
Remember me



Endoscopic retrograde cholangiopancreatography (ERCP) is a minimally invasive procedure utilized in the diagnosis and treatment of choledocholithiasis. It involves wire cannulation of the ampulla of Vater and cholangiography. Interventions for choledocholithiasis include sphincterotomy with sweeping and extraction of the calculi. ERCP followed by LC under a separate general anesthetic remains the standard treatment method at many institutions. The most common complication of ERCP is pancreatitis (1.3–6.7%), followed by infection (0.6-5%) and bleeding (0.3-2%) [5]. While success rates are high, access to ERCP can pose a barrier along with the burden of pre-intervention imaging, such as magnetic resonance cholangiopancreatography (MRCP), which can delay patient care [18, 19]. Additionally, as noted above, this subjects the patients to additional LOS and anesthetic use. There are descriptions of a single procedure LC + ERCP but this is an exceptionally rare entity due to logistical complexity.
Laparoscopic-Assisted Transgastric ERCPEndoscopic management on its own is not always feasible due to surgically altered anatomy such as a history of gastric bypass or other surgically altered foregut anatomy. Many of these procedures inherently alter gastrointestinal physiology and actually increase a patient’s risk of developing cholelithiasis while also creating anatomic barriers to treating choledocholithiasis [20]. In the setting of Roux-en-Y anatomy after gastric bypass, one management option is laparoscopic-assisted transgastric ERCP [21, 22]. This is accomplished by coordinating intervention in the operating room with both the surgical and gastroenterology teams. With this technique, the surgical team mobilizes the excluded or remnant stomach and places a 15 mm trocar transabdominally through the anterior wall of the stomach. This access point allows gastroenterologists to advance the endoscope through the trocar into the stomach and perform an ERCP in a standard fashion. Upon completion of the procedure, a gastrostomy tube can be secured in place at the site of the trocar insertion, or the site can be closed using standard techniques. With a tube in place, the biliary tree can be subsequently accessed for further interventions such as biliary stent removal. If biliary stent removal is required, a 24 Fr gastrostomy tube can be placed to facilitate passage of a standard gastroscope for stent retrieval. If an additional ERCP will be necessary, larger (32 Fr) gastrostomy tubes are placed to accommodate the larger duodenoscope. Alternatively, as previously noted, the gastrotomy can be closed at the time of initial endoscopic intervention if further access is not necessary.
Endoscopic Ultrasound-Directed Transgastric ERCP (EDGE)Modern advancements in endoscopic techniques have circumvented typical anatomic challenges by utilizing endoscopic ultrasound to facilitate ERCP access. Endoscopic ultrasound-directed transgastric ERCP (EDGE) procedures are performed in patients with altered anatomy by first identifying the excluded (remnant) stomach via endoscopic ultrasound (EUS) through the gastric pouch [23]. Once the excluded stomach is visualized and found to be abutting the gastric pouch, a needle is advanced into the excluded stomach, and the lumen is distended with fluid. A wire can then be advanced into the excluded stomach and a lumen-apposing metal stent (LAMS) is deployed to create a connection between the two spaces. A scope can then be advanced through the stent to perform an ERCP. After completion of the procedure, the tract is allowed to mature, and the stent is removed at a later time. The access afforded by LAMS can be used for repeat procedures such as biliary or pancreatic stent removal. Often, the resultant gastro-gastric fistula persists and can be clipped or sutured closed endoscopically after completion of all interventions. While this is an emerging technique, there are associated complications, including a reported rate of 31% of persistent fistula [23]. This gastro-gastric fistula in gastric bypass patients can lead to weight regain, ulcer formation, and resultant bleeding or perforation.
Double-Balloon Enteroscopy-Assisted ERCP (DBE-ERCP)Double-balloon enteroscopy-assisted ERCP (DBE-ERCP) is an additional option for patients with a history of Roux-en-Y gastric bypass but is technically challenging [24]. The double-balloon enteroscope is advanced to the jejuno-jejunal anastomosis and the afferent limb is then intubated followed by cannulation of the papilla and subsequent ERCP. This technique is generally performed in tertiary care centers and has a 50–80% rate of successful afferent limb intubation [24]. The most common reason for a failed DBE-ERCP is the inability to reach the papilla, yet overall ERCP success rates approach 87.5–92.9% [24].
