
Remember me



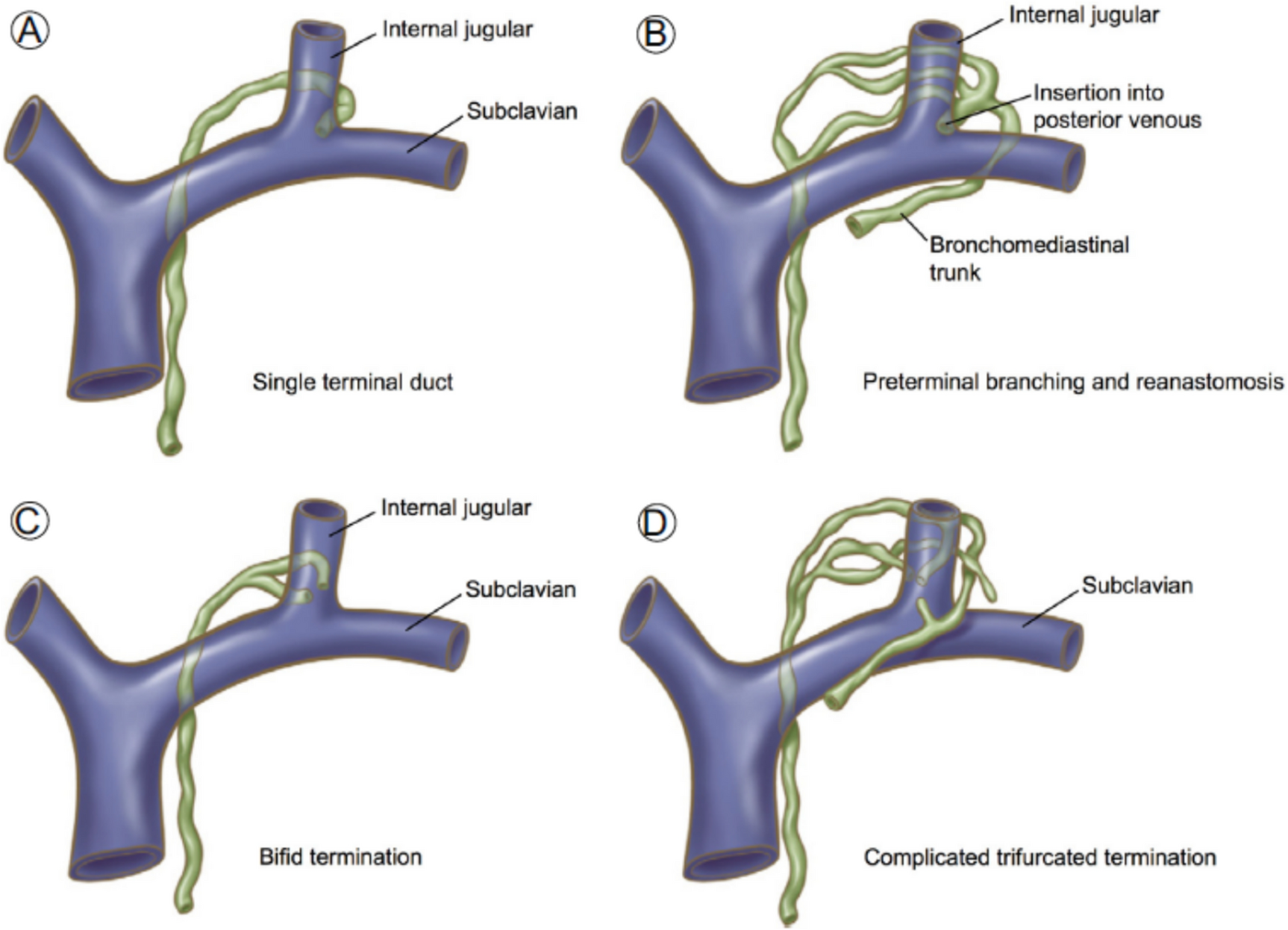
The lymphatic system is a complex network of peripheral vessels and channels that coalesces into a central channel for return of lymphatic fluid into the central venous system [1, 2]. The contiguous interlocking network of lymph vessels in the body originate from the periphery and viscera and converge into the cisterna chyli, typically located in the pelvis at the level of L1-L2 [2]. The thoracic duct originates from the cisterna chyli, representing the terminal end of the lymphatic system, and ends at Pirogoff’s Angle, the junction between the left subclavian and the internal jugular veins, where the TD drains most of the body’s lymphatic fluid into the venous system [2]. Despite this some constancy in the central lymphatic system anatomy, there are individual variations in anatomic drainage that may impose a significant challenge for identification, interpretation of imaging, and intervention of central lymphatic obstruction. The coalescence of the TD with central veins in the neck can vary significantly with studies demonstrating multiple terminal branches and the presence or lack of valves [3] (Fig. 1).
