
Remember me


In the chaotic moments following a critical injury, the success of trauma care hinges on a team’s ability to rapidly coordinate and adapt. Effective interdisciplinary teams balance structured protocols with the agility to respond to unexpected injuries and evolving patient needs. To develop effective teams, trauma leaders can learn from the growing science of teamwork in healthcare. Healthcare teams comprise professionals from diverse training backgrounds, each with interdependent roles [1]. Delivery of healthcare in interdisciplinary teams has improved quality and efficiency of care, as evidenced by improved patient outcomes such as increased survival and lower risk of recurrence in cancer patients [2,3,4] and decreased cost of care for complex issues such as antibiotic utilization and mechanical ventilation in the critical care sphere [5,6,7,8]. However, trauma teams present unique challenges of coordination and collaboration [9, 10] that should be acknowledged and addressed by leaders to ensure the teams’ success.
Key qualities of a high-performance, interdisciplinary, collaborative team as outlined in Table 1 include: having shared goals and objectives, cooperation among the different roles and responsibilities, and strong communication [11, 12]. When these qualities are lacking, interdisciplinary collaborative teams can face significant challenges that ultimately result in team conflict and failure to achieve patient care goals. Interdisciplinary stereotyping can reduce collegiality and collaboration. Failure to establish objectives can cause confusion as to which tasks are required to achieve the team’s goals, and a lack of personal investment in the team’s success can cause greater focus on individual roles rather than teamwork.
Table 1 Qualities of high-performance collaborative teamsTeam leaders can address these challenges by establishing a team culture and priorities. By defining roles, delegating tasks, and articulating shared goals and objectives from the beginning, team leaders can lay the foundation of collaboration. To mitigate communication barriers, team leaders can establish ‘psychological safety’ by seeking member input, listening when concerns are raised, being receptive to members’ ideas and questions, and providing feedback so that team members feel comfortable speaking up [13]. Establishing this norm of psychological safety, where team members feel comfortable speaking up without fear of reprisal [14], enables team members to voice questions and concerns, further ensuring that everyone is on the same page about the plan.
Leadership becomes even more important in interdisciplinary rapid action teams, like those in trauma resuscitation that work in fast-paced, unpredictable situations [13]. Having shared mental models is paramount to allow teams to respond to uncertain circumstances. When team members have a shared mental model of a situation, they can anticipate each other’s responses and actions and coordinate effectively when faced with an unexpected and swiftly evolving case [15]. Team leaders are instrumental in adjusting the team response when given new information and thus must have a bird’s-eye view of each role and interconnected action [13]. Additionally, although outside of the scope of this review, it a cannot be overstated that the success of any trauma team is contingent upon the infrastructure provided by designated trauma centers and trauma systems from pre-hospital care through to rehabilitative services.
Unique Aspects of Trauma TeamsMultidisciplinary teams are widely recognized as an advantageous and necessary aspect of comprehensive healthcare in the United States, but developing effective trauma teams requires applying these techniques in unique, high-speed, high-intensity settings [16]. Similar to cardiopulmonary resuscitative or rapid response teams, trauma teams assemble within minutes for quick-action and consist of members from different specialties with varying degrees of skills and experience [17]. Resuscitation teams must act promptly in response to constantly changing physiology to initiate corrective action to prevent morbidity or death. Trauma teams meet the additional challenge of providing care to injured patients at the point of entry with limited foreknowledge of their patient’s history or condition. The composition of a trauma team usually involves coordinating teammates across multiple departments on all levels from students and trainees to licensed providers and physicians [17, 18]. The care of a traumatically injured patient can be challenging based solely on the severity and complexity of common injury patterns. Trauma patients in extremis enter the healthcare system with no prior planning, and may be intoxicated, distressed, or agitated. The situation may be confounded by the presence of family, friends, law enforcement, or in multi-patient scenarios. Noise level, provider stress, patient acuity, and bystander interference are all distractions that prohibitively affect communication and teamwork which must be overcome to provide high quality care [19].
