was a higher prevalence of MDD in the PCOS group compared to the non-PCOS group; however, no significant difference in suicide attempt history between PCOS and non-PCOS participants (both 6.7%) were observed.
In contrast, in a 16-year follow-up study using a national database (n = 208, 56), Hsu et al. (2024) reported that individuals with PCOS had a higher prevalence of suicide attempts compared to controls (standardized mean difference; SMD = 1.23) and are at a higher risk of future suicide risk (hazard ratio; HR = 8.47, 95% CI = [7.54, 9.51]). Moreover, suicide attempts were found to occur more prominently at earlier ages in individuals with PCOS compared to the controls (SMD = 0.38) wherein older adults with PCOS had the lowest risk of suicide (HR = 3.75, 95% CI = 2.23, 6.28]) compared to adolescents (HR = 5.38, 95% CI = [3.93, 7.37]) and young adults (HR = 9.15, 95% CI = [8.03, 10.42]) [12]. The aforementioned trends were suggested not to be subserved by a psychiatric comorbidity as there was an equivalent prevalence of psychiatric disorders between groups [12].
The aforementioned results suggest that individuals with PCOS are at an increased risk of suicide attempts; however, the underlying pathophysiological and psychopathological mechanisms require further investigation. Moreover, whether the risk of suicide is direct and independent of comorbid mental illness and/or whether causality can be attributed to both PCOS and mental disorders is not sufficiently addressed by the studies we have identified.
Association of PCOS with completed suicideWe identified one study that evaluated the prevalence of completed suicide cases in persons with PCOS (n = 268,235) [6]. Based on the retrospective cohort data, completed suicides were nonsignificantly different between the PCOS cohort and the control cohort (OR = 1.19, 95% CI = [0.71, 2.02]; adjusted OR = 0.86, 95% CI = [0.51, 1.46]). Notably, the prevalence of a mental health disorder was significantly greater in the PCOS population compared to the control cohort (OR = 1.56, 95% CI = [1.51, 1.61]). The aforementioned result suggests that the presence of a mental health disorder is a greater contributor to completed suicide risk compared to PCOS. However, the degree to which PCOS may contribute to completed suicide risk requires further investigation.
Comments (0)