Data Source and Study Population
This cross-sectional study utilized data from the 2018 and 2020 Medical Expenditure Panel Survey (MEPS), a nationally representative survey of healthcare cost, utilization, and health insurance coverage in the USA. A detailed description of the MEPS study design and survey instruments can be found online (https://meps.ahrq.gov/mepsweb/survey_comp/survey.jsp). In short, we utilized the household component of the MEPS, which collects data from a sample of families and individuals drawn from a nationally representative subsample of households that participated in the National Health Interview Survey (conducted by the National Center for Health Statistics). In prior iterations of MEPS, households were interviewed five times over a 2-year period, but in the spring of 2020, in-person data collection was limited due to the COVID-19 pandemic. The MEPS survey team adapted data collection by overlapping three simultaneous panels of data collection in the spring of 2020, compared to the usual two-panel overlap. Some in-person interviews were also moved to telephone surveys.
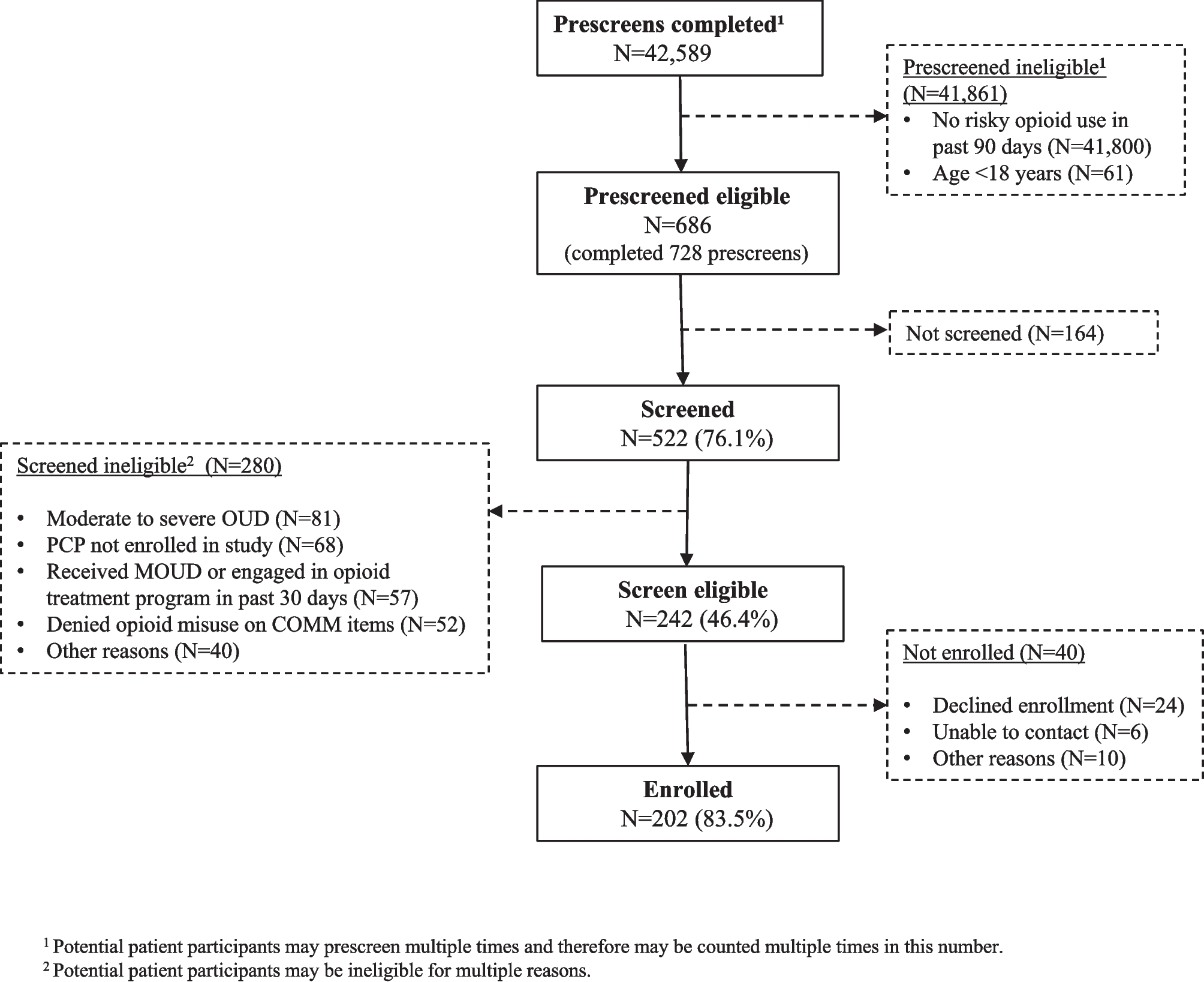
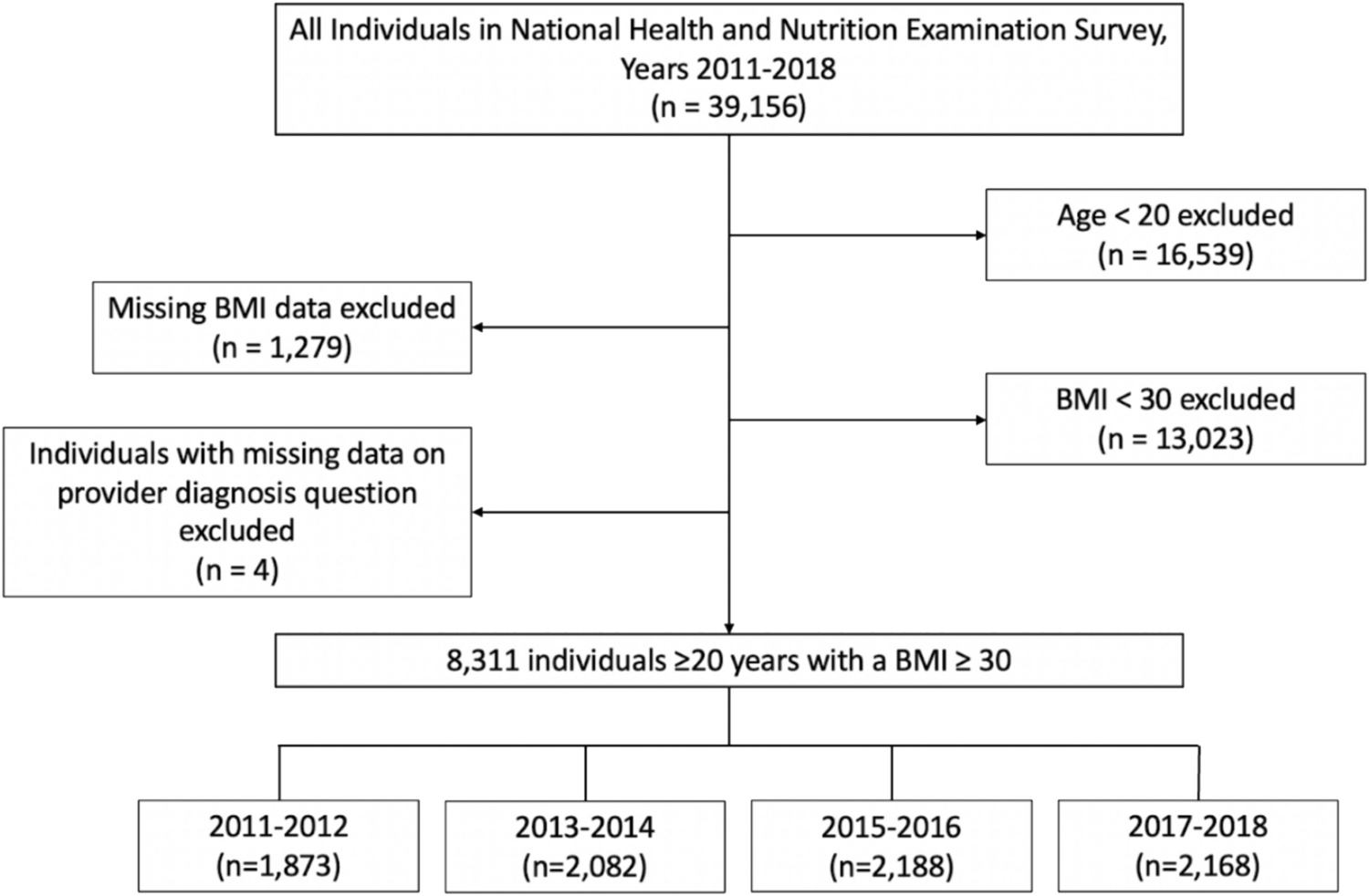
For this analysis, all adults ≥18 years old who completed the 2018 or 2020 MEPS survey were eligible for inclusion (n=44,464). Participants were excluded if they identified as multiracial (n=1030) or if they reported that they did not have a usual healthcare clinician (n=12,848). Participants were also excluded if clinician race and/or ethnicity was reported as multiracial or missing (n=10,160) or if clinician sex was missing (n=3). Our final unweighted sample size was 20,423 adults.
