
Remember me
The statistical analysis validates our hypothesis that patients with the SLC6A4 SS and HTR1A rs6295 GG (SS-GG) are overrepresented (+74.61%) to a statistically significant degree (p = 0.003) in our disability cohort and may be more likely to fail treatment with a first-line medication for anxiety and depression (i.e., SSRIs). Results additionally revealed that those with allelic combinations of SS-CG, SS-CC, SL-GG, LL-CG, and LL-GG were also overrepresented (+40.68, +2.95 +3.68, +0.86, and +30.96%, respectively) in the studied disability cohort.
The presence of a homozygous C variant at HTR1A rs6295 is consistently underrepresented in the disability cohort except for in the presence of the homozygous S variant, while the same is not true of the L allele of SLC6A4. Additionally, the individual presence of one G allele at rs6295 is more overrepresented than the presence of just one S allele at SLC6A4, indicating that the G allele is likely to be more harmful than S allele in impeding SSRI therapeutic effect. This is further highlighted in the comparison of LL-GG being markedly more overrepresented than SS-CC indicating that the G allele is more impactful in negatively affecting therapeutic response to SSRIs, or that those with SS-CC variants are less likely to experience anxiety and/or depression.
LL-CC, SL-CC, and SL-CG are underrepresented. This is in line with previous studies indicating that the C allele of HTR1A rs6295 may improve response, whereas the G allele may harm response [7].
The presence of one L variant of the SLC6A4 in a patient with one C variant at HTR1A (SL-CG) is a significantly underrepresented (−37.62%, p = 0.000) combination in the disability cohort, despite being the most common and statistically likely combination within the European population. This indicates that the presence of just one L allele of SLC6A4 with the presence of one C allele is sufficiently redeeming to potentiate drug response.
Where the results diverge is pertaining to LL-CG; this combination is overrepresented very minimally and insignificantly by 0.86% in the disability cohort. This may not be a failure of the homozygous L combination’s ability to compensate for the presence of a G allele at rs6295, but perhaps due the limitation of comparing results as against the general European population, which may encompass drug-resistant individuals, as opposed to a cohort of drug responders, which are difficult to access. Alternatively, it is possible that those with LL serotonin transporters in combination with one or more G alleles at HTR1A rs6295 may require higher doses for sufficient (80–90%) SLC6A4 occupancy due to the high SLC6A4 expression of LL, such that serotonin levels are maximally increased and able to apply desensitization pressure to regulate the highly expressed autoreceptor. This would also justify LL-GG being more overrepresented in this study than LS-GG.
A meta-analytic study from Kiera Stein et. al. indicates that those with SS variant serotonin transporters experience a higher side-effect incidence and decreased response to SSRIs [3]. This may be due to the lower availability of serotonin transporters for blockade. Some of these studies reveal that increased dosing results in the same therapeutic effect as those expressing the LL variant [11, 12]. At higher SSRI doses, the maximal number of serotonin transporters are occupied, and thus therapeutic success is achieved, albeit at the expense of increasing the likelihood of adverse events, which would account for the moderately weaker effect of one S variant at SLC6A4, relative to one G variant at rs6295.
