
Remember me

Out of the 152 health facilities included, 54.3% were from Jinja (Table 1). Most facilities were located in non-slum areas (79.2%), and the majority were PFP facilities (73.9%). According to level of facility, drug shops were the most prevalent, comprising 38.4% of the sample, followed by clinics at 31.5%.
Table 1 Characteristics of 152 health facilities included from Jinja City and Iganga MunicipalityHealth workers were interviewed from each included health facility, except for one clinic in Jinja. Of the 174 health workers interviewed, most (68.3%) were female, and 44.5% were between the ages of 21 and 30 (Table 2). Most participants (67.3%) were either married or cohabiting, and 32.4% identified as Anglican. Nearly half (46.1%) were employed in higher-level health facilities, while only 5.0% worked in pharmacies. Nurses and midwives formed the largest professional group, with enrolled nurses/midwives representing 40.3% and registered nurses accounting for 26.7%. In contrast, only one pharmacist and one pharmacy technician participated, while CHWs constituted 12.1% of the sample. Furthermore, 67.7% of the participants had completed their basic training over four years prior, and nearly half (49.3%) reported working at their current health facility for one to four years. Majority (67.4%) of these health workers worked in facilities in Jinja.
Table 2 Health worker characteristics (N = 174)Availability of family planning servicesOf the 152 facilities included, 145 (94.2%, weighted proportion) reported offering at least one family planning service. Among these facilities, only 8.9% reported providing at least one permanent method, 34.2% provided long-acting reversible contraceptives (LARCs), and 36.1% offered LARC removal services. Additionally, 58.2% provided counselling on at least one natural family planning method, while nearly all (99.0%) offered at least one short-acting method (Table 3). Looking at specific methods, only 6.9% of facilities offered vasectomy, while 8.0% provided female sterilization. In contrast, most facilities supplied male condoms (95.5%) and combined oral contraceptive pills (85.4%). Injectable DMPA-IM was available in 76.5% of facilities, while self-injectable DMPA-SC was offered by 66.9%. Additionally, 21.3% provided IUD insertion, and 23.6% offered IUD removal services.
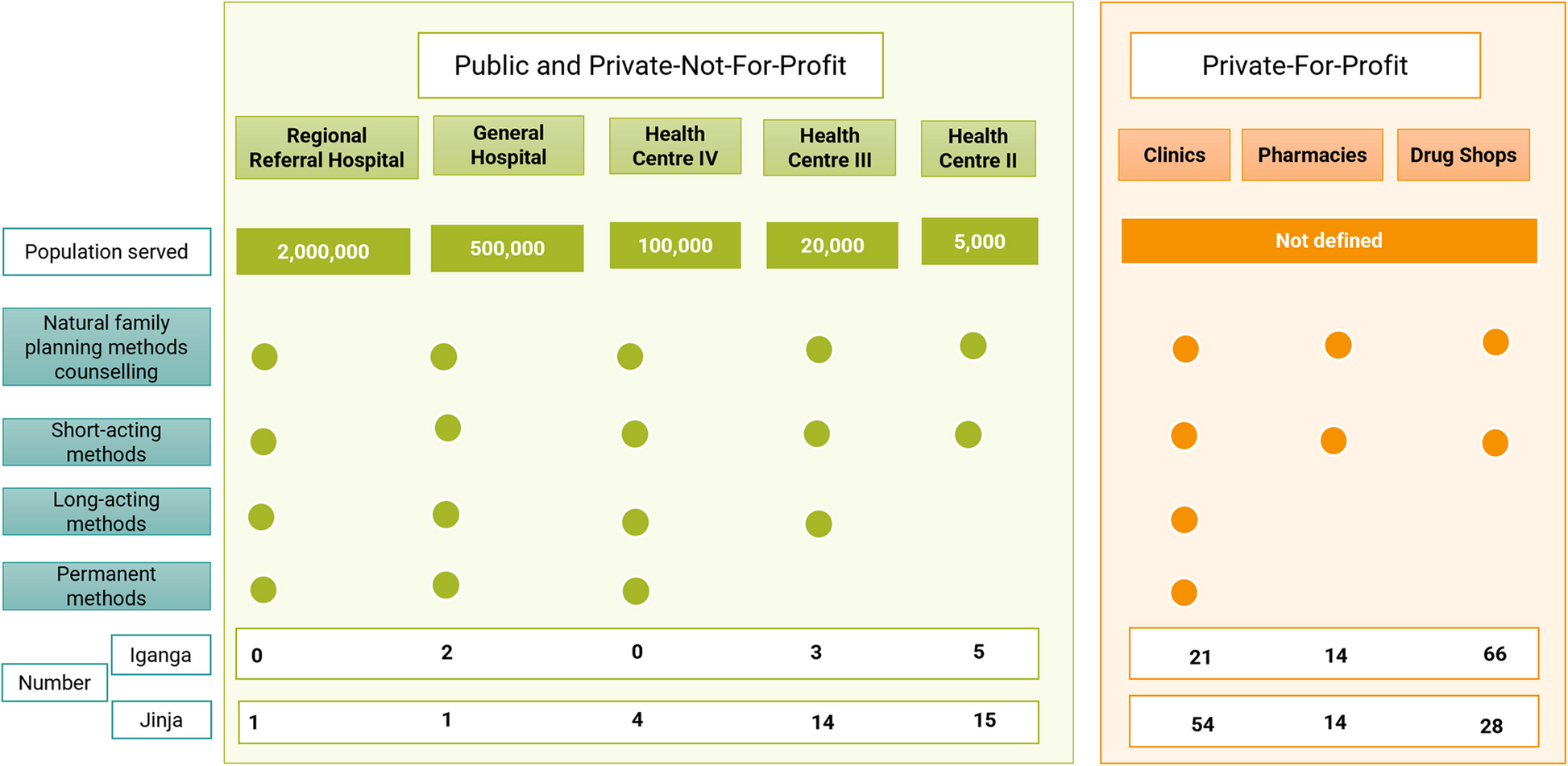
Table 3 Proportion of health facilities that reported providing the different methods by level of care (N = 145)Comparing availability across different levels of care, higher-level facilities reported the highest availability for most family planning services. These included male condoms, oral contraceptive pills, DMPA-IM, UD insertion, and IUD and contraceptive implant removal which were offered in all higher-level facilities. HCIIIs also had high availability of male condoms (87.5%) and combined oral contraceptive pills (87.5%), though availability was lower for methods such as IUD insertion (43.7%) and female sterilization (0.0%). HCIIs also had high availability of male condoms (95.0%) and combined oral contraceptives (80.0%), but a lower availability of IUD insertion (25.0%) and female sterilization (5.0%).
