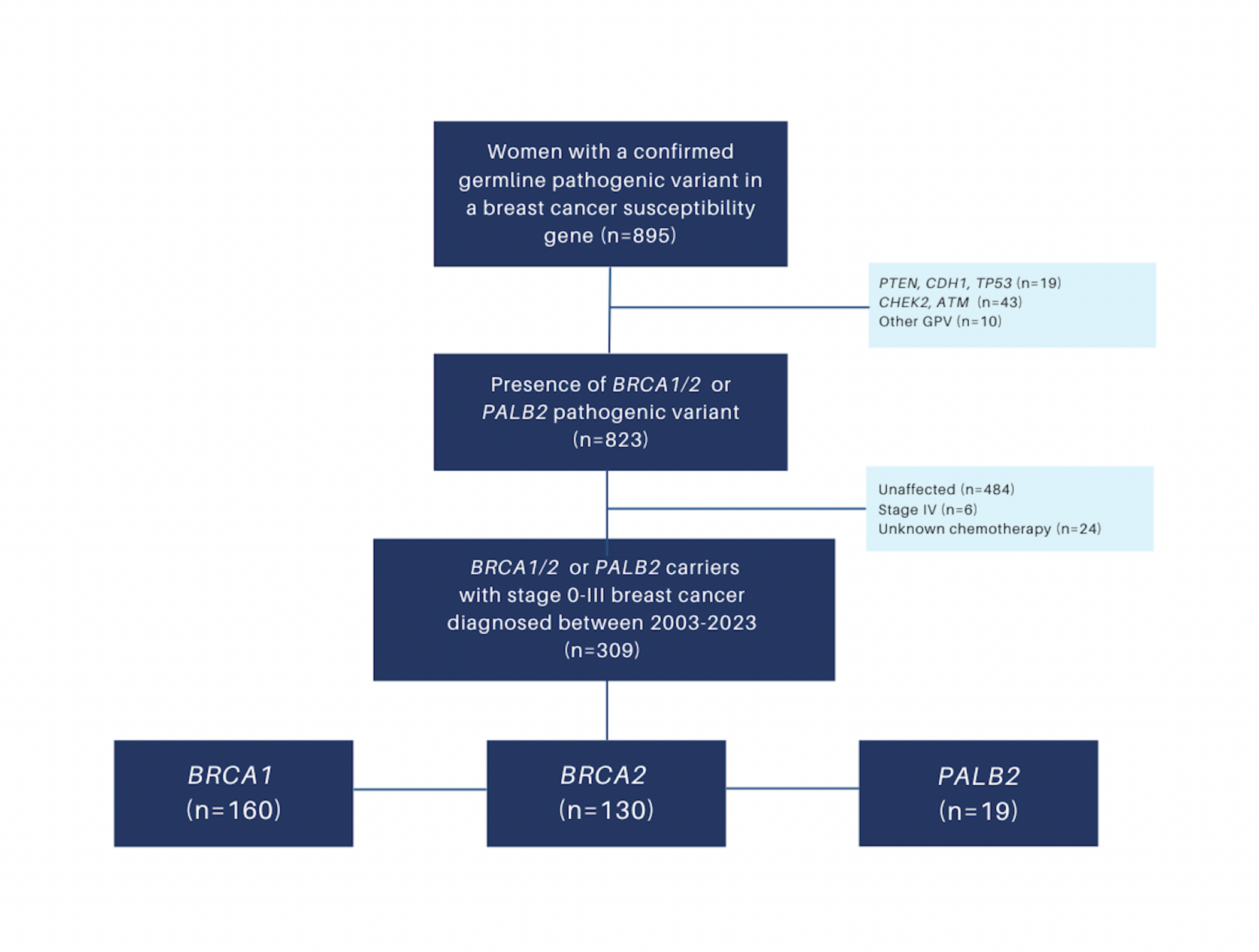
In our study of 309 affected BRCA1/2 and PALB2 carriers with operable breast cancer, the receipt of chemotherapy following an index breast cancer diagnosis was 70% overall but varied from 57% in BRCA2 carriers to upwards of 80% in BRCA1 and PALB2 carriers. In the setting of early-stage, T1N0 disease, we found that 79% of BRCA1 carriers still underwent chemotherapy, largely due to more aggressive tumor biology with TNBC.