Adherence to Preventive Services Recommendations
For this analysis, adherence to eight preventive services recommended by the United States Preventive Services Task Force (USPSTF) or Advisory Committee on Immunization Practices (ACIP) was assessed: influenza vaccine, pneumococcal vaccine, shingles vaccine, breast cancer screening (female only), cervical cancer screening (female only), colorectal cancer screening, blood pressure screening, and cholesterol screening. Participants were only asked questions about preventive services where they fell within the recommended age group (and sex) based on published guidelines (e.g., breast cancer screening is recommended for female adults ages 50–74, so females outside of that age range and all males skipped those questions) (Supplemental Table 1). Participants also skipped questions if they reported having a contraindication for the preventive service; for example, female participants with a history of breast cancer or mastectomy were not asked about routine breast cancer screening even if they fell within the age range for screening.
Adherence to colorectal cancer screening recommendations was captured using three questions, given that multiple screening tools are available (colonoscopy, sigmoidoscopy, fecal occult blood test), and each has its own recommended timeframe. Participants were classified as being adherent if they met the guidelines for at least one of the screening tools.
Patient-Clinician Race and/or Ethnicity and Sex Concordance
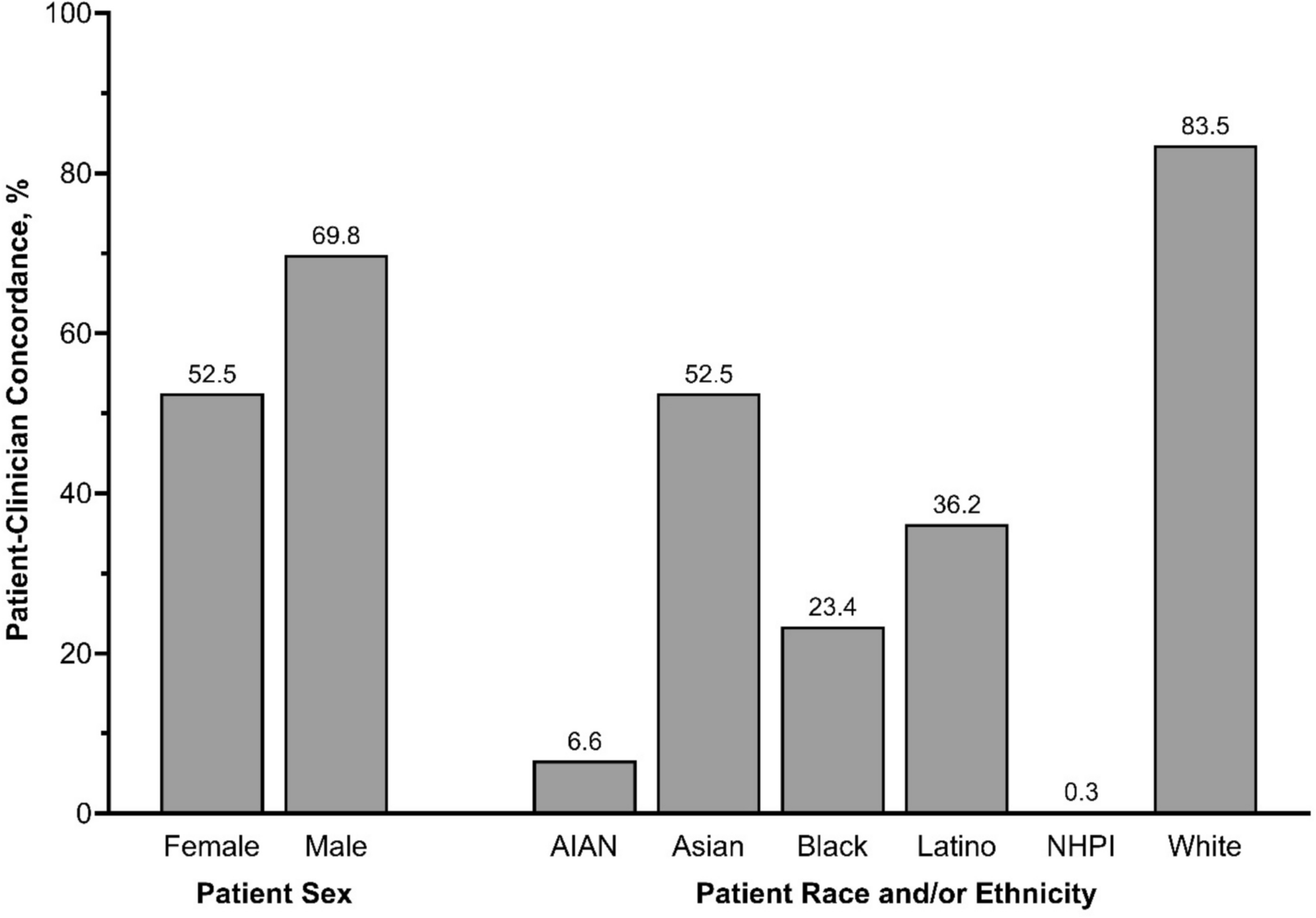
Race and/or ethnicity concordance and sex concordance variables were created using participant-reported participant and clinician demographics. Participants were asked about their ethnicity (“Are you Hispanic, Latino, or of Spanish origin?”) and their race (“What is your race?”) separately as part of the survey and then combined into a single variable. Individuals were categorized as Hispanic or Latino (Latino) regardless of their response to the race question. For non-Hispanic or non-Latino participants, race and/or ethnicity was categorized as American Indian or Alaska Native (AIAN), Asian (including Asian Indian, Chinese, Filipino, Japanese, Korean, Vietnamese, and other Asian), Black or African American (Black), Native Hawaiian or Pacific Islander (NHPI, including Native Hawaiian, Guamanian or Chamorro, Samoan, and Other Pacific Islander), and White. As mentioned above, participants who identified as multiracial or other race (and not Latino) were excluded due to our inability to determine concordance with their clinician.
Participants were similarly asked about their clinician race and/or ethnicity in separate questions and then categorized using the same criteria described above. Patient-clinician racial and/or ethnic concordance was defined as when the participant’s race and/or ethnicity matched the clinician’s race and/or ethnicity (as reported by the participant). Participants with clinicians identified as multiracial were also excluded.
