
Remember me
The American Psychiatric Association defines MI as “a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning” (2013, p. 20). The definition encompasses a wide range of conditions including anxiety, depression, psychosis, attention-deficit/hyperactivity disorder (ADHD), and substance use disorders. Acuity ranges from any mental illness meeting the DSM’s diagnostic criteria to serious mental illness resulting in substantial interferences with or limits on one or more major life activity. In 2019, 21% of U.S. adults experienced any mental illness; one quarter of those lived with serious mental illness (SAMHSA, 2021).
Mental illness often emerges unexpectedly and can manifest as a crisis, catching individuals and their loved ones off guard. A shift in mental state, such as intense anxiety, panic attacks, or depressive episodes, may emerge suddenly or the crisis can build up over time until worsening symptoms reach a breaking point. Securing MI treatment is a complex and ambiguous consumption experience. The causes of MI are unclear; the prevailing biopsychosocial model implicates a combination of psychogenic causes including trauma, maladaptive learning, and cognitive distortions, and somatogenic causes including biology, genetics, and illness (Harrington, 2019). Diagnoses are imprecise and rely on behavioral observation and self-reports of intangible feelings rather than physical medicine’s blood tests and imaging studies. Treatment pathways are complex including psychopharmacology, psychotherapy, and alternative therapies, used in tandem or separately, delivered in outpatient, hospital, and long-term residential settings. Treatment effectiveness is often unclear. Symptoms may abate with treatment, but unexpectedly come raging back. Provider shortages and a fragmented delivery system hamper access to treatment. Untreated MI can have significant consequences including unsafe behaviors, destroyed relationships, inability to perform activities of daily living, impaired work performance, and worsened physical health. Individuals with untreated MI often use substances to self-medicate, further exacerbating existing symptoms (SAMHSA, 2021).
In short, the MI treatment journey is a crisis-ridden, highly consequential consumption experience marked by deep uncertainty — a TCJ. We situate our study in the context of MI treatment following Stremersch et al. (2023) advice on the pages of this journal that context-specific studies may illuminate phenomena overlooked in multi-context studies, especially if the research team has expertise in the context. Our research team has deep proficiency in the MI space developed through advanced training, ongoing direct work with individuals whose lived experiences are like our research participants’, and ongoing collaboration with industry and nonprofit partners.
Data collectionWe used narrative interviewing to understand how consumers navigate the consumer journey for MI treatment following Richardson’s (1990, p. 126) reasoning: “When people are asked why they do what they do, they provide narrative explanations, not logical-scientific categorical ones. It is the way individuals understand their own lives and best understand the lives of others.” Narrative-based interviews give researchers a window into participants’ assumptions about how the world works and should work (McCracken, 1988), and how identity interacts with personal experiences over time (McAdams & McLean, 2013).
Participants were recruited across the U.S. with the assistance of nonprofit agencies and schools working with individuals with MI, electronic postings to neighborhood listservs, and snowball sampling from the acquaintance networks of our participants. We screened to select participants seeking treatment for serious MI interfering with life activities and moderate MI, rather than less complex, lower acuity conditions. We intentionally did so, following Pratt et al. (2006, p. 238) advice, “Extreme cases facilitate theory building because the dynamics being examined tend to be more visible.” Three MI domain experts confirmed the validity of our screening criteria.
Our dataset includes 33 participants comprising 14 individuals with mental illness and 19 parents of individuals with mental illness (Table 3). We intentionally include both individuals and parents for three reasons. First, because we are interested in the consumer journey rather than the clinical experience, we sought research participants who are responsible for and involved in the decision-making and purchase of mental health services. This includes people with the condition, and often includes family members who frequently select, guide, and pay for services (Harrington, 2019); in other words, surrogate consumers who share collective goals (Epp & Price, 2011). Second, we are interested in tracing the entire journey beginning with its onset. MI often emerges in childhood or adolescence (Kessler et al., 2007); it is unlikely an individual with childhood-onset MI would have guided the early purchase process. Third, by interviewing parents, we can explore higher acuity situations without risking the interview potentially being disruptive to the individual with MI or that MI’s impairments interfere with consumer agency. Interviews lasted between one and three hours, were audiotaped, and transcribed for data analysis. Participants were not paid for participation. Institutional Review Boards at each of the authors’ institutions approved the research protocol.
Table 3 Informant characteristicsFollowing long interview techniques (McCracken, 1988), we asked participants to, “Tell me about yourself (your child).” As needed, participants were prompted to describe the onset and evolution of the MI and their reactions along the journey. We specifically queried about turning points, how providers were found and evaluated, and the impact of MI and its stigma on activities and relationships. Following Gioia (2013), we adjusted the interview protocol as we learned more. For example, we asked one-third of the participants to sketch their journey. The interview guide is provided in the Web Appendix.
