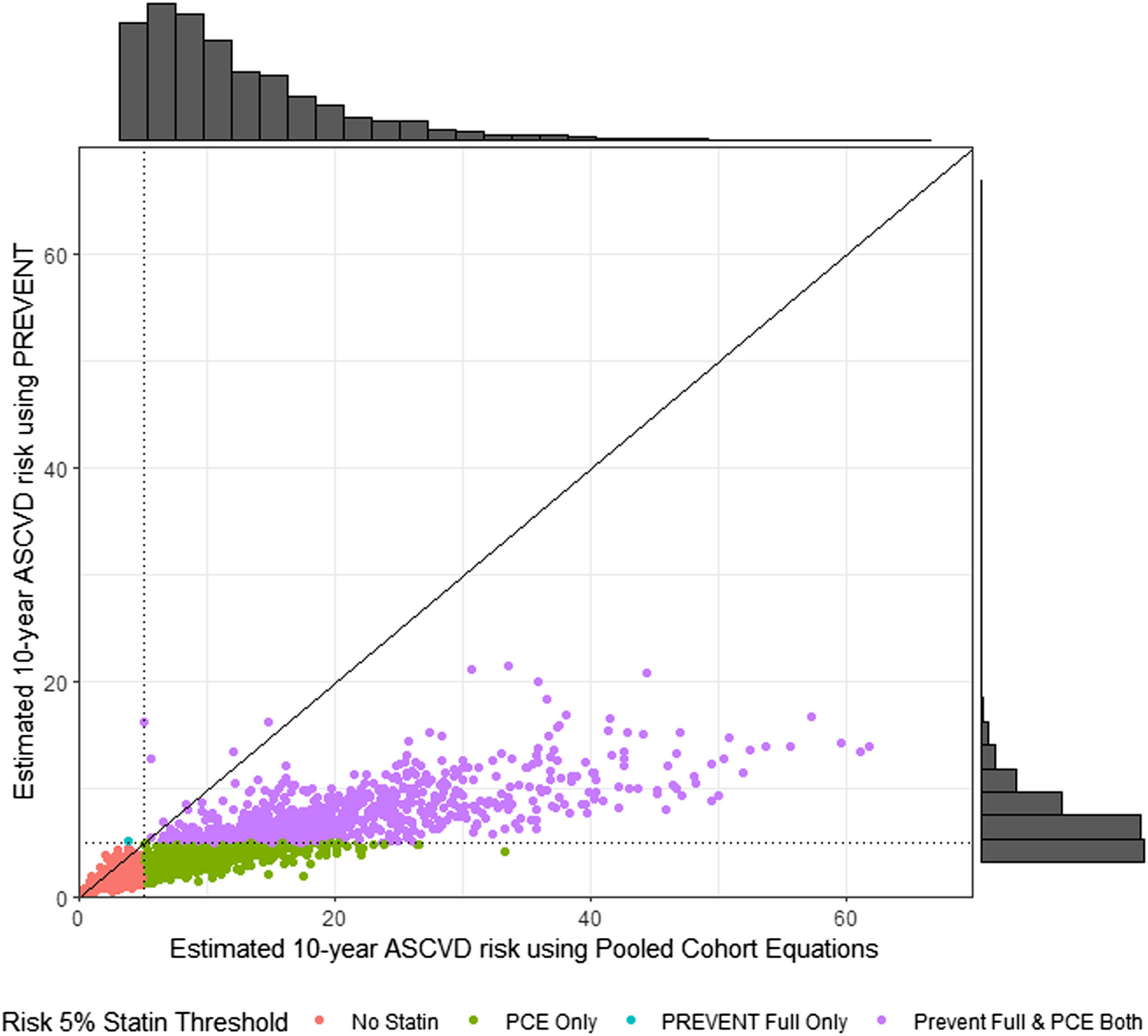
In this study, we found that among PWH, the new PREVENT equations predict lower 10-year ASCVD risk compared to the PCE. The implication is that if the PREVENT equations are widely implemented in place of the PCE without recalibration or changes in current guidelines, many fewer PWH would be strongly recommended to be treated with statins for primary prevention of cardiovascular events. While we found differences in how the choice of calculator impacts the predicted risk by natal sex and race/ethnicity, the impact on statin recommendations varied less by these groups.
