
Remember me
Evidence-informed policymaking emphasizes that policy decisions should be informed by the best available evidence on effectiveness, equity, feasibility of implementation, affordability, sustainability, and acceptability to stakeholders within the specific context that the policy is to be applied [1, 2]. It is widely accepted that policies informed by research evidence will be more effective than those that are not, make more effective use of scarce resources, have more legitimacy, and ensure transparency and accountability in decision-making [1,2,3]. Ideally, evidence-informed policymaking follows a systematic and transparent approach across all aspects of the decision-making process. In reality this is not always the case, and perhaps it is too much of an ‘ask’ to expect that it be so at all times. Policy that is developed under situations where fast decisions need to be made, where there is a perception of low quality or scarce evidence, or when conflicts of interest are involved, can ‘test’ and work against the concept of evidence-informed policy. However, better use of research evidence and transparency may not need to be sacrificed if a framework to guide policy makers under ‘realistic’ policymaking conditions is used.
During the COVID-19 pandemic considerable attention was given to the importance of transparent decision-making that is informed by evidence. Much was written about the decisions that were made and the consideration (or not) of research evidence [4,5,6]. The WHO and many national governments have conducted reviews of what went well and what could have been done better [7, 8]. Recommendations include calls for greater transparency in decision-making to gain public trust, especially when there is limited research evidence, to publicly release the modeling and evidence used in government decision-making [8], and the use of evidence-based strategies [7] at both national and global levels. This has had implications for governments. In some instances, governments have successfully had legal proceedings brought against them for not acting on the evidence and taking timely action to prevent deaths [9]. Alongside this there are international calls for action to make use of the increased focus on evidence to strengthen the evidence-informed policymaking system [2, 10, 11]. According to the Global Commission on Evidence to Address Societal Challenges, “COVID-19 has created a once-in-a-generation focus on evidence among governments, businesses and non-governmental organizations, many types of professionals, and citizens” [10].
We can learn from existing practices of transparent, evidence-informed decision-making in health. These include systems for the development and implementation of guidelines [12,13,14], health technology assessments [15, 16], and essential medicines lists [17, 18] to guide health care and public health policy. These processes combine clear criteria for decision-making with a transparent, deliberative process for making recommendations and/or decisions [19]. Similar processes and criteria can also be used for coverage decisions, priority-setting, and health benefit package design, though there is not a widely used set of criteria or established process for these [20,21,22,23,24]. Thus, they are not explicitly included in this analysis. In the case of health policymaking outside of clinical practice and medical technology, however, more work needs to be done to institutionalize the use of evidence in a transparent, deliberative process. This is exemplified in WHO’s Evidence-Informed Policy Network Call to Action to accelerate the institutionalization of evidence-informed decision-making, including through the use of high-quality norms, standards and tools [25, 26], and related work to make the use of evidence in policymaking routine [27].
Guidance for evidence-informed policymaking that is systematic and fosters transparency need to factor in the political processes (institutions) and external stakeholders (interests) that play a role in the success or failure of a policy intervention, even when supported by high-quality research evidence [28,29,30,31]. Powerful interest groups can and do influence policy by implementing a range of strategies to obfuscate or undermine the evidence used to inform policy, see for example Gómez 2019 [32] and Gilmore et al. 2023 [33]. To respond to, and counteract this, Reich advocates for the use of political economy analysis, alongside the technical analysis, to assess the political landscape, including mapping the key stakeholders and estimating the feasibility of policy change [34]. He argues that this analysis can help the health sector to improve the effectiveness of its policy process, and to give them ideas and strategies on how to shape health policies and the policy process [34, 35]. Likewise, Walt and colleagues argue for the use of health policy analysis to understand the actors, processes and context in which policy is made, in addition to the policy content [36]. They suggest that health policy analysis can be used prospectively (as well as retrospectively) to understand and influence policy outcomes [36,37,38]. Gómez, another key scholar in this field, notes that politics is an indispensable part of global health policy discussions; and that the just allocation of health resources requires democratic deliberation [39].
In this paper we propose an integrated framework to guide evidence-informed policymaking that builds on existing evidence-to-decision frameworks [14, 15, 18, 19, 40], but includes a more explicit consideration of the political factors that influence policymaking [28,29,30,31]. It does so by integrating the political and deliberative process factors into existing, widely used evidence-to-decision frameworks, rather than treating the political and technical factors separately.