AnalysisWe analyzed the 495 single-spaced transcript pages in three stages. We began with narrative analysis, a family of techniques for interpreting narrative data by focusing on sequences of action. As Riessman (2008, p. 11) explains, “Narrative analysts interrogate how and why incidents are storied, not simply the content to which language refers.… Why is the succession of events configured that way? What cultural resources does the story draw on, or take for granted? What storehouse of plots does it call up? What does the story accomplish? Are there gaps and inconsistences that might suggest preferred, alternative, or counter narratives?” Following established practice for interpreting life history narratives (McAdams & McLean, 2013; Riessman, 2008), each member of the research team created a thematic memo for each of their informants including a visual map of the customer journey marking critical incidents. For each incident, attention was paid to its timing, precipitating factors, the way it unfolded and wrapped up, key players, its meaning to our informant, and the informant’s emotional and behavioral response. A different team member validated the original memo writer’s interpretations. During weekly team meetings, the researchers discussed the memos and transcripts in relation to the research question to identify broad themes for later theory development (Strauss & Corbin, 2008). Transcripts were reread and additional memos were drafted multiple times (Birks et al., 2008).
Second, to ensure the thematic and critical incident analyses had extracted the essential lessons from the transcripts, we intensively analyzed a sample of 9 transcripts using Gioia’s (2013) approach for developing grounded theory. We initially identified over 100 first-order categories, later reduced to about 35 after considering similarities. From those and after rereading the transcripts multiple times, we identified nine abstract, second order themes. We situated the themes on the journey maps emerging from the first phase. Following Tsarenko et al. (2019), we then assessed the fit of the emerging themes with the remaining interviews and renegotiated themes to ensure fit with the entire interview set.
Throughout, we referred to the interdisciplinary literature on MI and customer journeys. We also paid particular attention to differences among our respondents. We found only minor differences between the reports of individuals with MI compared to surrogate buyers/parents; specifically, the surrogate buyers were somewhat more likely to report service system failure. Thematic differences across MI severity were also relatively minor; those with more severe MI took longer to recognize the onset as the symptoms were less common (e.g., disabling OCD was seen as a quirk—“she would only drink from the princess cup”—and became quite serious before being recognized as a disorder), were somewhat more apprehensive of finding a solution, and were more likely to assess service system failure. We draw our conclusions from the entire sample and carefully describe dissenting voices.
In our third stage, we conducted member checks with three MI domain experts to confirm the interpretation and authenticity of our findings and to assess the transferability of our interpretations (Strauss & Corbin, 2008).
FindingsOur research investigates how consumers seeking mental illness treatment experience and navigate a prolonged, crisis-ridden, deeply uncertain, and high stakes consumer journey. Participants typically responded to our opening prompt to “Tell me about yourself” with chronologically organized narratives rather than discursively jumping around in time or topic. The chronological response made it clear participants see the entire experience as a journey; indeed, several used the term. Time is linear; progress, however, is chaotic with many starts, stops, and changes in direction.
Our findings reveal a journey emerging in three phases: (1) an invisible embarkation; (2) a long and winding road in search of solutions; and (3) the arrival at an unexpected destination. While this dynamic journey’s three phases are superficially similar to the three phases of the classic journey (i.e., pre, during, post), they are much more complex, as consumers were required not only to make multiple consumption decisions, but, crucially, to take on the overwhelming task of identifying and sequencing these consumption decisions within a complex and often failing marketplace system. As we explicate below, our overwhelmed consumers did not have a detailed master plan, but instead inch forward, often reluctantly, in sensemaking fashion. See Fig. 2.
Fig. 2
Trajectory and navigation of the mental illness turbulent consumer journey
The invisible embarkationOur participants’ MI treatment journeys open with an invisible embarkation because, unlike other journeys, TCJ travelers experiencing mental illness do not realize they are on board until the journey is well underway. Participants described feeling their way forward: first anchoring their experience in pre-journey normalcy, then assigning benign inferences to make sense of discrepant events, until a crisis prompts recognition of the journey.
NormalcyParticipant narratives often began with a pre-journey anecdote demonstrating their normalcy or even exceptionalism. Julia described her daughter who would later be diagnosed with autism and anxiety: “Amanda seemed to be a very typical baby…other than the fact that she was a little bit too smart, and a little bit too [observant].” Julia anchored Amanda’s experience in the days before the onset of MI rather than today and emphasized the baby’s typicality or even “too smart” exceptionalism.
Prefacing the interviews with evidence of normalcy guided our participants’ journeys in two ways. First, our participants’ overarching goal becomes a return to pre-journey normalcy rather than settling for reduced MI symptoms, and the early evidence of exceptionalism made the goal seem reasonable and just. Second, the vivid salience of pre-journey normalcy explains why early ambiguous signals of MI are easily dismissed. Life was routine; there was no reason to anticipate the coming difficulties.
