
Remember me
PrCa is known to have one of the highest heritability of the more common cancers at 58% [8]. The genetic predisposition to PrCa is made up of 1) common variants in the population that confer a modest impact on PrCa risk and 2) rarer monogenic variants that have a modest increase in lifetime risk of developing PrCa for individuals carrying a variant. The most well-known genes in which pathogenic variants increase risk of PrCa include BRCA2, BRCA1, MSH2, MSH6, MLH1, HOXB13, ATM, PALB2, NBN and CHEK2 [9]. Monogenic variants are identified using DNA sequencing methods, while SNPs have been identified through genome wide association studies (GWAS), and to date 451 PrCa risk-associated SNPs have been identified [10]. These PrCa risk-associated SNPs may confer lower risk individually but multiplicatively can add to up to at least 2.7-fold increased risk of PrCa for those in the top decile of PRS [11]. This may now be estimated as even higher given the more recent identification of 451 PrCa risk associated SNP [10], while the previous estimate of 2.7-fold was estimated when less than half of these had been identified.
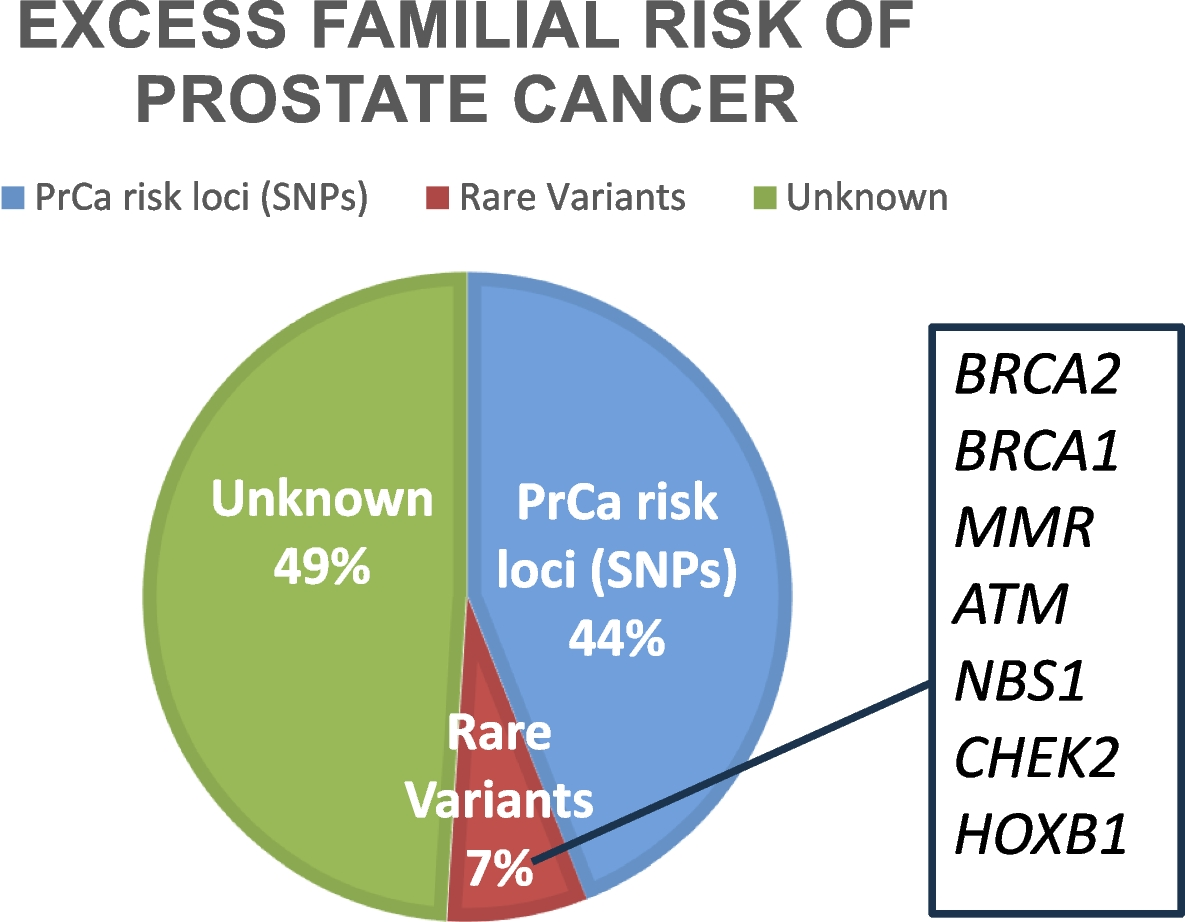
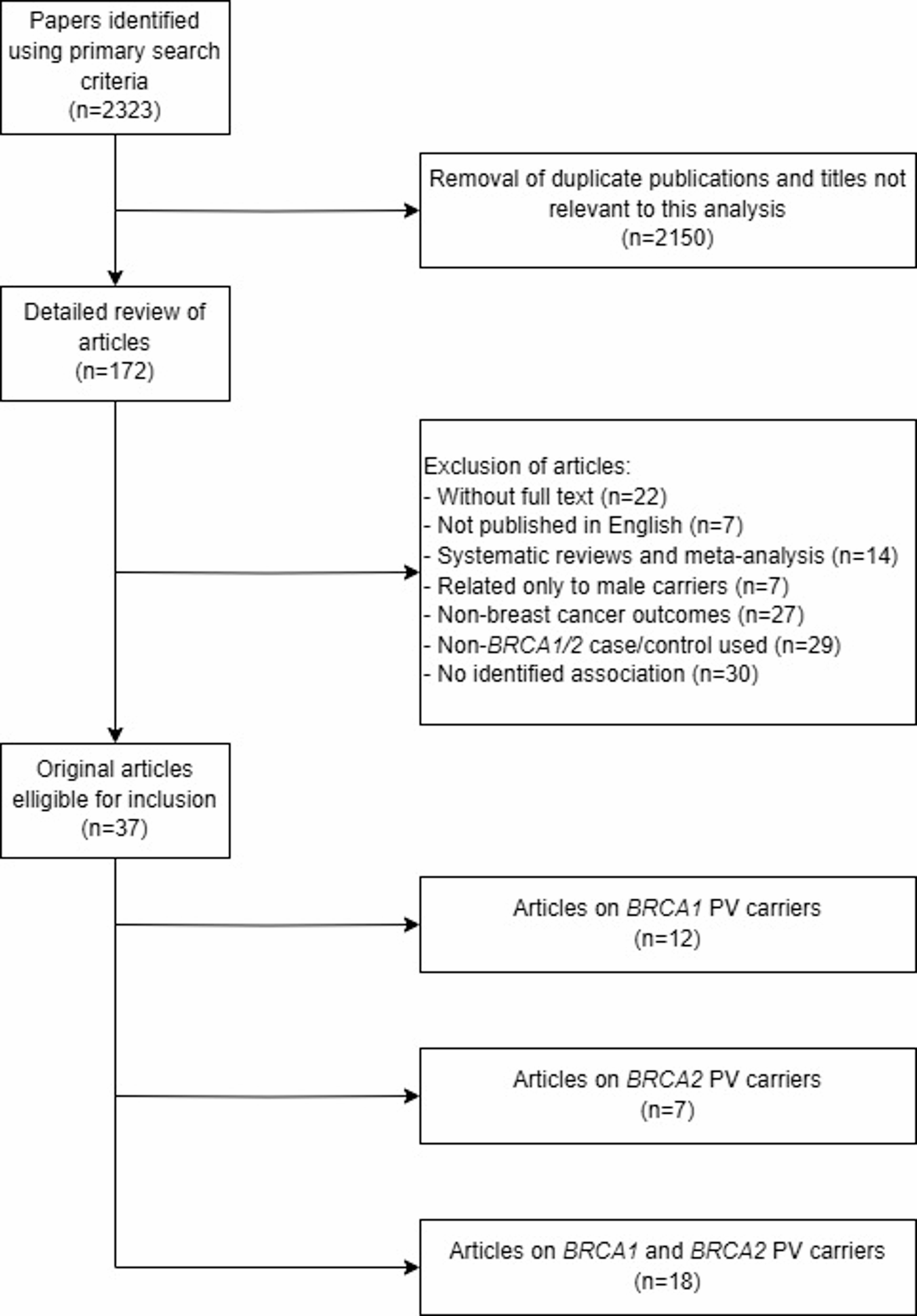
In Fig. 1 above, the excess familial risk of PrCa causes is outline with GWAS identified SNPs currently estimated to account for approximately 44%. Approximately 49% is as yet unexplained. Rare variants in certain genes associated with hereditary cancer syndromes like BRCA2 and BRCA1, MMR = mis-match repair genes such as MSH2 and MSH6 associated with Lynch Syndrome, ATM, NBS1 and CHEK2 among others and HOXB13 is PrCa specific account for approximately 7%.
Fig. 1
Excess familial risk in prostate cancer causes
The National Comprehensive Cancer Network (NCCN) guidelines recommend the following genes for germline testing currently include BRCA2, BRCA1, ATM, PALB2 and CHEK2 and mismatch repair (MMR) genes; MSH2, MSH6, MLH1, PMS2 and HOXB13 [12]. In the United Kingdom (UK) there are 8 of the above genes listed for testing on the National Genomic Testing Directory and NBN and HOXB13 are also considered PrCa predisposition genes and may be included in future clinical guidelines [13].