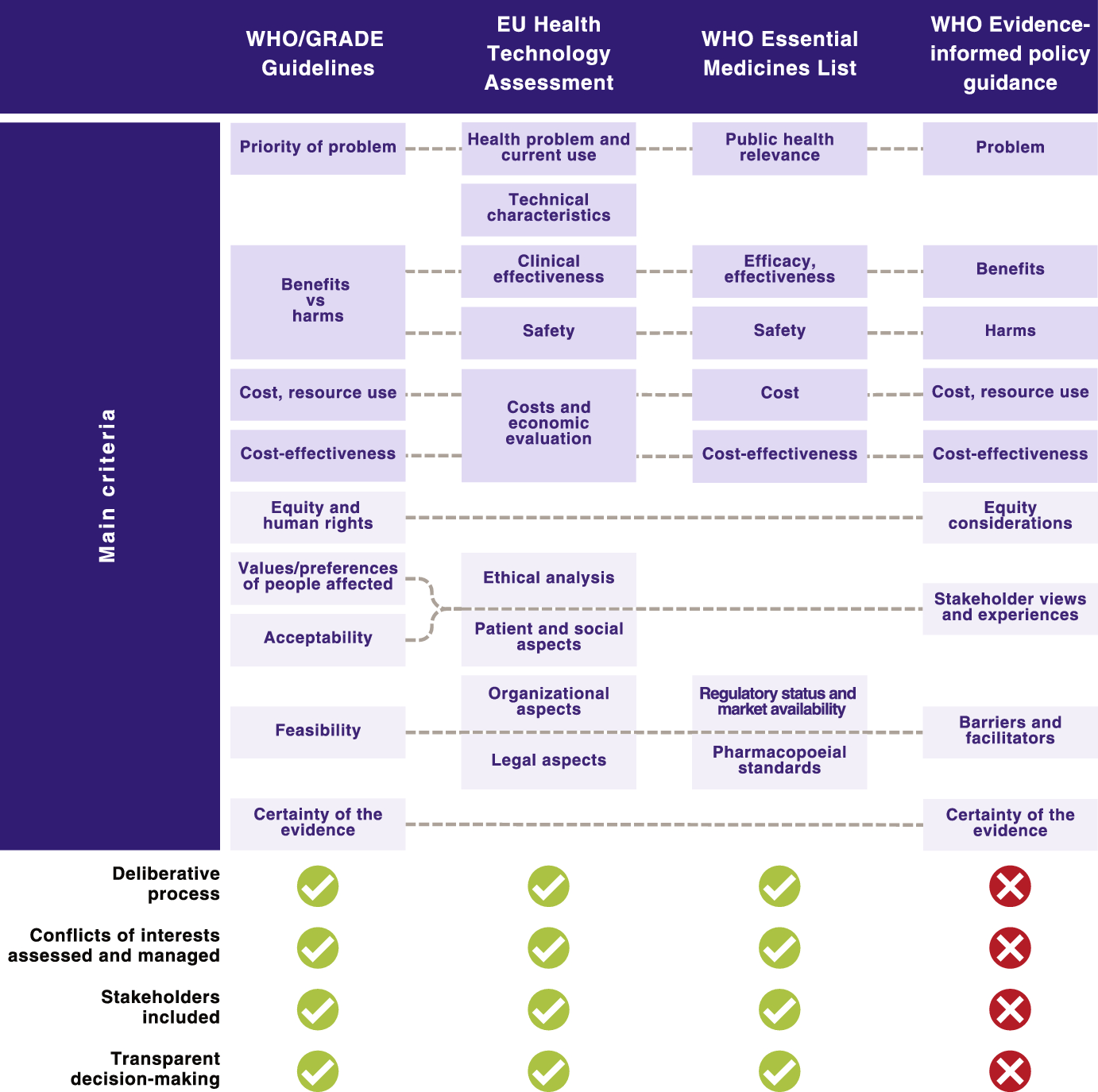
Frameworks for evidence-informed decision-makingA selection of existing frameworks that support evidence-informed decision-making for the development of guidelines, health technology assessment (HTA), and the compilation of essential medicine lists (EML) are shown in Fig. 1. This selection was informed by reviews of existing evidence-to-decision frameworks [41,42,43], an international survey of decision-makers [44], and literature on the use of deliberative processes for decision-making [16, 20, 45,46,47,48]. We selected frameworks that are endorsed by the World Health Organization for use by Member Countries [13, 14, 17, 18] due to their likely widespread global use, including in low- and middle-income countries. In the case of HTA, the WHO does not endorse a specific framework or decision criteria apart from cost-effectiveness, though it does offer guidance on the institutionalization of HTA mechanisms [49]. Thus, for HTA we have included the HTA Core Model that has been adopted by the European Union for joint assessments by its Member States [15, 50, 51] due to its wide coverage. In the case of evidence-informed policymaking, there is not a widely used or endorsed framework or process for decision-making. However, the WHO does offer guidance for preparing evidence briefs for policy and for organizing policy dialogues [52, 53], which are aimed at informing the policymaking process—these are included in Fig. 1. The figure includes the main criteria recommended for decision-making, and also indicates some key elements of the decision-making process that would promote a more balanced, non-biased assessment of the evidence and decision-making criteria. These elements include whether a deliberative process is used for decision-making, there is a clear process for assessment and management of potential conflicts of interest, stakeholders are included, and whether there is transparency in the decision-making process. Here, transparency refers to the publishing of the criteria used, stakeholders involved, and outcome of the decision-making process.
Fig. 1
Evidence-informed decision-making frameworks and processes. The guiding manuals and articles for each of the frameworks are: WHO/GRADE Guidelines the WHO Guideline Handbook and GRADE articles [13, 14, 19, 40]; EU Health Technology Assessment The HTA Core Model® [15, 50, 51]; WHO Essential Medicines List—WHO regulations and manuals [17, 18, 54]; and WHO Evidence-informed policy guidance WHO evidence briefs for policy guiding manual [53]. EU European Union; GRADE Grading of Recommendations Assessment, Development and Evaluation; WHO World Health Organization