BenignitySlowly, over months or even years, participants became aware something was different. Life was no longer easy, but the differences were minor and, importantly, viewed through a lens of normalcy. Betty recalls her son’s early symptoms of disabling anxiety:
Looking back now, I can see the signs of him asking for help and me not recognizing it as “Help, help!” [I thought], “He’s just stubborn” and “He’s got to learn he can’t always have his own way.” I didn’t give him credit for knowing who he was, and he knew who he was. He knew a big [elementary school] didn’t work. He knew. And I am like, you’re seven or whatever and he doesn’t know shit, but he did. He felt bad about himself. It started, you know, the downward spiral.
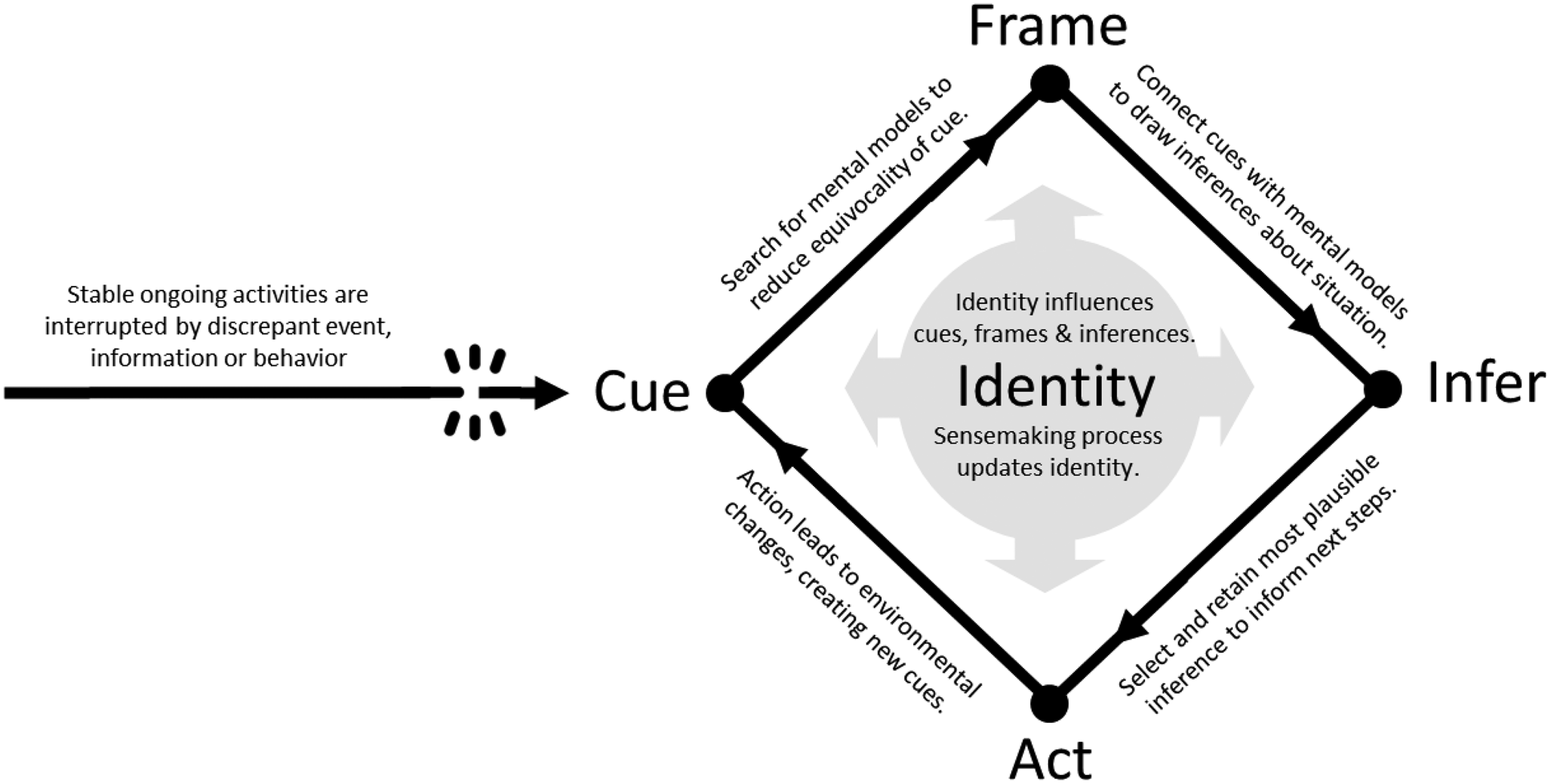
The MI warning signs were ambiguous, and easy to misinterpret. Betty filtered her son’s school avoidance through a normative personality lens (a strong-willed child). Sense makers filter ambiguous cues through preexisting mental frames to form plausible, although not necessarily accurate, inferences that guide action. Betty mistakenly inferred the outbursts were signs of stubbornness rather than emotional pain, and so she responded with discipline rather than treatment. Signal noise drove many of the inferential errors at this early stage. Ingrid’s daughter excelled academically, athletically, and socially before developing a severe bipolar disorder with psychotic symptoms:
Isla was the perfect child… Smart, great friends, no trouble, bubbly personality. In high school, she played varsity basketball, ran cross country, took AP classes, very bright math and science mind. She went to [a highly selective university] and got a bioengineering degree. She was feeling kind of burned out. I didn’t realize the significance at the time, but I noticed changes in her. She couldn’t seem to focus on her classes. She was very dissatisfied with the dean, the professors, and the group projects…She told me, “My heart isn’t in grad school. I want to quit.”