Pharmacies and drug shops primarily stocked short-acting methods. Male condoms were available in all pharmacies and 98.1% of drug shops, while emergency contraceptives were available in 93.0% of pharmacies and 72.8% of drug shops. Injectable contraceptives—DMPA-IM and DMPA-SC—were available in 52.5% and 40.5% of pharmacies, respectively, and in 67.2% and 56.7% of drug shops. Notably, 8.9% of pharmacies and 1.9% of drug shops reported providing LARCs. Clinics exhibited moderate to high availability of most family planning methods, particularly short-acting methods such as male condoms and emergency contraceptives (91.7%) and DMPA-IM (93.5%). However, availability of long-term methods was lower compared to higher-level facilities. Specifically, IUD insertion was available in 40.2% of clinics, contraceptive implant insertion in 56.8%, and IUD removal in 45.2%. Permanent contraceptive methods were least available across all facility types (8.9%), with female sterilization provided in only 16.8% of clinics and vasectomy in 10.1%.
Staff and guidelinesStaff trainingAmong the 145 facilities offering family planning services, 57.8% reported having at least one staff member providing family planning trained in some aspect of family planning within the past three years. Training levels varied by ownership type: only 50.4% of PFP facilities had a trained staff, compared to 75.0% of public facilities and 83.6% PNFP facilities.
From the health worker survey, 261 out of 274 respondents (95.3%) were from health facilities providing family planning services. However, out of the 261, few had received recent refresher training on family planning: 6.5% on tubal ligation, 7.1% on vasectomy, 20.2% on program management, and 26.3% on IUD procedures. Similarly, about a third had training in general clinical skills (37.8%), family planning counselling (39.5%), implant insertion and removal (33.8%), and LAM counselling (33.1%).
Knowledge of family planning methodsMost health workers from the facilities that offered family planning (97.5%) were knowledgeable enough to counsel and provide male condoms (97.5%), DMPA-IM (92.7%), combined oral contraceptives (91.9%), and emergency contraceptives (90.9%) (Fig. 2). However, knowledge of vasectomy (2.9%), female sterilization (3.2%), IUD insertion/removal (42.4%/50.2%), natural methods SDM and moon beads, as well as that of the female condom, was limited, at 55.0%, 40.4%, and 55.6% respectively.
Fig. 2
Proportion of health workers knowledgeable enough to counsel and provide various methods (N = 261)
GuidelinesOnly 10.1% of facilities offering family planning services had all relevant SRH and family planning guidelines, and 21.8% had family planning checklists. Guidelines were more available in PNFP (40.7%) and public (31.3%) facilities than in PFP facilities (1.2%). Checklists followed a similar pattern, with the highest availability in PNFP (68.3%) and public (59.4%) facilities compared to PFP facilities (21.8%).
EquipmentLess than half (48.6%) of the facilities had a functioning blood pressure machine available on the day of data collection. The proportion was highest among clinics at 88.4%, followed by higher level facilities at 75.0%. HCIIs recorded a proportion of 55.0%, while drug shops had a proportion of 20.8%. Pharmacies had the lowest proportion of facilities with functioning blood pressure machines at 13.9%.