Fig. 1
Anatomic variation of the distal thoracic duct from Hsu MC, Itkin M. Lymphatic Anatomy. Tech Vasc Interv Radiol. 2016 Dec;19(4):247–254. https://doi.org/10.1053/j.tvir.2016.10.003. Epub 2016 Oct 8. PMID: 27993319
EpidemiologyThe occurrence of CLO cuts across all demographics and has been reported in adults, pediatric and neonatal patients. The specific incidence of congenital thoracic duct abnormalities is not well known [4]. The incidence is similarly no well known in adults, as a number of factors can result in central lymphatic disruption including trauma, malignancy, and iatrogenic injury. For example, certain cardiac, thoracic, and abdominal surgeries portent roughly a 2–7% risk of central lymphatic injury and leak [5,6,7,8].
Approximately 70% of cases were reported to have successful outcomes from nutritional therapy, with the failed cases resulting in a significantly higher risk of mortality in infants [9]. The morbidity and mortality rate varies widely based on the etiology of CLO and associated morbidities. The mortality range is anywhere from 10 to 50% in patients whose symptoms were not alleviated with conservative treatment [10].
Presentation and Work UpThe symptomatic presentation of patients is based on the level of central lymphatic obstruction. Several commonly occurring symptoms at our center include malnutrition, fatigue, undifferentiated abdominal pain, generalized lymphedema, and chylous fluid accumulation in the pelvis, abdomen, chest, or neck. Protein losing enteropathy (PLE) can be noted in patients presenting with CLO and contributes to chronic malnutrition. PLE is a diagnosis which is typically discovered through assessing triglyceride content in the stool [11].
As previously mentioned, the etiology of CLO varies. Obstruction of the central lymphatics can be a result of trauma, malignancy, congenital aberrances, or iatrogenically caused by surgery or chemoradiation therapy. Identification of CLO is typically a diagnosis of exclusion. Many patients have had multiple imaging studies prior to evaluation without a unifying diagnosis. After a basic lab workup, our preferred initial means of imaging remains high quality magnetic resonance lymphangiogram (MRL). While MRL functions as an initial screening tool, anatomic configurations are more appropriate and accurately characterized by percutaneous lymphangiography. (Figs. 2 and 3).
Fig. 2
MRL of patient with suspected CLO demonstrating dilated thoracic duct in the central chest and multiple collateral channels indicative of distal obstruction
Fig. 3
Image of occluded distal thoracic duct on lymphangiography with peructaneous, transabdominal access to thoracic duct to allow instillation of contrast and opacification and delineation of thoracic duct anatomy
Non-surgical ManagementConservative management of central lymphatic occlusion traditionally has included a low-fat diet and parentally administered nutrition [12, 13]. Additional medication directed at reducing the overall volume status. The targeted management of chylous ascites or chylous pleural effusion can be accomplished with repetitive paracentesis or thoracentesis, respectively.