One of the most pervasive features of a trauma team is the inability to ensure consistent personnel or established relationships. Since trauma care requires 24-hour a day staffing, teams frequently change from one activation to the next, limiting consistency and established working relationships. Ideally, trauma centers would attempt to staff teams with members who work together day in and day out, similar to operating room specialty teams. In reality, trauma team members may meet for the first time in the bay and may not know each other or be familiar with each other’s roles, experience, or skills. Emergency room physician schedules often do not align with surgery department schedules, and physician work hours may not correlate with nursing shifts. A recent randomized control trial studying team familiarity in general medical inpatient teams showed improvement in complex cognitive tasks at 12-months. In this study, the intervention group consisted of PGY-1 residents who worked with nurses on a single unit during all required 16-weeks inpatient medicine rotations versus the control group that completed 16-weeks of rotations on 4 different units over the course of a year. The physician/nurse teams were then assessed at 6- and 12-months using simulation-based scenarios showing no difference at 6-month, but improvement by the intervention group in leadership, management, and scenario outcome at 12-months [20], suggesting that long-term team interaction correlates with enhanced teamwork. Another observational study at a single academic institution examined team familiarity as determined by the amount of time shared among clinicians caring for mechanically ventilated patients across five ICUs, including a trauma-burn ICU, and showed that increased shared clinical care time was associated with 4.5% greater probability of spontaneous breathing trials, 23% reduction in mechanical ventilation duration in days, and 3.8% lower probability of mortality [21]. This further supports an association between team familiarity and patient outcomes. Although team familiarity has been recognized as an important attribute of high-performance teams, there are few studies on team familiarity in civilian trauma teams and a “familiarized trauma team” staffing model has not been broadly adopted.
Roles and Characteristics of Team LeadersThough all team members contribute to team function, the presence of an identifiable leader is particularly important given the acuity and instability that trauma teams face. Common leadership attributes exhibited by leaders in all fields include establishing a common goal, assembling a team with appropriate composition to carry out a desired purpose, ensuring adequate preparation, directing prioritization and delegation of tasks, promoting communication and feedback, deconflicting competing interests, fostering a productive environment, and promoting adaptability [22, 23]. Team leaders are also instrumental in establishing the “culture” of the team from the outset. In small rapid-action teams these behaviors may occur in swift succession and in parallel but can be augmented by active planning.
Preparation & Team AssemblyHaving a trauma activation plan is a major component of trauma center verification [24]. However, trauma centers have flexibility in determining what works best within the standards based on institutional resources. Policies and protocols are helpful in outlining specific “rules of engagement,” such as which providers perform head-of-bed airway management or procedural interventions during the resuscitation, but if not otherwise determined, team leaders should proactively coordinate team roles and perform preparatory briefing [25]. An important facet of team assembly is garnering an understanding of experience and skill levels within the team. There are often learners or trainees on trauma teams and knowing their prior experience is important in identifying