The biologic differences between BRCA1 and BRCA2-associated breast cancers have been well established in the literature, with data on PALB2 continuing to evolve [3, 17, 18]. Germline pathogenic variants in these three genes are associated with a greater than 8-fold odds of TNBC relative to women with sporadic breast cancer [17, 19, 20], although among BRCA2 and PALB2 carriers, ER + HER2- breast cancer is still the most common biologic subtype. Data from the BRIDGES study suggest that protein truncating variants in BRCA2 and PALB2 are associated with a 17–22% and 11–13% absolute risk of developing low and high-grade ER + HER2- breast cancer, respectively, and a 7–9% lifetime risk of developing TNBC by age 80. In contrast, protein truncating variants in BRCA1 have a 22% lifetime risk of ER + HER2- breast cancer but a 40% lifetime risk of developing TNBC by age 80 [17].
Although we found that BRCA1-associated breast cancers were more likely to be early-stage and node-negative at presentation, they were also more likely to receive chemotherapy due to a higher prevalence of TNBC. Current guidelines recommend consideration of chemotherapy for triple-negative tumors greater than 5 mm and endorse its use for all TNBC beyond 1 cm (T1cN0 disease) [5, 21, 22]. The use of chemotherapy – including neoadjuvant chemotherapy– for stage I TNBC has increased over time, reflecting changes in the treatment paradigms for high-risk biologic subtypes [23, 24]. In our subgroup analysis of 89 T1N0 breast cancers, 56% of BRCA1-associated cases were TNBC compared to only 18% of BRCA2 and PALB2-associated cases. Although similar treatment patterns were seen within biologic subtypes of T1N0 disease regardless of germline pathogenic variant (85–90% of T1N0 TNBC patients received chemotherapy compared to 52–60% of ER + HER2- breast cancers), the higher prevalence of TNBC in BRCA1 carriers resulted in 80% of BRCA1 patients receiving chemotherapy for stage I breast cancer overall. Thus, unaffected BRCA1 patients who undergo high-risk screening with the goal of early detection should be counselled around the high likelihood of requiring chemotherapy if diagnosed with a breast cancer, even if detected at early stages.
As has been shown in other studies [11, 25, 26], we found that pre-diagnostic awareness of a germline pathogenic variant in BRCA1/2 and PALB2 was associated with a stage-shift towards smaller, node-negative tumors at diagnosis, with a significantly lower proportion receiving chemotherapy (60% vs. 74%) and endocrine therapy (22.2% vs. 36.7%) relative to those undergoing genetic testing after a diagnosis of breast cancer. In a recent study by Hadar et al. that included 105 BRCA1/2 germline pathogenic variant carriers diagnosed with breast cancer, pre-diagnostic awareness of their BRCA1/2 status was similarly associated with earlier detection with higher rates of stage 0-I disease (86% vs. 39%, p < 0.001) as well as lower rates of chemotherapy receipt (29% vs. 79%, p < 0.001) [11]. In another study by Bernstein-Molho et al. of 225 Israeli BRCA1/2 carriers, chemotherapy was recommended in 51% of known carriers with pre-diagnostic awareness compared to 80% of latent carriers who underwent genetic testing during oncological treatment or follow up (p < 0.001) [25]. The method of breast cancer detection was also dramatically different between these two groups, with 58% of known carriers having breast cancer diagnosed by MRI screening, compared to the majority (65%) of latent carriers presenting with a self-detected palpable mass, the latter of which was more likely to be node-positive (48.5% vs. 11.5%, p < 0.001). Results from our study show similar patterns of detection, with 61% of known carriers presenting with an MRI-detected abnormality compared to those without awareness of their germline pathogenic variant, of which 70% presented with a clinical abnormality, typically in the form of a palpable mass. It is also notable that no patients with pre-diagnostic awareness in our study presented with stage IV disease. Recent data from the Hereditary Breast Cancer Clinical Study Group support a survival benefit of MRI in unaffected BRCA1/2 carriers partaking in MRI surveillance programs [2]. In their study of 1756 women, Lubinski et al. found that the risk of breast cancer mortality at 20 years was 3.2% for those undergoing MRI surveillance compared to 14.9% for those who did not. Notably, this appeared to be driven largely by an 80% reduction in breast cancer related deaths in BRCA1 carriers, whereas there was no statistically significant effect of MRI on reducing mortality in those with BRCA2 pathogenic variants.