Percutaneous ManagementPercutaneous transhepatic cholangiogram (PTC) is often employed when ERCP is either not an option due to the patient’s acute clinical condition or has already failed due to anatomy [25]. PTC is performed under ultrasound guidance and, typically, the root of the right anterior duct is accessed with an 18 gauge needle and dilated to 10 mm to accommodate a 7Fr tube for drainage [26]. After 1–2 days, the 7Fr tube is exchanged for a 7Fr introducer, and cholangiography is performed to confirm common duct obstruction [26]. A balloon catheter is then placed at the ampulla of Vater and is inflated, followed by balloon deflation. It is then positioned above the stone and reinflated and advanced back into the duodenum to displace the stone into the duodenum [26]. A cholangiogram is then performed, and if there are persistent stones, the previous steps are repeated. If the stone is > 8 mm, lithotripsy can be performed [26]. Choledochoscopy can also be employed through an adequately sized access site. The limiting factor to management with percutaneous interventions is adequate dilation of the ducts for access. If the intrahepatic ducts are not sufficiently dilated to allow a target for percutaneous intervention, other management techniques must be utilized.
Operative ManagementCholedocholithiasis can be diagnosed intraoperatively either with IOC or laparoscopic ultrasound. Prior to widespread adoption of endoscopy and laparoscopy, open cholecystectomy with choledochotomy, T-tube placement, and drainage was the accepted standard for the management of choledocholithiasis. However, LCBDE techniques are gaining renewed surgeon interest as the previously perceived barriers are being eliminated [7]. Two main methods for LCBDE involve access to the biliary tree directly via the common bile duct (transductal) or the cystic duct (transcystic) [27]. Additionally, the hybrid (endoscopic/surgical) “rendezvous technique” during LC involves the combination of surgical and endoscopic techniques in one procedure, as described above. In the rendezvous technique, the surgeon performs the typical steps for laparoscopic cholecystectomy and intraoperative cholangiogram in standard fashion. If CBD stones are identified, the surgeon then advances a guidewire into the duodenum and the endoscopist retrieves the wire endoscopically to allow for appropriate selection of the CBD and sphincterotomy [28]. It should be noted that if ERCP is not readily available, the wire may be left in place for future ERCP.
Laparoscopic Choledochotomy or Transductal ApproachA transductal approach involves direct choledochotomy with laparoscopic scissors or an energy device on the anterior wall of the CBD and direct exploration of the CBD. Initially, closure of the CBD was performed over a T-tube, but T-tube closure was replaced by antegrade stent placement [27]. Antegrade stents were then abandoned due to increased postoperative pancreatitis and product availability [27] More recently, the use of T-tubes has become less commonplace, and, primary suture closure is preferred via intracorporeal closure of the choledochotomy [27]. Given its more invasive nature and a closure predicated on meticulous intracorporeal suturing, the transductal approach is associated with higher leak rates, compared to the transcystic approach (11% vs. 1.7%).
Transcystic ApproachThe transcystic approach for treating common bile duct stones begins with an IOC followed by insertion of a catheter through the cystic ductotomy to flush the CBD. As described below, additional interventions can be performed through this ductotomy if needed. The cystic ductotomy can be closed with clips or endoloop placement at the conclusion of intervention in a routine fashion. Leng et al. in their meta-analysis compared the transcystic approach with choledochotomy and found that the transcystic approach was associated with fewer complications, decreased length of stay, and lower hospital expenses [29]. The following sections will focus on the LCBDE techniques and will provide guidance on techniques to facilitate efficiency and efficacy.
