
Remember me

Sexual and reproductive health (SRH) is currently one of the major public health concerns, especially for the maternal and adolescent health and wellbeing. It is used as an umbrella term for individuals to make their own free and informed choices, and have control over their sexual and reproductive health and lives so that they can become free from coercion, violence, discrimination, and abuse [1]. It also includes the availability, accessibility and quality of sexual and reproductive health care services that can contribute to their health and wellbeing [2, 3]. The global health and human rights communities have proactively worked for decades to define and advance SRH, encountering both advances and considerable setbacks [4]. Moreover, women’s sexual and reproductive health rights is the obligation of a state to respect, protect and fulfill rights related to women’s sexual and reproductive health.
Globally, 60% unintended pregnancies ended in abortion and 97% of them occurred in developing countries [5, 6]. Half of the abortion conducted in unsafe manner, that resulted in the maternal morbidity, and mortality associated with temporary or permanent reproductive disability [7]. A recent nationwide survey revealed that 29 per thousand women performed abortion in 2014, where most of them suffered complications and 33% of them required facility-based treatment and comprehensive post abortion care [8]. Most of the treated complications were hemorrhage, incomplete abortion, shock, sepsis and uterine perforation [8]. Moreover, abortion-related mortality increased by 7% in 2016 from 2010 [9].
In Bangladesh, providing quality reproductive health services and ensuring access to these services for people in lower socioeconomic tiers are major public health challenges. The scenario is comparatively worse for the urban poor women than the rural counterparts. These settings were characterized by a place that congested with overcrowded people, high fertility rates, unwanted pregnancies and unplanned births, limited access of healthcare services and many more health deprivations [10,11,12]. Moreover, apart from the adolescents living in poor settlements, significant gaps remain in obtaining SRH information from migrants and internally displaced persons [13], and nearly 52% of the migrated women living in the urban poor and marginalized settings [14]. For example, one out of ten married adolescent women living in those marginalized settings reported having heard about emergency contraception methods [15], but lacked awareness on family planning methods. Consequently, inconsistent use of family planning methods occurred and resulted in unintended pregnancies among adolescent women [16, 17]. Moreover, the patterns of discrimination and sexual violence, irregular contraceptive use and family planning access is higher in marginalized urban areas which resulted in an increasing risk of unintended pregnancies [18,19,20]. Besides, these settings suffered from a lack of SRH services and supplies due to overburden and disruption of healthcare provision [16, 21]. Hence, these settings increase the vulnerability of women and adolescent girls to incomplete and unsafe abortion. Therefore, the abortion rate is higher among the urban poor women in Bangladesh.
Major barriers to accessing safe abortion include lack of knowledge about reproductive health, contraception, and available abortion services [22,23,24,25]. Bangladesh Demographic and Health Survey 2018 reported that about 70% ever-married women heard about menstrual regulations [26]. Women in urban slums often have very low levels of SRH education, which is influenced by the socio-cultural factors, familial settings, and past reproductive experiences [27, 28]. Furthermore, cultural taboos hold them back from discussing sexual issues explicitly with their parents and partners [21]. However, the main sources of these information were parents, in-laws, husband, health personnel and teachers [29]. Study also suggests that poor level of SRH knowledge increase the risky sexual behavior, less use of family planning methods, and increased risk of abortion [22, 23, 29, 30]. Due to these low access to health facilities and cultural rigidness, many urban abortions conducted in unsafe manner [24, 25, 31, 32]. Moreover, national policy and health entitlements often reflects the low access to SRH services and information, such as lack of comprehensive sexual education or contraception for adolescents; in addition, particular SRH services for abortion are criminalized [8, 25]. Therefore, the lack of sexual education translates into lack of contraceptive use and will be subject to unplanned pregnancies resulted in unsafe abortions and sexually transmitted infections [33, 34].
There is a dearth of studies focusing the knowledge and awareness regarding the slum population, especially women. However, some studies have been indicated a lack of awareness on sexual health of slum population- including women [11,12,13,14,15]. Particularly, the study gaps were limited to the coverage of inclusive, vulnerable and lower communities and abortion-related knowledge and awareness [13]. Besides, women who experienced abortion should be aware of the SRH rights and services irrespective of sociodemographic clusters [35]. These rights have not been recognized to their maximum potential in aborted women living in the urban poor and slum area. Therefore, this study aimed to determine the magnitude and predictors of SRH knowledge among the slum women who had any abortion.
Methods and materialsStudy setting, design and periodFor this study, a cross-sectional survey was designed to assess the SRH knowledge among the married women aged < 49 years living in slum areas. This study was conducted in five slum areas of Dhaka (North & South) and Gazipur City Corporations which was under the Urban Health and Demographic Surveillance System (UHDSS). Dhaka North City Corporation includes the largest slum area- Mirpur and Korail, while Dhaka South City Corporation includes- Dhalpur and Shaympur, and Gazipur City Corporation includes- Tongi and Ershadnagar slums. Since 2016, International Centre for Diarrhoeal Disease Research, Bangladesh is running the HDSS to collect and monitor the demographic and health related parameters in the selected area. This survey was conducted in November 07–December 26, 2021.