potential gaps in knowledge and skill sets. Sometimes, a quick orientation to the trauma bay at the beginning of a shift may be all that is required to improve team confidence and cooperation [26]. Taking time at the beginning of a clinical rotation or call period may be necessary to provide refresher training on basic trauma resuscitation skills such as primary and secondary surveys, ultrasound in trauma (FAST exam), and other procedural skills. This can be time consuming in institutions that have high patient volume and high provider turnover but can be crucial in preventing team complacency [26].
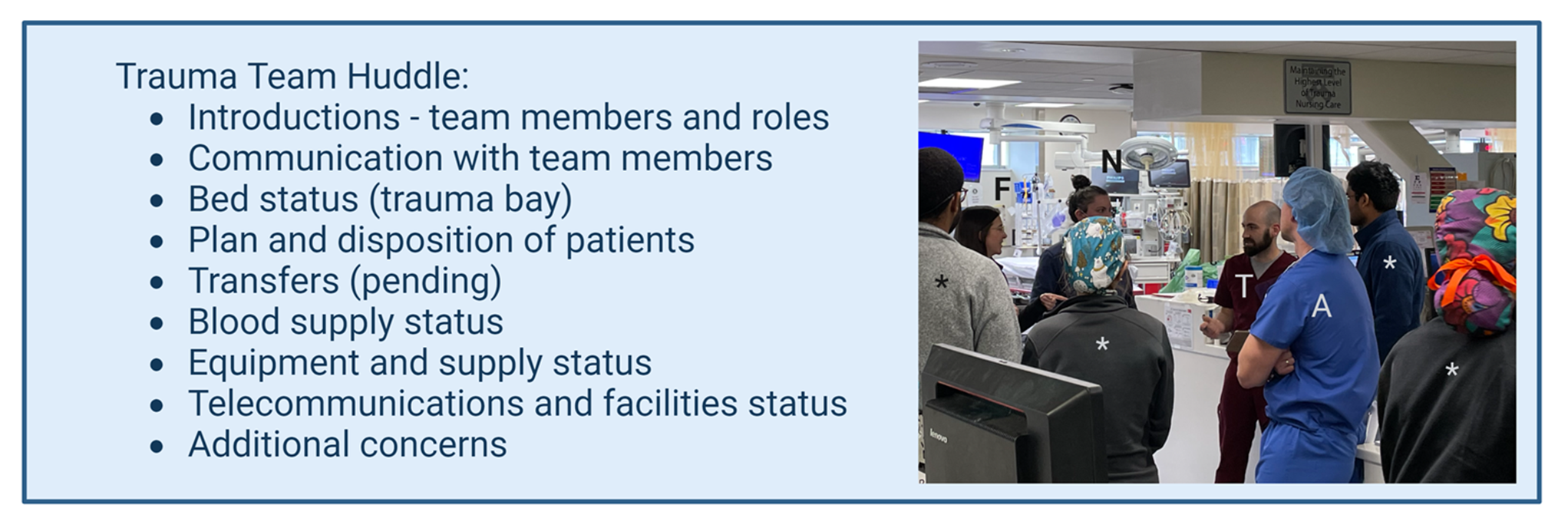
Once a trauma activation is signaled, one of the first leadership tasks is to conduct a pre-brief or “zero point survey” to prepare each individual, the team, and the environment for patient receiving [27, 28]. This is often a “just in time” activity, providing only a short interval for team members to mentally prepare for the task at hand. A preparatory “trauma team huddle” at the beginning of a shift may be beneficial in providing mental preparation. Similar to pre-operative huddles or TeamSTEPPS that have been shown to improve patient satisfaction, clinician confidence, and decrease sentinel events [29, 30], a trauma team huddle can help in obtaining real-time situational awareness without the stress of imminent patient arrival. Our institution has enacted a trauma huddle at the beginning of day and night trauma nursing shifts to make introductions, confirm team roles, and outline means of communication with the respective team components which is independent and distinct from the activation team pre-brief (Fig. 1). The trauma huddle is especially useful as at our institution where there is a high likelihood of little or no prior notification of inbound patients. This precludes an effective pre-brief or “zero point survey” prior to patient arrival. The shift-start trauma huddle is an adaptation of command huddles described by military resuscitative units to promote overall situational awareness when inbound casualties arrive [31, 32]. The trauma huddle also provides all team members with an understanding of the current staffing, capacity of the acute trauma beds (trauma bay), operating rooms, and trauma intensive care unit, as well as any resource limitations or logistical issues like equipment dysfunction, consumable supply limitations, computer and telecommunication downtime, or local/regional events that may impact the trauma system. Some institutions may have other formalized means of addressing these considerations such as checklists or real-time status boards. Whatever the means of conveying this reporting, information gathering and preparation is a necessary safeguard prior to a high-acuity event.
Fig. 1
Trauma Team Huddle. A trauma huddle checklist is provided outlining the key points for trauma team situational awareness. The trauma team huddle is performed after changes in manning such as call or nursing shifts as pictured: trauma attending (A), trauma fellow (F), nurse (N), emergency technician (T), and residents (asterisks)
Prioritization & Deconflicting Competing InterestsThe trauma team leader oversees the patient’s clinical trajectory and therefore directs prioritization of tasks for the group. It is incumbent for the leader to set the pace of a resuscitation pushing tempo where needed and likewise providing a calming presence. Experienced trauma team members may be familiar with the protocolized approach to trauma resuscitation and may pursue their designated tasks without direction. However, the team leader may need to deviate from protocol to redirect focus on the highest urgency interventions, and help the team avoid being deterred by distracting injuries and circumstances. Incumbent in this process of directing team prioritization and adjusting response is the ability to convey that information to the team constructively.