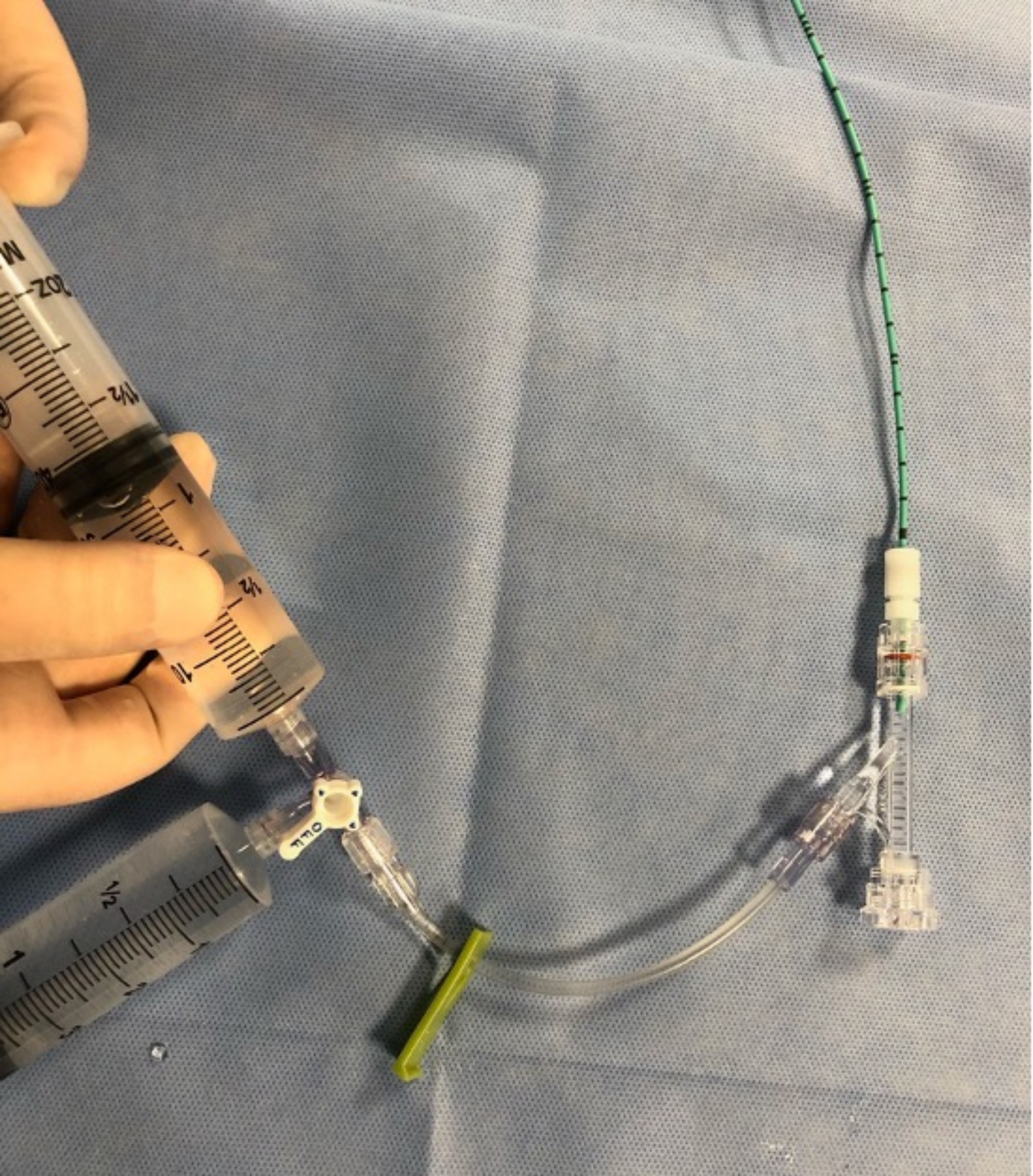
LCBDE TechniquesIn this description, we focus on transcystic LCBDE. We have found our surgery first, step-up LCBDE technique to be highly successful in clearing CBD stones. Initial steps for performing LCBDE include ensuring that the operating room can accommodate a C-arm used for fluoroscopy and the appropriate orientation of screens for viewing both laparoscopic imaging and IOC. The operating table should be positioned to allow for the placement of the C-arm to visualize the entire biliary tree. The use of a dedicated LCBDE cart, or supplies kept in a central location, is highly recommended for efficiency. Supplies recommended for intraoperative cholangiogram include the following: fluoroscopy, Tuohy-Borst connector, 12-gauge angiocatheter, 5 or 6Fr open-ended ureteral stent, surgical clips or Olsen-Reddick clamp, two 60-ml Luer lock syringes connected via 3-way stopcock and attached to extension tubing (one with saline and one with 50/50 saline/contrast mixture) (Fig. 1). We recommend using a ureteral stent as this is both economical and allows for rapid escalation to the next steps in the LCBDE pathway. We recommend using a 6Fr ureteral stent when able. However, when using an Olsen-Reddick clamp, it is important to use a 5Fr ureteral stent as the clamp cannot accommodate a 6Fr stent.