Filtered through the vivid normalcy lens (“the perfect child”), Ingrid benignly interpreted Isla’s ambiguous symptoms as school fatigue and endorsed her daughter’s decision to drop out of graduate school. Vivid situational factors, such as a divorce or a toxic boss, also propelled benign explanations for worrisome, but ambiguous, behavioral cues. Lacey felt “not normal,” but her parents attributed her sadness, argumentativeness, and poor concentration to her father’s second marriage. The tendency to make normative inferences as these participants did is consistent with Luce’s (1998) finding that consumers postpone negative inferences.
Importantly, marketplace actors as well as consumers misinterpreted early clues. Though Katherine raised concerns about her son’s walking and speech delays, her pediatrician dismissed the concern saying, “Let’s not worry about it now because he’s still young. You know, boys develop slower than girls.” Instead of making a timely autism diagnosis, Katherine’s trusted pediatrician benignly chalked up the signals to gendered developmental differences. Our participants’ reliance upon the assessments of family and professionals illustrates social others’ roles in drawing sensemaking inferences (Weick, 1995) and along consumer journeys (Hamilton et al., 2021).
During this early phase, our participants’ concerns were often explained away with plausible explanations provided by medical professionals, family members, or even themselves. In retrospect, participants recognize the benign interpretations as inferential errors, but at the time, they took no action until the escalating MI symptoms became too disruptive to ignore.
CrisisThe eruption of a crisis marks the end of the first phase on the TCJ. As symptoms and actions became unacceptably worrisome, our participants slowly recognized they were, to their surprise, on a journey. JoAnn talks about the crisis launching her son’s TCJ:
Throughout his childhood, there were always ongoing issues and concerns, and then as he’s gotten older there were many incidents of reckless behavior that we chalked up to being a teenager and poor decision-making. Over the last two years, we saw more and more behavior that was concerning, to the point where last year his fiancée called me and said, “I’m really worried about Sam. He just broke up with me. He thinks he’s God. He’s going around saying he needs to give away all of his possessions.” She was very concerned.
This was a crisis: neither Sam’s fiancée nor mother were sure of how to respond, yet his delusions and impulsiveness demanded action. Benignly interpreting Sam’s behavior as teenage indiscretions no longer made sense, and the crisis propelled the family to seek professional care.
Crises occur when an individual lacks the resources to solve a problem, yet its importance demands an immediate response (Eastham et al., 1970). Alice realized her daughter’s behavior was more than “attention seeking:”
She began to talk about suicide. She connected with other kids on Instagram who were flirting with the idea, and she would post things about guns. It was quite frightening. I was worried about keeping her safe. I slept on the floor outside her room, but I knew I couldn’t keep doing that. The responsibility for keeping her alive seemed too big for me.
Alice had been concerned for several months about Addie’s new taste in clothes and her new friend group. Her concerns reached a crisis stage when Addie talked about suicide. Alice first tried to take care of Addie herself, by sleeping outside her door, but soon realized suicidality was beyond her scope and sought professional help.
The precipitating crisis was often life-threatening for those with psychosis, suicidality, or other serious MI. For those like Amelia with processing disorders or other moderate MI, the crisis was more muted:
I started realizing school, reading in particular, was getting harder for me. Math has always been really easy, but then reading would be really slow. And so, it was a struggle in late middle school and all of high school to try to get accommodations from teachers. Some wouldn’t understand and some would make fun of me in front of the class… In science class I was having really terrible anxiety taking tests, so I asked if I could take my tests in the science closet because I would take so much longer than everyone else and then it would be too loud because people would be done, and they would talk. The teacher said terrible things about me.
Amelia’s crisis—her recognition that school demanded more than her resources—came on slowly. The accommodations she sought earlier were no longer sufficient and she was now also grappling with social anxiety brought on by teachers’ and peers’ criticisms.
Recognizing the crisis marks the end of the invisible embarkation and the start of the long and winding road for a solution. Each of our participants recalls the moment they recognized a crisis and became fully engaged. Curiously, none of our participants reported being alerted to MI by a clinician. Instead, they inferred MI when escalating symptoms could no longer be explained benignly.