Communication & DistractionsTrauma team leaders are responsible for ensuring an environment conducive to effective communication and eliciting closed-loop communication. Effective communication is one of the most important facets of high-acuity team responses, and is one of the most challenging. Miscommunication in trauma resuscitations is two to four times more likely to result in fatal errors than in other healthcare settings, due to the urgency, multiple parallel tasks, and high-stress conditions unique to trauma care [33]. A recent study in trauma simulation among surgical trainees utilizing nontechnical skills assessments and eye tracking demonstrated that teams scored the worst in communication compared to other domains such as leadership, situational awareness, cooperation and resource management [34]. Closed-loop communication as part of crisis resource management is a widely used metric for team performance and has been adopted by most high-acuity action teams [35, 36]. Some of the common reasons for communication failures are ambient noise level and parallel conversations [35]. Experienced providers trained in team communication techniques may have more skill at filtering out external stimuli, but less experience teammates may become overwhelmed or confused, which must be recognized by the team leader and addressed to maintain smooth team performance. It is essential that teammates feel empowered to feedback information and ask for help when necessary [37, 38]. It is likewise important for the team leader to ensure an environment conducive to communication. Making a clear announcement for uninvolved personnel to leave the resuscitation area or asking unengaged staff to make that announcement and usher people out can minimize distractions.
Productive Environment & Provider StressThe American Association of Critical Care Nurses published Six Essentials of the Healthy Work Environment that cited skilled communication, true collaboration, authentic leadership, effective decision-making, meaningful recognition, and appropriate staffing as key factors in enabling teams to provide quality care and maintain a strong work environment [39]. As outlined above, the team leader is instrumental in ensuring these elements are maintained. It is also the team leader’s responsibility to recognize situations when the team is under an exceptional amount of strain and in need of additional resources. That may include everything from performing a post-resuscitation debrief to requesting additional back-up or surge staffing from other units during multiple high-acuity patient resuscitations.
Provider safety and prevention of workplace violence is also a foremost concern in emergency departments and trauma centers [40,41,42]. Healthcare workers are five times more likely to suffer from workplace violence than the general workforce, and over 40 states have laws enacting penalties for healthcare worker assault [42]. Emergency departments are also cited as being among the healthcare settings at highest risk for workplace violence [43]. The Centers for Disease Control cites increased stress, the experience of pain, substance use, prior history of violence, lack of staff training, complacent attitudes, fatigue, inadequate coping and interpersonal management skills, and staffing constraints as risk factors for workplace violence in healthcare settings [44]. Clear protocols and multi-component strategies for managing aggressive or dangerous behavior in the emergency department and trauma bay can help promote physical and psychological safety of the team [41, 42]. Evidence-based interventions that have been studied include patient screening, staff education and training in de-escalation, and environmental design [44, 45]. Behavioral response teams have also been shown to reduce the number of physical assaults, security interventions, and the use of restraints [46]. In a review by Recsky et al., no compelling evidence was found to support a specific approach to workplace violence mitigation but favored a comprehensive approach that included multiple strategies [45]. The team leader has an obligation to recognize high risk conditions and assist in de-escalation efforts for both patients and staff.
Leading in a High-Stress EnvironmentMultiple studies in both civilian and military settings have demonstrated that strong leadership behaviors such as assuming leadership, assigning roles, sharing information, eliciting input, and facilitating closed-loop communication is link to a greater likelihood of completing trauma assessments and less time to the next phase of care [34, 47,48,49,50]. High-acuity environments necessitate the need for adaptability and responsiveness. Exhaustive theories of leadership have developed over time in various domains of healthcare such as management, nursing, and education, but leadership styles in the provision of trauma care have not been as well characterized. The available literature favors directive (command-driven) versus empowering styles [47]. Ford et al. demonstrated that employing a “directive” style is more effective for resuscitation of patients with a high Injury Severity Scores (ISS), where an empowering style can be suitable in lower acuity patient care [47]. Therefore, trauma team leadership is dependent on dynamic leadership to provide the clinical agility required for a rapidly evolving environment [51]. Essential is an ability to “read the room” and use human-factor intelligence to perceive how team members are functioning in order to direct tactics for highest yield [52].
Team familiarity when coupled with emotional intelligence permits leaders to anticipate teammate stress responses and pre-emptively assign tasks based on respective skill set and prior performance. Trust within the team is an vital facet of teamwork reinforced by the leadership characteristics listed above to reach a common goal of excellent patient care [53]. Leaders should trust that teammates are professional in the execution of their job, and likewise team members should trust that leaders have the same professional expertise with the collective goal of a successful outcome.