Fig. 1
Set up with two 60-cc syringes connected with a 3-way stopcock and extension tubing placed on a Touhy-Borst connector with the ureteral stent in place
After obtaining the critical view of safety and performing a cystic ductotomy, a 12-gauge angiocatheter is inserted into the abdominal wall under laparoscopic visualization. A cystic ductotomy is made with laparoscopic scissors. It is critical that the angiocatheter is placed directly in line with the cystic duct for optimal ergonomics for LCBDE performance and one-to-one feedback with wire manipulation (Fig. 2). The ureteral stent should be secured via surgical clips or an Olsen-Reddick clamp.
Fig. 2
The placement of angiocath can greatly affect the ease of LCBDE. In A, the angiocatheter is farther away and not a straight shot to the cystic duct making for a more difficult wire placement. B shows a more direct line from angiocatheter placement to the cystic duct, making wire placement easier and providing 1-to-1 feedback
If a filling defect is seen on IOC, glucagon 1 mg, in the absence of contraindications, is administered intravenously to relax the sphincter of Oddi. Several minutes following its administration, the duct is vigorously flushed, oftentimes removing small stones. Prior to flushing, under fluoroscopic guidance, a floppy-tipped guidewire is utilized to advance the stent into the CBD just proximal to the stones. This allows a unidirectional flush close to the stones, maximizing success.
Basket ExtractionBasket extraction can be used to capture stones under fluoroscopic guidance. This involves threading the wire basket down the cholangiogram catheter and removal of either whole stones or stones that have been crushed in a retrograde fashion. With the “crush and flush” technique, the stones are crushed during basket closure due to their soft nature and are then flushed into the sphincter of Oddi if crushed into small enough pieces. It is important to be confident in complete clearance via the post-intervention IOC.
Balloon DilationIf flushing is unsuccessful, antegrade balloon dilation of the sphincter of Oddi is a simple, efficient LCBDE technique that is highly successful. It is best suited for small to medium stones (8 mm or less). Supplies needed include the following: a 150 cm floppy-tipped 0.035” guidewire, balloon dilator catheter, and a rotational balloon inflation device. The balloon diameter selected must not be greater than the diameter of the common bile duct (most common diameters used are 6 mm and 8 mm). We have found the 40 mm balloon length to be ideal for working within the duodenum and cystic duct-CBD junction. After identification of stones, a 0.035” floppy-tipped guidewire is advanced into the CBD through the 6Fr cholangiogram catheter. Fluoroscopy is liberally used to visualize advancement of a generous amount of wire in the duodenum. Excess wire in the duodenum allows for prevention of loss of wire access while placing the balloon. All manipulations of the wire, catheter, and balloon should be fluoroscopically guided for the duration of the procedure.
To perform sphincter dilation, the balloon is advanced completely into the duodenum and inflated using a rotational balloon inflation device according to balloon specifications. Using balloon markers and 50/50 mix of contrast and saline for inflating the balloon will allow for optimal visualization of the balloon within the duodenum. The viscous nature of the contrast will not allow for complete evacuation of the balloon, so a 50/50 mix is used. After inflation, the balloon is gently retracted allowing for tactile and fluoroscopic identification of the location of the sphincter of Oddi. This combination of visual and tactile feedback is much more accurate than estimating the suspected sphincter location on initial fluoroscopy. After confident identification of the sphincter, the balloon is completely deflated and retracted so that the middle of the balloon (halfway between the two markers) straddles the sphincter. We advocate for gradual inflation of the balloon to the nominal pressure. When inflation is around 50% complete, we recommend a brief pause and continued gradual inflation. Careful inflation allows for a more controlled dilation of the sphincter and the prevention of spasms. A “waist” at the level of the sphincter will be briefly visualized during live fluoroscopy. The balloon is held at full expansion for 5 min for dilation. This timing has been extrapolated from ERCP literature with evidence suggesting that longer dilation (5 min) with the largest balloon able to be accommodated by the duct is associated with decreased post-procedure pancreatitis [30, 31].