The first phase of the journey challenges consumers to recognize they are, indeed, on a journey. Three linked sensemaking cycles emerge: (1) anchoring the experience in normalcy, (2) making benign interpretations of disturbing events, and eventually (3) taking action as more extreme events emerge that force an interpretation of crisis. As we unpack in the next section, our participants first turned to the clinical marketplace for help with the crisis. After multiple disappointments, many concluded the marketplace was broken and they, personally, would need to take charge of the journey.
The long and winding roadParticipants started the long and winding road phase of the journey with a goal of returning to normalcy. The job journey literature describes consumers crafting a goal hierarchy to reach an overarching goal like return to normalcy; in this context, a goal hierarchy might include acute care treatment (i.e., find a provider and get medication), longer term care (i.e., join a support group), and lifestyle changes (i.e., daily meditation and seek a less demanding career). Our participants’ goal hierarchies develop over years as they slowly feel their way forward one step at a time and rely on sensemaking to decide what to do next. Small wins and bigger setbacks were common. Throughout, participants described an emotional rollercoaster characterized by Betty as “delusion, hopelessness” interspersed with “hopefulness, and mindfulness” as they initially perceive the situation to be easily manageable, then attribute service provider failure when the return-to-normalcy goal remains elusive, and then, ultimately infer service system failure.
Easily manageableParticipants initially filtered the surprising MI discovery through the familiar medical model frame (Anderson, 1995) and anticipated a relatively rapid return to normalcy after clinical intervention. Fred, for example, expected to manage his daughter’s bipolar illness fairly easily, thinking “it was just a matter of getting the right combinations of medications.” Fred drew on his medical mental model in which a clinician diagnoses and treats a condition, and the problem is resolved. Other participants echoed Fred, inferring their MI would be easily managed, just as physician-prescribed antibiotics eliminate infections and physical therapy rejuvenates a sprained ankle. Families reinforced the idea the condition would resolve with treatment. Abigail described her mom’s assumptions:
I went through therapy with [a specialized dyslexic treatment center]. My mom will not accept I’m dyslexic. If I say I’m dyslexic, my mom looks at me and tells me with the straightest face, “You went through three years of therapy to retrain your mind, so you are not dyslexic. You would not test positive for dyslexia today.” It is a battle.
Abigail’s mother expected treatment would eliminate dyslexia and return her daughter to pre-diagnosis normalcy. Inferences that a return to normalcy would follow structured treatment were common, and participants were puzzled by continued difficulties. As we see next, they held fast to the expectations for an easily manageable condition and concluded the problem must be with the service provider.
Service provider failureInstead of a journey easily managed by marketplace providers, our participants were often baffled as birthdays, graduations, jobs, and other typical life activities were interrupted by recurring MI symptoms. The stakes were high: suicidality, job loss, and school failure. Participants attributed failures and relapses to an individual service provider’s lack of skill or integrity. Jackie cried as she recounted her quest for a clinician to help her son:
We had five psychiatrists, two neurologists and two developmental pediatricians [over several years]. And I had him in a developmental school. 97% of doctors don’t understand bipolar disease in early onset. In fourth grade, well, this psychiatrist thought it was hyperfocus in autism and put him on an SSRI, Lexapro, and within three days he was full-blown psychotic, hearing voices telling him to poke his eyes out. The doctor, you could tell in her voice, was surprised.
Jackie describes sequentially working with more than ten clinicians, each time hoping she found a solution, only to conclude each provider was ineffective. Many other participants described similar experiences in which they would infer service provider failure and churn to a new provider. The effort was monumental, frightening, and highly emotional.
While the pharmacological error Jackie described led her to quickly infer service failure, more often it took months for participants to interpret slowly emerging cues. Helen explains how she finally concluded her son’s psychologist was ineffective:
[My son’s psychologist] kept telling us, “You just have to let him go, don’t give him money, don’t help him out.”…My husband and I were both at a loss of what to do. So over months of struggling with it, we finally gave up. We thought, “OK, maybe the psychologist is right, maybe this tough love approach is the only way for us. We have to cut him off.”… We didn’t help him. He got evicted from his apartment. He ended up on the streets. He went to jail. He got beat up. He would knock on our door for food, and ask, “Why can’t you just let me live at home?” We said no, because that’s what the psychologist said, “No, don’t take him in because you’ll be falling for his trap”…But then I realized the psychologist was puzzled that [despite reaching rock bottom], my son just wasn’t picking up the pieces and taking charge of his life. And I thought, the kid has an illness and you’re expecting him to perform.…Finally, we decide to take him to a new place for treatment. Within not even two days, the new psychologist called to say, “Your son has a mental illness. This is not addiction. Yes, he’s devolved to addictive behaviors but that’s because he’s self-medicating the pain from the mental illness.”
Helen and her husband were mired in uncertainty, “at a loss of what to do.” Initially, the psychologist’s “don’t help him out” directive resonated as tough love; however as new cues emerged—homelessness, jail, and beatings—she grew uneasy with the provider’s advice. Trusting in the professional, she followed the directive until she observed a disturbing new cue: the psychologist himself was surprised his guidance was not working. The new cue led her to a new action, finding a different service provider.