The criteria for decision-making that are common between all four frameworks include the priority of the health problem (magnitude or burden, causes), the balance of health benefits (efficacy, effectiveness) and harms/safety, cost/resource use, and cost-effectiveness (Fig. 1). Other criteria that are used in two or more of the four processes include equity considerations, certainty of the evidence, acceptability to stakeholders, and feasibility. In the case of acceptability, the key stakeholders can include the public (patients or population affected), government, deliverers of the intervention, industry, and civil society organizations, depending on the policy option or intervention being assessed. The acceptability of an option overlaps with the values/preferences of people affected, ethical analysis, patient and social aspects, and stakeholder views and experiences, as shown by the dashed lines in the figure. Further, different stakeholders may implicitly consider criteria, such as equity and feasibility, when deciding whether an option is acceptable to them. Feasibility overlaps with resource considerations, and organizational aspects, e.g., existing infrastructures, legal aspects, regulatory status and market availability and availability of pharmacopoeial standards in the case of medicines, among others [14, 15, 18, 51]. All four frameworks and processes shown in Fig. 1 use systematic reviews of primary studies as an important source of research evidence to address the main criteria.
The use of deliberative processes, involving key stakeholders, to consider and weigh the different criteria when making recommendations or decisions about options is an essential part of the WHO/GRADE guidelines development process [13, 14]. Deliberative processes are also used in WHO EML decisions [18]and for HTA [49, 50]. Here, deliberation refers to a discussion that involves the careful and serious weighing of reasons for and against the options [55], and allows “individuals with different backgrounds, interests and values to listen, understand, potentially persuade and ultimately come to more reasoned, informed and public-spirited decisions” [56]. The use of deliberative processes gives legitimacy to the decisions made and their acceptability to stakeholders, especially if they are seen as fair, and are also transparent, allowing accountability [20, 57]. In the case of WHO/GRADE guidelines, EU HTAs, and WHO EML, it is normal practice to publish details of the process, the stakeholders involved, the evidence used, and the criteria assessed [14, 18, 50, 58, 59], though the implementation of this within countries may vary. In the case of the WHO EML, however, some authors have noted that there may be room for improvement in the quality and transparency of the process and for selection of stakeholders [60,61,62]. In the case of HTA, transparency in decision-making is also recommended by the WHO for countries working towards institutionalization of HTA mechanisms [
Comments (0)