Gallbladder perforation as a rare complication of minor blunt abdominal trauma: a case report
Because of its anatomic position and relatively small size, blunt abdominal injury to the gall bladder is rare and the true incidence is not exactly known. Preoperative diagnosis is difficult and the diagnosis is almost always intraoperative especially in resource limiting areas [12]. Isolated traumatic gall bladder injury is more likely in male adults’ individuals probably due to their increased involvement in violence activities and the next groups are children in road traffic accident [13]. The road traffic accident, fall down, knocked down by a horse, direct blow with butt of gun, direct blow to the abdomen and blow from fist are the causes to isolated gallbladder injury [4]. The current case report might be the second which is caused by blow fist injury according to the existing literatures [14].
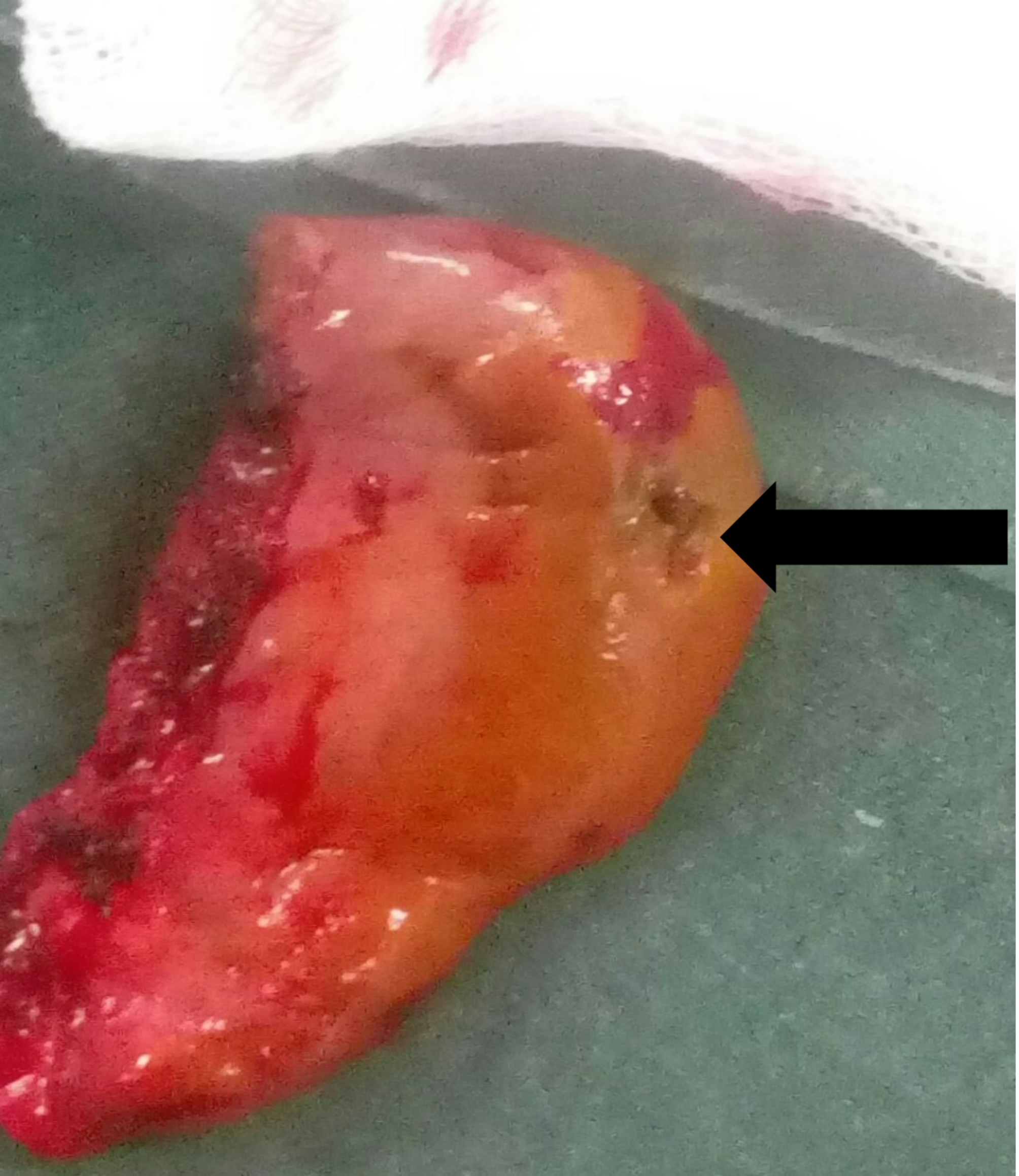
The fundus is the common site of perforation and there are presumed risk factors generally for blunt trauma perforations like: distended gall bladder following meals or alcohol, obstructive biliary diseases, and non-scared gall bladder [14]. Most Patients’ presentation are vague and it creates a diagnostic challenge for clinicians, and most patients miss and come in a delayed time [15, 16]. Usually, patients report mild symptoms with minimal constitutional upset that resolve transiently and don’t visit or are discharged from the health care center until later and they come back days to weeks later with abdominal distension and ascites the so called “period of illusion” [12]. Here, in the current case also, presentation is after a kind of period of illusion, which is really difficult for diagnosis. This is further compounded with limited resources for further workup with advanced imaging modalities [17, 18]. After intraoperative diagnosis, management depends majorly on the local findings. In our case, we resuscitated him well preoperatively, the local tissue was not as friable as in other cases, and we did a formal cholecystectomy, which is a standard recommendation. But, when local tissue is too friable, partial cholecystectomy is the next option [6, 19, 20].
Some proposes laparoscopic cholecystectomy as the safest and most effective way out of isolated gallbladder injuries for diagnosis and management [16]. Endoscopic sphincterotomy and temporary biliary stenting are also well suited to encourage preferential bile drainage to the duodenum and prevent bile leakage into the peritoneal cavity after complicated laparoscopic cholecystectomy [21]. Postoperatively, patients’ need to be monitored for adequate hydration status, signs of biliary leakage and possible infections.




Comments (0)