Medical treatment and dietary modification aim to reduce the overall lymphatic burden through minimization of lymphatic fluid produced. With globally reduced lymphatic fluid production, there is reduced downstream regurgitation and therefore decreased symptoms of central lymphatic occlusion. A low-fat diet can aid in reduction of lymph fluid by decreasing the amount of dietary fat absorbed by the intestinal lymphatic channels. Medications such as diuretics can help in minimizing the overall fluid burden and aid in temporarily reducing lymphedema [14, 15].
Minimally invasive percutaneous interventions are similarly utilized to reduce the symptomatic aspects of CLO. Most commonly, this involves the abdominal ascites or pleural effusions. Drainage procedures of lymphatic fluid during large volume paracentesis or pleurocenteses can alleviate organ-specific symptoms but are not definitive solutions. Moreover, the sustainability of these solutions are questionable given the risk associated with repeated percutaneous interventions, namely, the loss of immunologic factors and significant reduction in albumin rich fluid. These attempts a repetitive drainage do not alter the underlying pathophysiology of CLO, but merely treat the symptoms (Fig. 4).
Fig. 4
Repetitive large volume paracentesis or thoracentesis and removal of chylous fluid can result in metabolic derangements, immunologic compromise, and nutritional deficiencies
Surgical ManagementProgressive advancement in microsurgery and intraoperative imaging with fluoroscopy and lymphangiography have allowed for a new, novel approach to correcting CLO. At our institute, thoracic duct bypass procedures are performed in a hybrid operating room with an interventional radiologist and plastic and reconstructive surgeon. This hybrid approach allows for percutaneous visualization of the central lymphatic system in real-time with concurrent open surgery for direct bypass of the thoracic duct to regional veins (Fig. 5).
Fig. 5
All operative cases of CLO are done in a hybrid operating room with the ability to image in real time to help guide surgical identification, anatomic anatomy, and confirmation of successful bypass
All cases are performed under standard general anesthesia with endotracheal intubation. Our colleagues in interventional radiology percutaneously access the thoracic duct through a trans-abdominal approach. Once the central lymphatics are cannulated, they are imaged with lymphangiography to identify the obstruction or anatomical aberrancy that is amenable to bypass. The percutaneously placed catheter is maintained in place to assist in the surgery and as a means for potential catheter-based therapeutic intervention.