Patient-clinician sex concordance was similarly defined as when a participant’s sex matched their reported clinician’s sex. Participants were asked “What is your sex?” (male or female) and “Is [your clinician] male or female?”
Statistical Analysis
Multivariable logistic regression was used to model the association between patient-clinician concordance and adherence to each preventive services guideline as well as calculate the predicted marginal prevalence of adherence and prevalence ratios,22 comparing adherence between those with and without patient-clinician concordance; sex concordance and racial and/or ethnic concordance were evaluated separately. Models adjusted for patient sex, race and/or ethnicity, age, educational attainment (less than high school graduate, high school graduate/GED, postsecondary degree), annual family income, insurance type (any private, public only, uninsured), self-reported chronic conditions (heart disease or stroke, diabetes, asthma, and cancer), self-reported general health, and survey year. Sex concordance models were also adjusted for clinician race and/or ethnicity, and race and/or ethnicity concordance models were adjusted for clinician sex. Age and family income were modeled as restricted quadratic splines. Self-reported overall health was captured with the question, “In general, would you say your health is…” with answer choices of excellent, very good, good, fair, or poor.
We used interaction terms and population-specific models to estimate the association of sex concordance among males and females separately (e.g., the association between sex concordance on influenza vaccination among female patients), as well as the association between racial and/or ethnic concordance among each racial and/or ethnic patient population. Because results from both approaches were similar, only results from the population-specific models are reported. Due to small sample sizes and very low prevalence of patient-clinician race and/or ethnicity concordance, AIAN and NHPI population-specific estimates could not be generated.
We also conducted a sensitivity analysis where race and/or ethnicity concordance models were restricted to non-White participants, as well as where race and/or ethnicity concordance was reclassified from yes/no: (1) yes, (2) no, but clinician is non-White, and (3) no and clinician is White.
Analyses were performed using SAS version 9.4 (SAS Inc, Cary, NC) and SUDAAN Release 11.0.4 (RTI International, Research Triangle Park, NC), were weighted, and were accounted for the complex sample design used in MEPS. This study was conducted in accordance with STROBE guidelines.

Comments (0)