In addition to enabling enhanced surveillance and access to preventive strategies, early awareness of a germline pathogenic variant in BRCA1/2 or PALB2 vastly influences surgical decision making when a patient is diagnosed with breast cancer. In the current study, 72 (23.3%) of patients underwent genetic testing prior to their breast cancer diagnosis, whereas 105 (34.0%) had testing and result disclosure after diagnosis but before index breast surgery, and the remaining 132 (42.7%) underwent testing and/or result disclosure after index surgery. The high proportion of patients who were unaware of their germline pathogenic variant at the time of surgery likely contributed to the high breast conserving surgery rate of 48.4%, as those lacking knowledge of their genetics status had a 76% rate of breast conservation compared to only 28.6% in those aware of their carrier status. By contrast, women in our study who were aware of their BRCA1/2 or PALB2-positive status prior to diagnosis underwent bilateral mastectomy as their index breast surgery in 56% of cases.
Similar to other studies [27, 28], we have previously shown that preoperative result disclosure increases uptake of bilateral mastectomy by 70% and reduces the need for adjuvant radiation in a large percentage of carriers who forgo breast conserving treatment for therapeutic mastectomy [29]. Several guidelines currently support consideration of unilateral therapeutic and contralateral risk reducing mastectomy as a treatment option for affected BRCA1/2 and PALB2 carriers, although breast conserving therapy remains reasonable for eligible patients who desire this approach [30,31,32]. As mainstream genetic testing efforts that streamline result disclosure are more widely implemented, better informed local therapy decisions are expected to be cost-effective and will increase the opportunity for surgical prevention [33,34,35].
Data on treatment and chemotherapy receipt in PALB2 carriers who develop breast cancer remains sparse, in large part because of the more recent discovery and characterization of PALB2 as a breast cancer susceptibility gene and the relative rarity of pathogenic variants in PALB2 - seen in only 0.2–0.5% of invasive breast cancers [19, 36] - compared to BRCA1/2 [4, 14, 37]. Single-institution series from the United States suggest bilateral mastectomy uptake is approximately 60% in PALB2 carriers [38], while studies from population-based data that combine PALB2 with other non-BRCA carriers such as those with moderate penetrance variants in ATM and CHEK2 report expectedly lower bilateral mastectomy rates of 43% [39]. In our study, PALB2 was associated with a 37% likelihood of bilateral mastectomy at index breast cancer surgery, but this did not account for women undergoing risk reducing surgery during follow-up. The available literature also suggests that PALB2-associated breast cancers are biologically aggressive, with TNBC diagnosed in approximately one third of breast cancer cases [4, 37]. In the remaining PALB2 affected carriers with HR + HER2- breast cancer, higher 21-gene recurrence scores (similar to that of BRCA2 carriers) have been reported, suggesting that tumor biology and chemotherapy response is likely similar between these groups [6]. In our study, PALB2 carriers were more likely to require chemotherapy relative to BRCA2 carriers, however analyses were based on a small number of only 19 PALB2-cases and were likely underpowered; therefore, further data on this subgroup are needed.
Our study has several additional limitations related to its retrospective cohort design and prolonged period of study between 2002 and 2022, during which indications for chemotherapy were changing. Furthermore, we lacked information on the rationale for chemotherapy decisions by treating oncologists, and as stated above, the PALB2 subgroup was limited. For the patients with pre-diagnostic awareness, we did not collect information on long-term adherence to high-risk MRI screening, nor did we have information on participation and adherence to provincial mammographic screening programs, which begin at 50 years old in Canada, for those with post-diagnostic awareness. Despite the stated limitations, our study is one of the first to evaluate PALB2 germline pathogenic variant carriers and to our knowledge is one of the largest in the reported literature to address the topic of chemotherapy receipt in those with pre-diagnostic awareness of their germline pathogenic variant status.
Our results suggest a 55–80% likelihood of receiving chemotherapy for BRCA1/2 breast cancer and provide early estimates for patients with PALB2-associated disease. Furthermore, while these data support the value of pre-diagnostic awareness and high-risk screening to detect cancers early and reduce the need for chemotherapy, they also suggest that BRCA1/2 and PALB2 carriers should be counseled around the greater than 60% likelihood of requiring chemotherapy even if diagnosed with early-stage disease. Decision tools and counseling that extend beyond survival outcomes and incorporate estimates around the need for chemotherapy will remain important for unaffected carriers considering preventive options in the future. Additional studies that evaluate the interaction between premenopausal risk reducing salpingo-oophorectomy, hormone-replacement therapy, and endocrine prevention on subsequent breast cancer development, tumor biology, and chemotherapy receipt would also be valuable for women considering risk-management strategies.

Comments (0)