Participants were painfully aware of their limitations in assessing quality, yet the high stakes forced them to do so. Fred asked rhetorically, “How do you know who is a good therapist? Part is a personality issue. But the other is, who has an effective regimen and who just tends not to be effective?” Fred was aware he lacked the specialized skills to judge clinical quality but reluctantly did so. Often our overwhelmed participants described using marketplace quality heuristics to make sense of clinical performance. Claire could not judge quality by looking at outcomes, as she was unsure if the psychiatrist had indeed eliminated her 9-year-old son’s suicidality. Instead, she paid attention to subtle cues.
The psychiatrist wanted his money before the session started. It’s one thing, if my son goes in for a session and then you hand them the check; but this psychiatrist was all about money… Plus, he told me to “plan for the worst and hope for the best.” He was defeatist.
Claire struggled for months to assess the psychiatrist’s effectiveness. The psychiatrist’s unconventional payment procedures did not fit with her mental model in which providers request payment after the service, leading her to infer greediness. His advice to plan for the worst indicated less than full effort and made him untrustworthy. Goal conflict perceptions like this were common. For our participants, the return-to-normalcy goal was non-negotiable; anything less was believed to preclude a satisfying life. In contrast, service providers often viewed success as effective management of the MI symptoms.
Service provider failure extended beyond the clinical marketspace and into related market sectors. Kim’s daughter has an auditory processing disorder:
This year, she had a teacher who did not want to wear [the headset]. Jess went and asked her about it, and she told Jess, point blank, that no, she would not wear it, that she was loud enough as she was, and she would just stand closer to her. I had to step in and write the teacher a message and explain that she’s got an auditory processing [disorder], it’s not the volume that’s the problem, it’s the tuning out the other stuff.
Kim had secured approval for the accommodation; as such, it was mandated by the school. Yet the teacher failed to comply, and Jess could not hear her. The teacher’s refusal jeopardized Jess’s learning, prompting Kim to hold the teacher responsible for the service failure.
Participants expected the journey to be easily managed by a clinician and ancillary providers. Instead, many participants, and especially those with serious mental illness, experienced repeated setbacks. They inferred service failure, blamed the provider, and responded by churning to new providers.
Service system failureAfter often years of disappointing experiences with individual service providers and escalating symptoms including suicide attempts, school failure, and social disconnection, participants began to look beyond individual service provider failures and inferred service system failures. Many bewildered participants concluded the fragmented clinical system is dysfunctional, Ingrid notes:
I feel like the professionals are throwing darts at walls sometimes when it comes to medication. We try this [prescription], then try different dosages, then roll off, then try that one. Isn’t there like a better method? Each new doctor starts messing with dosages and medicines. Is there a science to this or is it witch doctoring?
The seemingly haphazard medication changes signal to Ingrid both individual provider incompetence and, even more disconcerting, pharmacological system incompetence. Her “witch doctor” interpretation is not simple provider error, but a system failure. It is possible the prescribing psychiatrists were following best practice treatment pathways, that is, first try this, then that. However, participants did not receive, nor know to ask for, the diagnoses or treatment pathways that would shape their consumer journey. “It’s hard to get clear cut, concrete diagnoses and information,” Alice observed. As a result, information scarcity magnified the uncertainty.
Unrealistic resource integration responsibilities also led participants to infer system failure. As Fred explains, “Your primary care doctor coordinates your oncologist, your cardiologist, and this and that. And yet for psychiatric care, the patient is coordinating it themselves or their mom and dad are. Right. And how are we equipped to do that?” Fred resented the responsibility, noting other healthcare specialties coordinate care. He was also fearful his clumsy care coordination would keep his daughter from getting well. Fred lacked the goal setting, learning, and evaluation skills fundamental to effective resource integration (Hibbert et al., 2012).
Assessments of service system failure extended beyond clinical medicine and into related marketplaces. Breakdowns in the social service system made it difficult for Kristy to identify, evaluate, and qualify her foster son for MI treatment services:
It was exhausting to try to get to the bottom of it because of our lack of access to information. Because he’s in foster care and he’s in our physical custody, but he’s not in our legal custody, we are not entitled to have a copy of the IEP [Individualized Education Program] and other information I think normally you might use to help guide your decision-making process. Unique to our situation was the added layer of trying to figure out what was the diagnosis, what was the basis for the diagnosis, what were the other conditions going on at the time the diagnosis was made plus having to work with so many people: his special ed teachers but also other school officials, his therapists, social worker, etc.
Kristy was frustrated. She was responsible for orchestrating special education, therapy, and ancillary services, yet the system failures left her without the information she needed to make decisions related to her foster child’s MI treatment and academic support. Importantly, the system failures affected not only the quality of her decisions but left her “exhausted.” Participants who inferred system failure were initially frozen and unsure of how to proceed. They were slow to conclude system failure and did so only after multiple justifying experiences.