Our study demonstrates clinically meaningful differences in the predicted risk between the two equations but cannot assess which, if either, is calibrated correctly because we did not have longitudinal cardiovascular event outcomes available. Lower predicted risk is an intentional feature of the new equations by its developers given concerns that the PCE may overestimate risk in the contemporary general population.17 However, prior data suggest the PCE underestimates risk among PWH in multiple populations, especially among Black individuals and women in high-income countries such as the USA.9,9,11,19 Therefore, with lower predicted risk using the PREVENT equations, this underestimation is highly likely to be worse with PREVENT compared to the PCE. Future validation studies, ideally with adjudicated events, are urgently needed to assess the calibration of PREVENT (including comparison between base and full equations) among PWH overall and within specific subgroups prior to recommendation of their implementation specifically among PWH. With recalibration, these equations may be suitable for risk prediction for PWH.
Both calculators include versions of the same risk factors, such that they remain highly correlated with each other, but a few key differences are worth considering. Both include age, sex, current smoking, total cholesterol and HDL cholesterol, systolic blood pressure, diabetes, and hypertension treatment status. PREVENTfull swaps race for SDI and adds current statin use, estimated glomerular filtration rate, hemoglobin A1c, and urine protein creatinine ratio. One interesting implication is that if an individual moves to a different neighborhood, their predicted risk and therefore statin treatment recommendation may change. Whether excluding race from prediction models exacerbates disparities or promotes health equity remains controversial.
Our study sample with complete data had a high proportion with undetectable viral load (~85%) suggesting our results may be most applicable to those engaged in care with high levels of HIV control. However, only 65% with missing data were undetectable; our similar findings among those with imputed missing variables suggest that the difference in predicted risk between the two equations is probably independent of viral load or HIV control. Among those with ongoing HIV viremia, effective HIV treatment should be prioritized and can be done in parallel with initiation of statin therapy, if appropriate.
The major implication of our study is that implementation of the PREVENT equations would result in a dramatic reduction in the number of PWH strongly recommended for statins in the USA. We have illustrated the changes in predicted risk and statin therapy with a few hypothetical patient vignettes in Table 5. The clinical benefit of statins in preventing cardiovascular events in the general population has been well established in studies of more than 170,000 individuals.20 Given the known benefit of statin therapy now proven in PWH, reducing the number of PWH strongly recommended for statins appears to contradict the findings of benefit of pitavastatin found in REPRIEVE among individuals at low to intermediate predicted risk using the PCE.3 REPRIEVE did not find evidence of heterogeneity of treatment effect by predicted risk using the PCE, sex, race/ethnicity, or other risk factors. Nonetheless, the absolute benefit is greatest among those at highest risk, so the number needed to treat is lower among those with higher risk. The British HIV Society took a different approach from the US expert panel and recommended statins for all PWH over age 40 without the need for calculation of a risk score. In the setting of poor discrimination and calibration of risk calculators, this may be a reasonable approach.
Table 5 Change in Risk Prediction and Statin Recommendation for Sample Hypothetical PatientsLimitations
Our study is a real-world electronic record-based cohort of individuals with at least one primary care or HIV clinic encounter and thus represents the population for whom a risk calculator may be used to target primary prevention strategies to prevent cardiovascular events, so it is not intended to be a population-based sample of all PWH. Misclassification of primary prevention status due to missing ICD-10 codes for prior ASCVD events or coding of “rule out diagnoses” is possible. To mimic clinical care, we used the most recent available lipid panels and creatinine, which were not necessarily on the same day as blood pressure measurement for all participants. Our dataset did not have urine protein creatinine ratios available, so we did not include this element in the PREVENTfull calculator although it should be incorporated if available. We did not compare the PREVENT equations with other risk calculators besides the PCE, such as Framingham, which has better calibration in some datasets,6 or the D:A:D calculator. As a San Francisco-based cohort, our study has limited representation of individuals who live in ZIP codes with low SDI, and we did not rescale the SDI as this is not specifically recommended by the PREVENT developers. Finally, we could not assess the calibration due to the cross-sectional nature of this dataset without longitudinal assessment of subsequent clinical ASCVD events.

Comments (0)