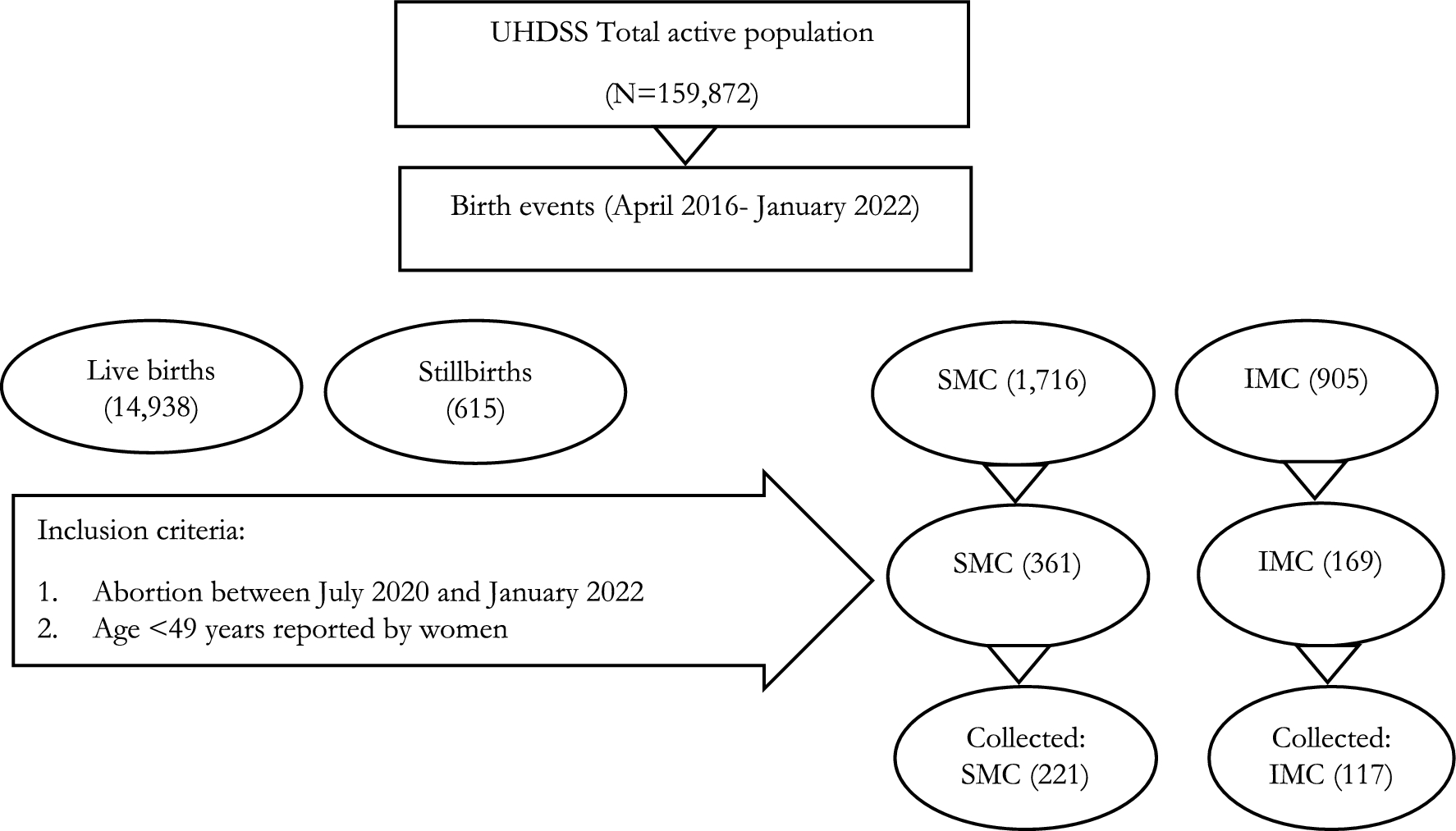
Study population and samplingSince the UHDSS started, a total of 18,174 birth events were recorded, among them 82.2% were live births, 3.4% still births and 14.4% were aborted (spontaneous: 9.4% and induced: 5%). Participants of this study were selected by following criteria: (a) any married women entered at reproductive age (≤ 49 years) listed in the UHDSS; (b) participated in any birth events; and (c) had undergone any sorts of abortion between July 2020 to December 2021. Therefore, 530 married women were included for the survey. Following the sensitivity of the study contexts, currently married women (age ≤ 49 years) who were consented to participate, communicated and not migrated (both in- and out-migration) during the study period were interviewed. Total of 338 women were interviewed successfully and they were included in the study (see Fig. 1). Due to sensitivity of the study context and high migration rate in the urban slums, the response rate (63.77%) was low.