Our findings reveal three sequential cycles propelling the difficult middle stage of the TCJ for MI treatment. Initially, participants draw faulty inferences by comparing the unfamiliar journey with more familiar experiences, and expecting a clinician to guide them back to normalcy. The mistaken assumption of a straightforward return to normalcy led to disappointment; participants responded with new inferences about individual service provider failures leading them to switch providers repeatedly. Eventually, many participants concluded the entire system was incapable of delivering their desired return-to-normalcy outcome. This realization marked the transition to the third phase of the journey: an unexpected destination. Participants reaching the third phase radically accepted the idea that their return-to-normalcy goals might remain unmet and recognized that they, rather than service providers, must take the lead in managing their care.
An unexpected destinationParticipants reaching the final phase found themselves arriving at a destination they could not have foreseen. The impact is profound. Those who reached the third phase of the journey are distinguished from those still in the middle phase by their radical acceptance of a new normal in which the return-to-normalcy goal might never be achieved and in which they, rather than the marketplace, would orchestrate the journey. As they reflected on the difficult journey, many inferred a just world violation leading them to crusade for system improvements. Many described a new wisdom emerging from their grief and anger that allowed for personal transformation.
New normalParticipants described radically accepting a new normal in which symptom management replaces the firmly held return-to-normalcy goal and in which they, rather than an elusive ideal clinician or clinical system, orchestrate care. Simon describes his future with hearing loss as a death, reflecting, “I think about it from the time I wake up ‘til the time I go to bed. There is no escaping it.” For Simon, the new normal is not attractive, but like death, permanent and real. Radical acceptance is a dialectic concept involving accepting the world as it is, as undesirable as it may be (Robins et al., 2004). It does not imply giving up a search for better outcomes or thinking today’s reality will not change. Instead, “reality is truly fully embraced, even welcomed, without judgment or escape, delusion or rationalization, and without rigid attachment to nonreality or wishful thinking, and attempts to change reality in the present moment” (Fruzzetti & Erikson, 2010, p 350). It is radical because the reality is especially difficult to accept. Helen, whose son lives in a group home in a distant state, radically accepted the chronic nature of her son’s psychosis and the likelihood of relapses:
There is a point where he’ll be challenged; it’s too much, and then he plummets. He packs his bags and goes to the next place. That’s the pattern. But we have a better relationship. We understand what’s going on with him…It’s been nine years and we kind of see that he’s always going to struggle emotionally and financially.
The repeated setbacks despite intensive treatment have led Helen to infer a new normal in which her son’s MI will persist. The radical acceptance phase involves accepting the disappointing reality rather than flailing against the system, and leaning into the intrinsic uncertainty. In this way, it is different from the earlier intense focus on service failure.
By accepting reality without judgment, participants developed a greater sense of self-compassion, self-acceptance, and often a fresh perspective on their MI. Wade, who has ADD and dyslexia, reflects on his public speaking skills:
My brain just works differently. For me, I never had a note sheet in front of me. I would always just talk openly with my hands. I noticed a lot of [other presenters] would try to do that and walk around and talk like I would. They were trying to mimic me, but really couldn’t. My marketing teacher told me my presenting style represents Steve Jobs, where he could just go up there and just talk. She’s like, ‘You have that same kind of vibe.’
Wade credits the same “brain” that creates reading struggles with being the source of his superior public speaking ability. He accepts his neurodiversity as reality. By shifting his goal from normalcy to acceptance, his sense of control increases.
Participants also radically accepted they, rather than the marketplace, must take charge of resource integration along the journey. Claire, who had originally believed resource integration responsibilities were beyond her capabilities, described radically accepting the role of care coordinator for her teenage son after a second, nearly fatal, suicide attempt.
The professionals, they’re not driving the boat. They drive the boat when there is financial benefit. We have a treatment team meeting every five weeks. It costs me $800 to get the psychiatrist, therapist, and family therapist together. Right now, family therapy doesn’t seem to be working. So, I think: would that $150 be better with a therapist that works in parent coaching to help me guide him? Or would it work better with an addiction counselor?
They put him on lithium. The way I look at it, and I’m not knowledgeable, but I think my son has thinking errors. He did intensive neurofeedback. I wanted him to have TMS, transcranial manipulation. Or ECT. Or something like that because they might help. But they put him on lithium. My son’s issues are thinking errors, perceptions. Meds can’t change that. New neuropathways can change that….
Claire schooled herself in conventional and alternative therapies and, after many traumatic years on the journey, she has radically accepted the role of care coordinator for her son. Notably, she remains cognizant of her knowledge limitations, but she is beginning to be the proactive project manager described on other job journeys, instead of expecting the providers to take charge. Often our participants evolved to radical acceptance following a major incident, breaking point or discrepant cue, as did Claire following a frightening suicide attempt and Helen after exhausting all other solutions.