Contraceptive supply and stock-out resilienceMost facilities assessed had male condoms (87.5%) and combined oral contraceptive pills (79.7%) available and valid (not expired or damaged) on the day of data collection (Fig. 3). However, only 37.2% of all facilities had avoided a male condom stock-out in the past three months, and 40.0% had avoided a combined oral contraceptive stock-out. Emergency contraceptives and injectable contraceptives, DMPA-IM also demonstrated relatively high availability, at 66.5% and 69.8%, respectively, but fewer than half of the facilities (41.3% for emergency contraceptives and 35.6% for DMPA-IM) reported no stock-outs. In contrast, IUDs, female condoms, and cycle beads had the lowest availability, at 13.7%, 10.7%, and 8.5%, respectively, with similarly low resilience to stock-outs (14.3%, 18.3%, and 18.9%, respectively).
Fig. 3
Proportions of facilities with different methods available and no stock-outs in the past three months (N = 145)
Governance of family planning servicesOf the 145 facilities providing family planning services, only 24.4% had a designated focal person for SRH/family planning. Additionally, just 23.7% indicated that their family planning staff received external supervision to monitor performance, with 20.4% having received supportive supervision focused on SRH/family planning in the last three months. Furthermore, nearly half of the facilities (48.6%) did not hold formal meetings to discuss facility management.
Service provision and imposed barriers to accessing family planning methodsAmong the 261 health workers at family planning facilities, 89.9% reported providing family planning services in the past three months. When asked which methods they would never recommend under any circumstances, over a third indicated moon beads (36.4%), the SDM (32.4%), and the LAM (32.0%) (Fig. 4). Conversely, the most recommended methods were male condoms (91.5%), DMPA-IM (81.9%), DMPA-SC (76.4%), combined oral pills (79.0%), and progesterone-only pills (75.5%). Additionally, 30.6% would recommend vasectomy only if preferred by the client.
Fig. 4
Weighted proportions of providers who reported recommending different family planning methods (N = 261)
Among the providers, 97.7% imposed at least one restriction (minimum age, parity, marital status, or spousal consent) on clients seeking family planning methods. Minimum age requirements were set by 79.5% of providers, most commonly in PNFP facilities (89.6%), followed by public (80.5%) and PFP (73.9%) facilities (Table 4). Parity requirements were enforced by 59.5% of providers, with the highest at PNFP facilities (85.7%). Marital status restrictions were applied by 83.3% of providers, and 75.6% required spousal consent, with both restrictions most frequently imposed at PNFP facilities.
Table 4 Proportion of health workers imposing age, parity, marital status and spousal consent barriers and the minimum age and parity required (N = 261)The proportion of health workers imposing restrictions was lowest for condom access and highest for sterilization, except regarding marital status. The mean minimum age requirement was lowest for condoms (16.2 years, SD ± 2.1) and highest for sterilization (35.3 years, SD ± 10.1). For minimum parity, injectables had the lowest requirement (1.8 children, SD ± 1.1), while sterilization required the highest (6.1 children, SD ± 7.9).
Readiness to provide family planning servicesThe average readiness score was 46.7% (SD ± 17.0) (Fig. 5). The lowest mean scores were in the staff and guidelines domain (29.9%, SD ± 29.1%), followed by equipment (48.6%, SD ± 50.1), while the highest scores were in medicines and commodities (52.1%, SD ± 18.2). PFP facilities had the lowest mean composite score across all dimensions at 42.4% (SD ± 14.1). Public health facilities followed with a mean score of 55.3% (SD ± 20.1), and PNFP facilities had the highest mean score at 63.7% (SD ± 15.3).
Fig. 5
Readiness across public, PNFP and PFP facilities in Jinja City and Iganga Municipality
Factors associated with readinessIn the bivariate analysis, factors such as the study site, facility ownership, level of care, receipt of outside supervision to monitor performance of family planning services, holding administrative meetings, and the proportions of health workers imposing marital status and spousal consent barriers to service access at the facilities were all associated with readiness to provide family planning services (Table 5).
Table 5 Factors associated with readiness to provide family planning services (N = 144)However, after adjusting for other variables, only the level of facility, receipt of outside supervision for family planning services, holding administrative meetings, and an increase in the proportions of health workers imposing marital status and spousal consent barriers to service access remained significantly associated with readiness. Compared to higher-level facilities, HCII facilities and drug shops had significantly lower readiness to provide family planning services (β = −9.42, p = 0.036) and (β = −11.00, p = 0.022), respectively. HCIIIs, pharmacies and clinics did not differ significantly from the higher-level facilities. Receiving external supervision for family planning services was associated with a significant increase in readiness (β = 9.04, p = 0.009). Similarly, holding regular administrative meetings was positively associated with readiness (β = 9.72, p = 0.017). Regarding provider-level barriers, increase in the proportion of providers imposing marital status barriers was negatively associated with readiness (β = −9.42, p = 0.017), while imposing spousal consent requirements was positively associated (β = 6.24, p = 0.023).
Comments (0)