Designating the Trauma Team LeaderA standard model for trauma team staffing in U.S. civilian trauma centers includes a surgeon trained in trauma care to act as the team leader. This individual is also usually the highest trained in complex surgical procedures necessary for the provision of trauma care. In situations with multiple operative patients, it can be argued that the surgeon should be doing surgery, leaving a theoretical gap in leadership in the trauma bay. However, patients with traumatic injuries worldwide often present to non-trauma centers, where a provider without trauma-specific training may unexpectedly find themselves leading a high-acuity team. This is in part why the American College of Surgeons developed the Advanced Trauma Life Support (ATLS) curriculum in 1978 to provide a framework and training in the trauma team approach and care of injured patients [54].
Prior evidence suggested no difference in outcome when trauma resuscitations were led by trauma surgeons versus non-surgeons [55, 56]. More recent evidence has shown that an on-site trauma surgeon resulted in earlier completion of ATLS components, decreased total resuscitation time by 259 s, and overall greater adherence to ATLS tasks [57]. Caldwell et al. also demonstrated that during trauma simulation among trainees, emergency residents scored higher in evaluation and planning while general surgery residents scored higher in action processes, but importantly there were no differences in team management between groups [58]. Any provider experienced in the care of injured patients and knowledgeable in evidence-based trauma care can lead the team, including emergency department providers, advanced practice providers, and nurses. For example, the United States Navy and Marine Corps have long employed forward resuscitative surgical teams in tandem with shock trauma platoons manned by non-surgeon physicians, physician assistants, nurses and medics to perform the casualty care and resuscitation with the expectation that the surgical team will be otherwise engaged in operative care [59]. Expanding on this concept for civilian trauma care, in the case of multiple or mass casualties, the trauma surgeon may be more valuable in the operating room, allowing for other trauma and disaster trained personnel to function at the incident command level until additional resources have been mobilized.
Though the skills necessary to provide effective trauma team leadership can be mastered by many, not all leaders will meet an equal reception. Trauma teams are as susceptible to societal biases as any other workplace. Cioffi et al. published the results of a recent survey among the young members section of the European Society of Trauma and Emergency Surgery which identified a gap in mentorship and education in non-technical skills among early career and female surgeons in trauma disciplines [60]. Recent studies have examined internal team dynamics with respect to team bias, taking into account verbal and non-verbal biomarkers as well as personnel demographics [60,61,62]. Female team members were assumed to be nurses and males to be physicians [61]. Female members were perceived as being ignored or overlooked and female team leaders were felt to need more proactive interventions to be recognized as leaders [61]. Team leaders who were people of color or younger were also less likely to be correctly perceived as the team leader [61]. However, another recent study using post-hoc video review to examine gender in trauma team leadership demonstrated that there were no gender-based differences in leadership or patient care when reviewed by an outside observer performing a validated behavioral assessment [62].
Improving Team DynamicsA general tenet of teamwork is to train together, train often, and “train like you fight.” Training is in fact mandated in the Resources for Optimal Care of the Injured Patient, published by the American College of Surgeons Committee on Trauma, that requires verified trauma programs to incorporate trauma education and disaster management drills into routine operations [24]. Over the last decade, efforts to provide training to medical providers in non-technical skills and leadership have taken on a greater role over a traditional individual algorithmic approach previously emphasized in ATLS. A randomized control trial by Botelho et al. among medical student teams performing simulated pediatric trauma assessments found that teams who engaged in non-technical skills specific debriefing that involved discussion of situational awareness, communication, decision-making, teamwork, and leadership were more likely to express confidence in leading, behavior assessment scores, and completion of ATLS tasks when compared with standard ATLS debriefing strategies [63]. Team training may take on a variety of formats such as didactic, online learning modules, simulation and drill-based practical application, debriefing, and post-hoc video review [64]. There are no head-to-head studies evaluating the efficacy of one training paradigm over another, but what has become clear is that team training improves overall team performance.
Leadership training has likewise garnered increased attention and taken the form of facilitated discussion, didactic, observation and reflection, simulation, and hands-on training [65, 66]. One of the most widely studied leadership training methods is simulation-based training. A recent randomized control trial demonstrated that among second and third-year emergency and general surgery residents simulation-based leadership training resulted in improvement in five of seven assessed leadership behaviors [50]. Quon et al. found that the learners preferred informal rather than formal methods of leadership training, and that the method employed should be adapted to the learner’s level of experience– early level learners preferred supervision whereas more experience learners valued autonomy [66]. There is growing eviden
Comments (0)