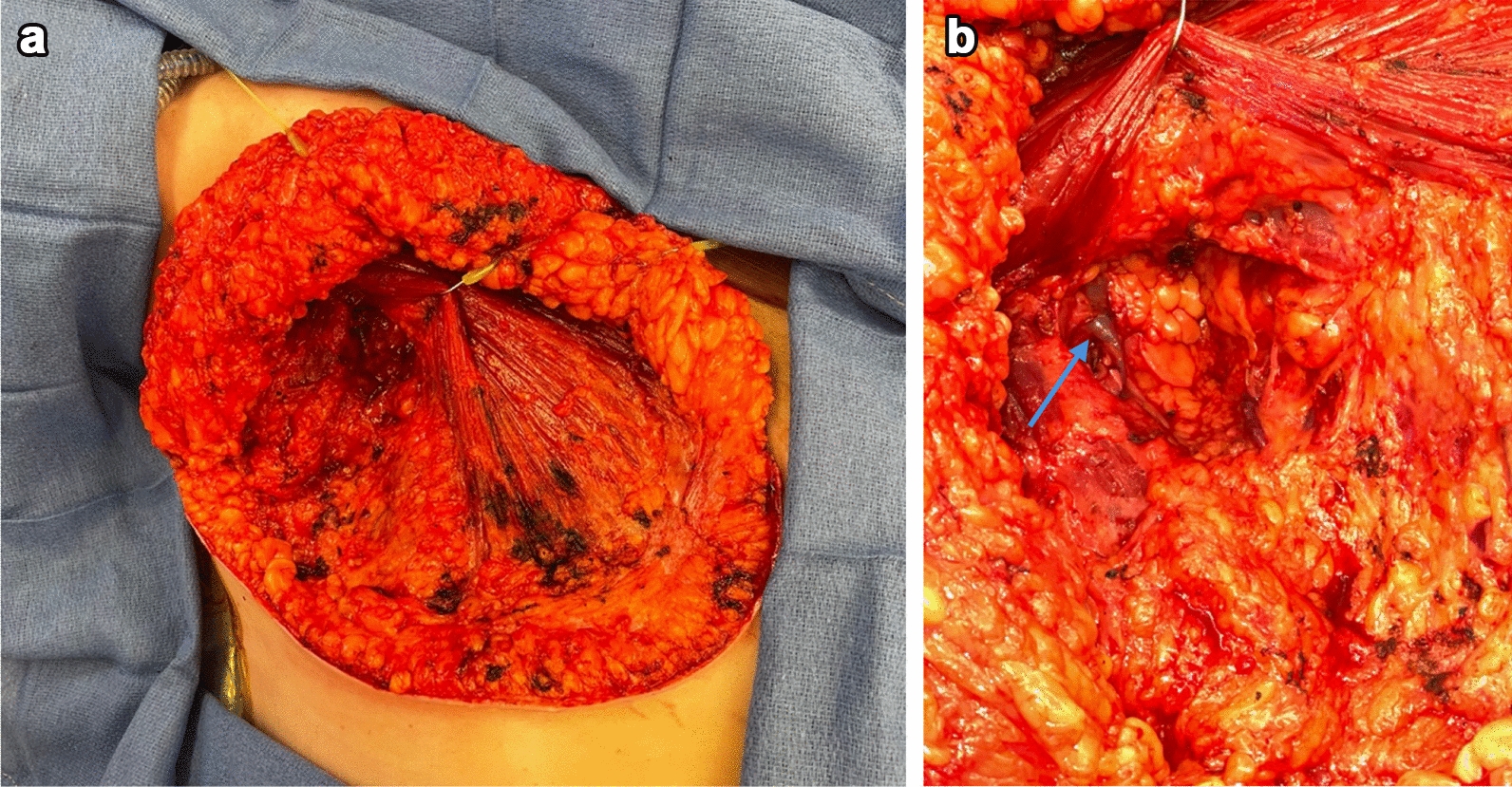
Once the anatomic pattern of the lymphatic obstruction is confirmed to be amenable to surgical intervention, the access incision is decided upon. Due to preoperative screening with MRL, the majority of central lymphatic obstructions taken to the operating room are localized to the distal thoracic duct. This is subsequently approached through the left neck. A transverse incision is made within the natural rhytids of the left neck and carried down through the platysma until the sternocleidomastoid muscle is identified. The sternocleidomastoid is divided transversely to provide wide exposure of the underlying carotid sheath. The internal jugular vein is then identified, and dissection proceeds posterior to the internal jugular vein until Pirogoff’s angle is identified, and the thoracic duct is identified within the fibrous layer of the posterior carotid sheath (Fig. 6).
Fig. 6
A: Intraoperative view of the left neck with surface landmarks of the manubrium and corresponding ribs. The tranverse incision to approach the left neck is designed in the natureal rhytids of the neck. B: A view of the left neck with internal jugular vein with blue vessel loop encircling it and traced down to Pirigoff’s angle to aid in identification of the thoracic duct. C: The thoracic duct to external jugular vein bypass completed with visual confimation of patency after instillation of methylene blue in indwelling abdominal catheter in the thoracic duct
The hybrid approach allows us to intraoperative confirm the level of obstruction and to surgically plan the level of bypass. In cases where the thoracic duct is difficult to identify, the real-time ability of imaging within a hybrid suite in the operating room allows identification, ability to discern direction of flow, and the level of obstruction. The anatomic course, level of obstruction, and anatomic location of bypass is then confirmed fluoroscopically with lymphangiography through the previously placed catheter, and then confirmed visually as well with injection of methylene blue through the indwelling catheter within the thoracic duct. In cases where the anatomic configuration of the distal thoracic duct is in question, and the direction of flow is in question, intraoperative lymphangiography as well as visual confirmation with instillation of methylene blue can be vital to ensure that the thoracic duct is bypassed at the appropriate level to alleviate the central lymphatic obstruction.