After the dilation is complete, the balloon is then deflated and partially reinflated at the level of the cystic duct-CBD junction (just sufficiently inflated to occlude the duct, well below the nominal pressure). The wire can be removed at this time. The balloon is now occluding the proximal CBD allowing for forward flushing only, preventing retrograde movement of residual stones or debris into the hepatic ducts. The balloon catheter is vigorously flushed and a repeat cholangiogram is performed through it. If stones persist despite this, we then employ choledochoscopy.
CholedochoscopyCholedochoscopy involves direct visualization of the CBD stones while removal is attempted. The development of high-quality, disposable choledochoscopes that are essentially “plug-and-play” and have revolutionized the landscape of choledochoscopy. While it is only utilized in the minority of choledocholithiasis when using the step-up technique described herein, the use of the newer generation scopes is straightforward and much less cumbersome than the traditional choledochoscope. The scope is advanced over the existing wire using Seldinger technique. It is important to note that the cystic duct must generally be at least 3–4 mm in diameter to accommodate the choledochoscope. This may require balloon dilation of the cystic duct for scope accommodation, a maneuver that must be done cautiously so as to not injure the cystic-common duct junction. It is also important to note that an atraumatic grasper should be used to manipulate the choledochoscope if intra-abdominal manipulation is needed to prevent damaging the scope. Also, the choledochoscope requires an attached, pressurized bag of saline for irrigation and adequate visualization. An additional video monitoring system is required to view both endoscopic and laparoscopic views concurrently. When the stones are visualized, they can oftentimes be simply pushed into the duodenum, particularly if a balloon sphincteroplasty has been performed. Alternatively, a basket can be introduced into the working channel to allow for crushing and flushing of the stones as described above. In the event of large, immobile stones, lithotripsy can be employed.
Lithotripsy: Laser or ElectrohydraulicLaser lithotripsy is an additional adjunct to choledochoscopy after stones have been identified. A laser can be passed through the working channel of the choledochoscope and used to break apart stones [32]. Afterward, the stone fragments can either be flushed into the duodenum or can be retrieved with a nitinol basket. This technique often requires credentialing for laser use and partnering with urology colleagues may be beneficial.
Electrohydraulic lithotripsy (EHL) is another technique performed under direct choledochoscopy [32]. EHL uses a charge generator and bipolar probe to create a spark and transmit a shockwave of pressure through saline, which is subsequently used to flush the duct and acts as the medium for the shockwave [32]. Despite one’s initial natural apprehension, EHL is straightforward and is highly successful.
Postoperative ManagementIf the surgeon is confident in the completion IOC without disruption of flow into the duodenum, no additional intervention is necessary. Indomethacin (100 mg) is given rectally at the end of the operation for the prevention of postoperative pancreatitis [33]. We recommend following the institutional post-operative pathway for patients with laparoscopic cholecystectomy and recommend against trending postoperative LFTs as they do not reliably predict ductal clearance and persistent choledocholithiasis [34]. Close follow-up via telephone call 2–3 days postoperatively to ensure no symptoms of postoperative pancreatitis is recommended along with routine follow-up.
If the completion IOC is not reassuring or if there is concern for retained stones, an ERCP is recommended postoperatively. Typical reasons for abandoning LCBDE include stones in the proximal CBD that are challenging to access with the aforementioned techniques and the presence of numerous filling defects that cannot be confidently cleared by LCBDE.
LCBDE SuccessAt our institution, employing the above techniques and developing a culture that supports LCBDE both in and out of the operating room has allowed us to increase both our LCBDE attempts and success rate. We have demonstrated an LCBDE success rate of 69% in overnight cases and 71% in daytime cases [13]. Additionally, length of stay and hospitalization costs were reduced with a surgery first mindset including concurrent LCBDE [13]. While we have not been able to eliminate post-op ERCP entirely, we have significantly reduced the need for post-op ERCP with our surgery first mindset. First, we eliminate unnecessary ERCP when the IOC is normal. Second, when the IOC is positive, we are able to clear the duct in over 70% of cases, eliminating the need for post-op ERCP in this group.
Comments (0)