Not all participants reached radical acceptance even after years on the journey. Fred invested “a couple hundred thousand dollars” in conventional and alternative therapies and advanced pharmaceutical, diet and exercise regimes for his young adult daughter. He despaired:
We still don’t know what to do. And I guess we have been just hoping that the specialists would be able to come up with a combination of drugs that puts her in a good enough place that she can hold a job and be reasonably healthy. We haven’t got there. And my wife and I can’t keep doing this.
Fred’s anguish is palpable. He is worried about his very ill daughter yet knows he and his wife are running out of the financial and emotional resources to continue the journey. Unlike Fred, participants who reached radical acceptance mentally stepped back from their journey. Their new perspective offered a deeper acceptance of the lifelong nature of the journey and shifted attention from fighting against the system to working to change the system.
Just world violationOur participants expected a clear, collaborative, and productive journey for MI treatment. Instead, their narratives were saturated with grief over unmet expectations, service provider shortcomings, system failures, and their own unintended mismanagement. Joyce noted, “I mean, that’s the worst part is that, as a parent with a kid with mental illness, half the time you have no idea if what has worked before is going to work again. Because there aren’t hard and fast rules.” Joyce grieved the unpredictability of MI relapses and longed for clear rules and a clear map of the journey. While Joyce decries the disorder, Julia and many other participants, blamed the market stating, “Therapists say she is not doing what they are asking her. No, [the therapists] are not effective in getting her to do what she needs to do.”
The journey has been unjust and unfair in the eyes of Joyce, Julia, and most of our other participants. The widely held belief in a just world—“good things tend to happen to good people, and bad things to bad people”—helps maintain a sense of stability (Furnham, 2003, p. 795). The perceived marketplace failures violated our participants’ sense of fairness by saddling them with a prolonged, needlessly difficult journey.
The inequity ignited a passion to help others on the journey and even to reform the system. Eileen is self-publishing a book on her alcoholism journey “because it’s unconscionable what happened to me.” She hopes to reduce the stigma by showing how trauma led her previously sober self to alcohol. Others like Helen seek to mentor newcomers, “Today I focus on trying to help other people, passing the knowledge and information and experience of what we’ve been through, so that others don’t have to suffer the way we and our child have.” Brittany created a Facebook group in middle school called ‘Learning Differences are the Best,’ comprising friends and a broader network who also had learning differences. Through confiding and uplifting each other, the group became the support community she had longed for on her journey. Crusading to improve the system paved the way for our participants’ personal transformation. We see this through the expression of a deeper wisdom.
WisdomOur participants’ radical acceptance of the new normal and processing of their just world violation led many to personal transformation prompted by wisdom gained from the life changing experiences. Eileen rejects the alcoholic label because it “minimizes and restricts and twists [one’s] identity to an illness;” instead, her identity is “vast.” She reframed alcoholism from a moral failing to an endocrinological and neurochemical disorder. Her personal transformation emerged from the inequity experience on the journey; in her case, being labeled as an addict and reduced to an illness. Others echoed Eileen’s transformation brought about by lived experiences in crisis and uncertainty—experiences different than those experienced on a traditional marketplace journey. Participants emphasized valuing inner peace, inherent personhood, relationships with others, and rejecting shame. Danielle reported:
I used to ask myself every day, what did I do to cause this? Did I do something when she was in utero? Did I do something during her first years of life? Is there something I did that caused this? Now, so many doctors have said to me, “No, this is who she is.” So, I have tried not to take on the stigma and just be more of an advocate or an activist and say, “Accept your kids as they are.”
The Sisyphean quest for normalcy combined with repeated marketplace disappointments created a sense of shame and chaos. Shedding the skin of stigma empowered Danielle to practice self-acceptance and to advocate self-acceptance to others. Consumers’ beliefs about their personal transformations lends support to Kapoor and Belk’s (2022 p. 197) prediction that “coping with adversities can not only help in learning compensatory strategies to employ in the face of specific hardships, but also becomes a source of strength and confidence for facing subsequent challenges in life.”
The final stage of the MI treatment journey is shaped by three key sensemaking cycles. First, participants come to terms with a new normal, recognizing the return-to-normalcy goal may never be fully achieved and they, rather than the marketplace, must take control of their journey. Through radical acceptance, participants gain a greater sense of agency over their lives and their treatment experiences. This realization often triggers a sense of injustice, sparking a crusade for systemic improvements. Finally, participants find wisdom through the grief and anger they’ve experienced, leading to personal transformation. Importantly, reaching this unexpected destination is not the end; rather, it marks the beginning of a new journey in which a new goal replaces the return-to-normalcy goal (Table 4).
Table 4 Using sensemaking to move forward on the turbulent consumer journey
Comments (0)