Fig. 1
Participant selection process and sample of the study. UHDSS: Urban Health and Demographic Surveillance System, SMC: Spontaneous miscarriage, IMC: Induced miscarriage
Study tools and questionnaireParticipants were interviewed using the predefined semi-structured survey questionnaire. The focus of the questionnaire was understanding the SRH perspectives of married women with experience of abortion living in the urban slums, existing accessible services to address sexual and reproductive concern for promoting SRH in urban health- especially for those poor women. The questionnaire was organized by literature searches [22] and adjusted on the context of Bangladeshi urban slums in following order- a) Socio-demographic information, b) Reproductive health and history, c) Knowledge on sexual and reproductive health [36], d) History of menstrual regulations (MR) and post abortion counselling/care (PAC), e) Barriers to access MR and PAC. The original survey questionnaire was first prepared in English. The questionnaire then reviewed by the externals (experts from icddr,b team and RHSTEP) and icddr,b’s ethical and research review committees.
Data collection procedures and quality assuranceAn interviewer-assisted semi-structured questionnaire was administered to gather the data through face-toface interviews. The English questionnaire and study tools were translated into Bangla by language experts for data collection. Consent were taken from individuals with age greater than or equal to 18 while for under-aged women, assent were taken from legal guardians including their husband, mother (or in-laws). As the respondents were urban poor, considering their low level of education, the interviewer assisted to read-out the questionnaire for her with possible options and record the answers provided by the respondents. Any discrepancy was probed and re-read for case specific respondents for record the actual scenario. Interviewers were trained for these settings and any conflicts were addressed discussion with the project member.
Data were collected in tablet-based application (SQLITE) in pre-coded format of the semi-structured questionnaire. Collected data from the field were checked by the field research supervisor incorporated with two data management team. Later, with the help of main investigator, and analyst rechecked the consistency across the variables. Any anomalies were reported to the field research supervisor, and the data were verified from the field level.
Study variablesDependent variables We considered sexual and reproductive health (SRH) knowledge as the main dependent variable that was assessed by 14 items adopted from World Health Organization [37] for evaluating 1. sexual conduct (3 items), 2. condom use and attitude (1 item), 3. STDs and HIV/AIDS (2 items), 4. emergency contraception (1 item), 5. safe abortion and care (1 item), and 6. complications of unsafe abortion (6 items). Respondents answered in “true”, “false” and “do not know”. For each item 1 point was given to correct responses and 0 to incorrect or “do not know” responses. Aggregated scores were converted into percentage and categorized into poor (< 50%), intermediate (51–70%) and good/high (> 70%) [38].
Independent variables We considered the socio-economic, reproductive health and abortion related information as the independent variables that were found in the previous studies [23, 39,40,41,42,43,44,45]. Age of the women (< 20 years, 20–29 years and 30 + years), educational status (no education, primary, secondary and higher), occupation (housewives, garment worker, other workers), wealth index (poorest, poorer, middle, richer, richest), duration of marriage (0–5 years, 6–10 years and 10 + years), age at marriage (< 18 years, 18 + years), experience of stillbirths (yes, no), experience/utilization of post abortion family planning (FP) counseling (yes, no), use of FP methods (yes, no), consult with partner about FP (yes, no), exposed to violence (yes, no). The wealth index was scored based on the dichotomously coded dwelling items (e.g., presence of chair, dining table, khat/bed, chowki, almirah, sofa set) and owner’s assets and durable goods (e.g., having radio, television, refrigerator, mobile phone, electric fan, watch, rickshaw, computer, sewing machine, cycle and motorcycle). The principal component analysis was used to calculate the factor score of each variable and the index is constructed as a weighted sum of these items. The index scores were ordered ascendingly and classified into five quintiles as poorest, poorer, middle, richer, richest [46].
Data analysisDescriptive data were presented in frequencies and percentage distribution for categorical variables, and mean, standard error, range and 95% confidence interval were reported for continuous variables. Participants sociodemographic information were assessed by the major geographic locations (City Corporations). A bivariate analysis was conducted using chi-square to assess the sociodemographic and reproductive health-related factors of SRH knowledge. Factors with p-value < 0.25 were considered as candidate variables for the multivariable analysis. Similar process of selecting candidate variables for identifying suitable determinants can also be found elsewhere [47,48,49]. Finally, the multinomial logistic regression model was conducted with available candidate variables to identify the predictors by controlling confounding variables. We also consider two variables from the expert view point. Determinants with 5% level of significance in the model were reported as risk ratio (RR) and standard error (SE) with 95% confidence interval (CI). All the analyses were performed in STATA windows version 15.0 (Stata.corp, TX).
Comments (0)