Once the appropriate level bypass is confirmed, the thoracic duct is transected in situ within the neck and controlled with a microvascular Acland clamp. A suitable surrounding venous conduit is then identified. In most cases this is the external jugular vein which is intentionally identified and preserved during the initial surgical approach. Regionally, the internal jugular vein can also serve as a suitable venous recipient, however the thoracic duct is often foreshortened and it can be technically challenging to reach the internal jugular vein for an anastomosis. The venous conduit is divided, confirmed to be patent, and irrigated with heparinized saline solution. An end-to-end anastomosis between the thoracic duct stump proximal to the level of the obstruction and the venous conduit is performed with the venous coupler (Synovis MCA, Birmingham, AL, USA). The use of the venous coupler is surgeon preference, as the end-to-end anastomosis can be hand sewed with microvascular technique as well. If if the bypass is done to the internal jugular vein, the anastomosis is done in an end to side fashion with the internal jugular vein controlled with vessel loops or atraumatic vascular clamps (Fig. 7).
Fig. 7
The Synvois venous coupler facilitates the anastomosis of the thoracic vein to a suitable venous conduit
Once completion of the anastomosis is done, patency and adequacy of flow across the anastomosis is confirmed intraoperatively with the indwelling catheter by means of intraoperative lymphangiography and methylene blue dye (Fig. 8). Once patency is confirmed both radiographically and visually, the catheter is withdrawn, and the access incision in the neck is closed in the standard layered fashion. Particularly attention is paid to reapproximate the sternocleidomastoid muscle which had previously been divided. The authors prefer placement of a closed suction drain at the time of closure to aid in detection of a lymphatic leak and manage any potential dead space from the neck dissection. The patient is typically observed overnight and discharged the following postoperative day.
Fig. 8
Lyphangiographic confirmation of patency of lymphovenous anastomosis to the external jugular vein with DSA (digital subtraction angiography)
This approach is contingent on the obstruction being in the neck at the distal TD. The surgical approach is dictated by where the level of obstruction is, and we have, at times, approached the TD through the chest or transabdominally when necessary.
OutcomesPediatricCentral lymphatic obstruction in pediatric patients can be a particularly challenging clinical scenario due to the devastating pathophysiology present in early infancy, as well as microsurgical anatomy. Our senior author and collogues at the Children’s Hospital of Philadelphia first described thoracic duct bypass for the treatment of chylothorax in infants [14, 16]. A subsequent case series following eight infants who underwent thoracic duct bypass demonstrated technical patency and symptomatic improvement in six (75%) of the patients [16].
Similarly, Boston Children’s Hospital reported on their experience with thoracic duct bypass in 14 patients with protein losing enteropathy secondary to congenital central lymphatic conduction anomalies [17]. They noted complete resolution of symptoms in five patients and (35.7%) partial resolution of symptoms in two (14.3%) patients [17].
AdultOur work at the University of Pennsylvania has been previously demonstrated in the adult literature. A preliminary retrospective review of 4 patients with central thoracic duct anomalies underwent central lymphovenous bypass with complete resolution of symptoms in three (75%) patients and partial resolution of symptoms in one (25%) patient [10]. Since this publication, we have expanded our lymphedema center and have treated over 20 patients with lymphatic anomalies at the thoracic duct. Retrospective analysis of these patients is underway. We are continuing to identify and recruit additional candidates through our lymphatic center of excellence.
Comments (0)