Currently, CPIC (The Clinical Pharmacogenetics Implementation Consortium) does not provide any actionable recommendations pertaining to SLC6A4 and SSRI therapeutics, though SLC6A4 has shown positive association results in meta-analytic studies as well as in this study, warranting continued research to solidify findings and determine evidence-based implications for clinical use [13].
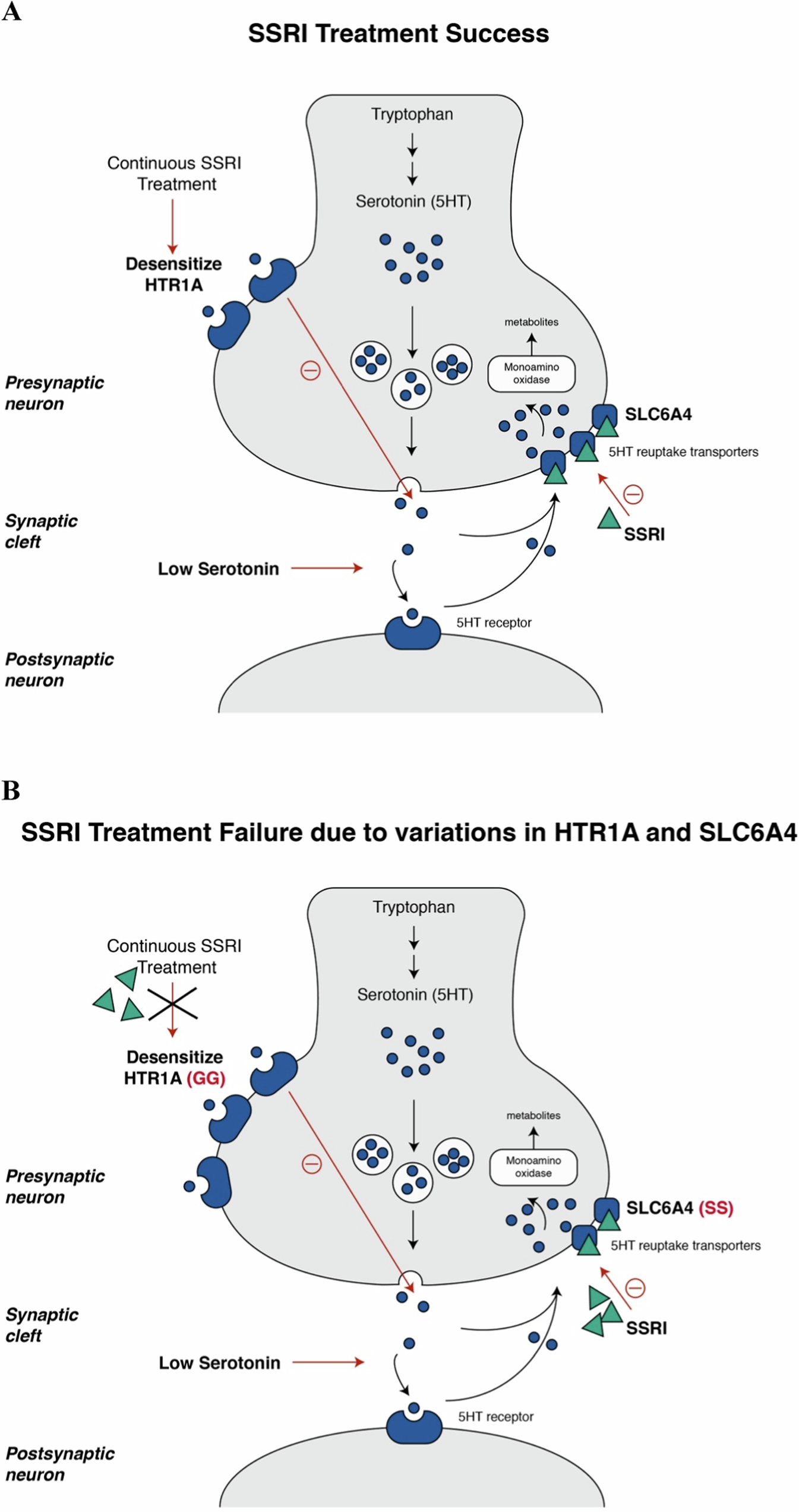
Various studies have implicated the 5-HT1A autoreceptor in the response to SSRIs [14, 15]. As per Richardson- Jones et. Al 2010, mice modified to express lower levels of 5-HT1A autoreceptors show a significantly superior response to Fluoxetine (SSRI) treatment as well as individuals with a C allele at rs6295 [16]. Extracellular 5HT levels were markedly increased in these mice compared with high expression 5-HT1A mice, as is observable in Fig. 1A [16].
Fig. 1: Interactive effects of HTR1A rs6295 and SLC6A4 polymorphisms on SSRI treatment.
A HTR1A rs6295 CC polymorphism and SLC6A4 SL or LL may result in significantly increased therapeutic response to SSRIs. The small blue circles represent serotonin. The green triangles represent an SSRI. Once an SSRI occupies and blocks the SLC6A4 serotonin re-uptake transporters represented by blue squares, there are increased levels of serotonin in the space between the pre and post synaptic neuron as well as heightened interaction with post-synaptic serotonin receptors. Initially, due increased serotonin transmission, and through a negative feedback mechanism, pre-synaptic HTR1A autoreceptors then limit the amount of serotonin leaving the neuron. Eventually, through continually increased cleft serotonin levels, the HTR1A autoreceptors are desensitized, allowing serotonin to flow freely out of the neuron, resulting in SSRI therapeutic success. B HTR1A rs6295 GG polymorphism and SLC6A4 SS polymorphism may result in significantly decreased therapeutic response to SSRIs. The small blue circles represent serotonin. The green triangles represent an SSRI. Once an SSRI occupies the few SLC6A4 serotonin re-uptake transporters of an individual with the SS low expression variant, the increase in levels of serotonin in the space between the pre and post synaptic neuron is minimal. Additionally, due to slight increased serotonin neurotransmission and through a negative feedback mechanism, HTR1A autoreceptors limit the amount of serotonin leaving the neuron. Due to an increased number HTR1A autoreceptors in rs6295 GG carriers, this minimal change towards slightly heightened serotonin levels, is insufficient to desensitize the function of HTR1A autoreceptors, thus, the change in neurotransmission is weak, and the SSRI fails to be therapeutically effective.
The heightened HTR1A autoreceptor expression of G allele carriers impede an SSRI’s ability to desensitize this receptor through consistent reuptake inhibition and increased cleft serotonin levels, as is observable in Fig. 1B [14].
SSRIs primarily modulate mood through 5-HT1A heteroreceptors [17]. 5HT interaction with HTR1A heteroreceptors in the post-synapse modulates mood and has a negative control on NMDA activation in the dentate gyrus and on mature granule cells, also activating ERK, suppressing GSK3B, and ultimately playing an important role in neurogenesis [18]. G allele carriers have fewer post-synaptic 5-HT1A receptors [5]. This dual effect of 5-HT1A receptors contributes to the scope of its individual effect, which as per our data analysis is more significant than that of one S allele of SLC6A4.
Thus we postulate that the L allele of SLC6A4 is possibly less protective than the C allele of 5-HT1A, or rather the S allele of SLC6A4 is less harmful than the G allele of 5-HT1A. Patients with either a homozygous SLC6A4 SS or HTR1A rs6295 GG and more specifically the combination of both these gene variants are less likely to respond to SSRI monotherapy as first-line treatment for depression and/or anxiety at standard doses.
Comments (0)