Germline testing is useful for: 1) diagnosis and screening potential, 2) prognosis; considering more aggressive management for variant carriers with localised PrCa and considering different targeted treatment options for those with advanced PrCa, 3) informing risk for family members; allows for cascade testing and counselling leading to personalised surveillance.
European guidelines from the European Society of Medical Oncology (ESMO) now recommend germline testing for those with PrCa [14]; echoing the USA NCCN guidelines. ESMO guidelines recommend germline testing for DNA damage repair (DDR) genes associated with cancer predisposition syndromes in patients with a family history of cancer and should be considered in all patients with metastatic prostate cancer. Tumour testing should be considered for homologous recombination genes and mismatch repair defects or microsatellite instability in patients with metastatic castrate resistant PrCa [14]. A recent ESMO update has recommended germline follow-up of tumour-only sequencing including defining the seven ‘most-actionable’ cancer susceptibility genes (BRCA1, BRCA2, PALB2, MLH1, MSH2, MSH6, RET) in which germline follow up is recommended regardless of primary cancer type [15].
Traditionally, germline testing would take place in clinical genetics units and involved two clinic visits: an initial testing and education visit and then another visit to discuss results. More recently technologies such as video/phone-based clinical counselling are routinely used to help to meet increasing demand for testing [16].
The 2019 Philadelphia Prostate Cancer Consensus Conference suggests optimal genetic consent should include: discussion of the purpose of testing and the types of possible results (pathogenic/likely pathogenic variants, benign/likely benign variants or variants or unknown significance, no variants detected), the possibility of identifying hereditary cancer syndromes or other cancer risks, the importance of cascade family testing, legal issues; and the US Genetic Information Non-discrimination Act (GINA) law [9].
Mainstream testing has been adopted as standard practice in breast, ovarian and colorectal cancer in many countries and this is now being implemented for PrCa. There is a need to streamline genetic testing as we use it more routinely and ideally make it accessible to all and feasible for oncology teams to deliver.
Comments (0)