
Remember me


The data used in this study were obtained from a web-based cross-sectional study conducted in China between March and June 2024. All participants were recruited from the ‘Beijing Aili Myasthenia Gravis Care Centre’. This is one of the largest MG associations in China. Interested members were contacted and requested to participate in a specific online ‘survey group’. The researchers informed the participants about the study’s objectives and provided guidelines for completing the online questionnaire. The study protocol was approved by the Human Research Ethics Committee of the Hong Kong Polytechnic University (ref. no.: HSEARS20240226001), and informed consent was obtained from all participants.
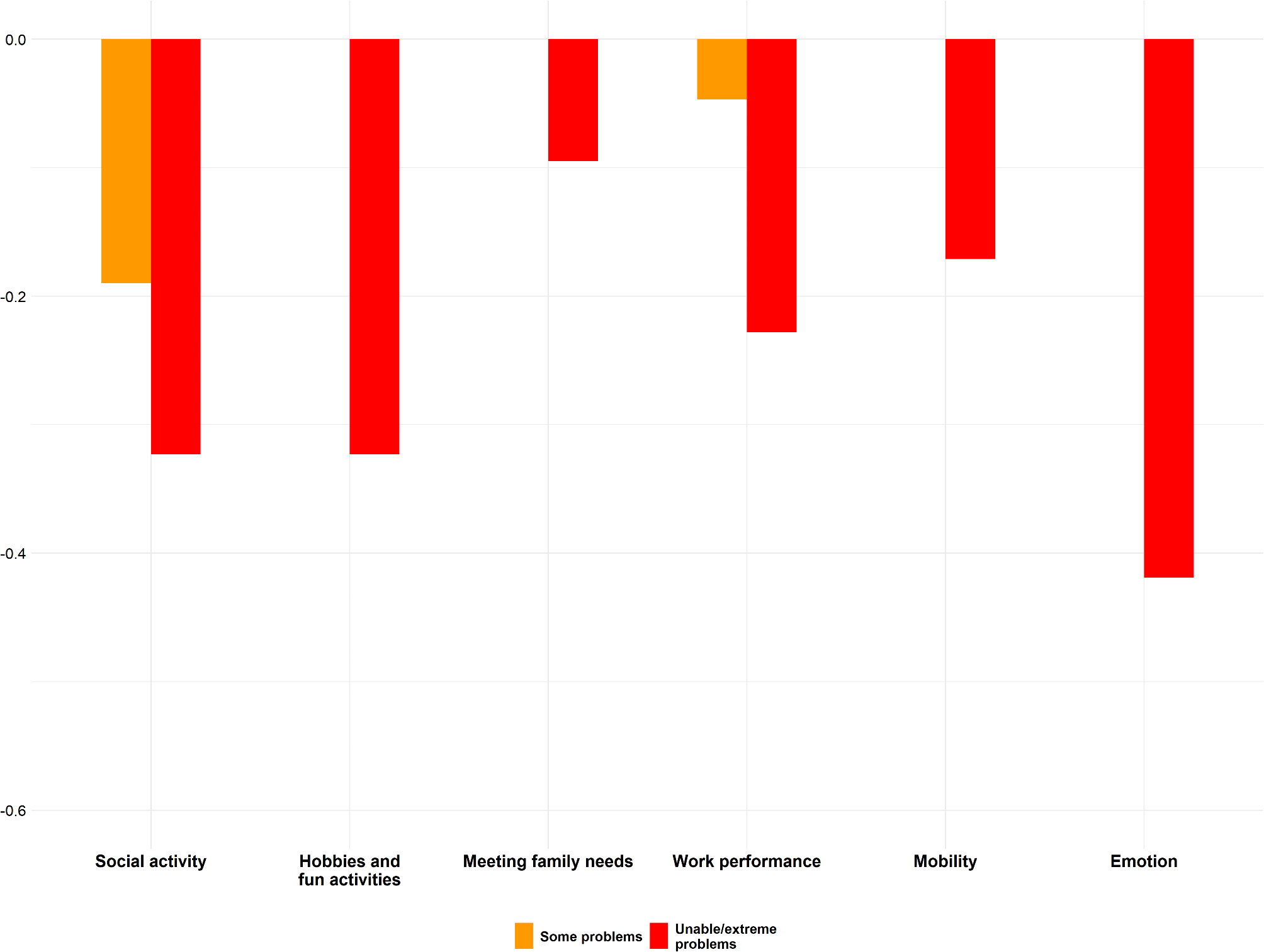
MeasuresMGQoL-6DThe MGQoL-6D descriptive system was derived from MGQoL-15r. It comprises six items: social activities, hobbies and fun activities, work performance, meeting family needs, mobility, and emotion. Each item can be answered using a three-level scale ranging from 1 (no problem) to 3 (unable/extreme problem). Consequently, the MGQoL-6D descriptive system represents 36 possible health statuses. It has demonstrated good psychometric properties in the Chinese MG population, as evaluated using both the classical test theory and item response theory methods [4].
Profile selection for the discrete choice experiment (DCE) surveyThe DCE combined with Time Trade-Off (DCE-TTO) method is a widely used approach to estimate preference weights for preference-based measures [6,7,8,9], like the MGQoL-6D because it effectively captures how individuals value different health states by integrating both choice-based and time-based valuation techniques. In a DCE, respondents are presented with hypothetical scenarios comparing pairs of health states defined by specific attributes, and they choose their preferred option, revealing relative preferences indirectly. The TTO component complements this by asking respondents to indicate how many years of life they would trade off to avoid a particular health state, providing a direct measure of utility anchored to a 0–1 scale (where 0 is equivalent to death and 1 is full health). This hybrid DCE-TTO method balances the cognitive simplicity and statistical efficiency of DCE with the precision of TTO in eliciting health state utilities.
The MGQoL-6D comprises six items with three response levels. We included a duration attribute to allow estimation of the trade-off between life expectancy and quality of life, which is intrinsic to the estimation of QALYs. When combined with the duration item (5, 10, 15, and 20 years), which was selected to be plausible for most respondents with sufficient spread to ensure discrimination between them, it resulted in over 2900 caring profiles (36 × 4 = 2916). The durations were selected based on a literature review and consultations with patient associations and clinical experts, balancing the need to reflect realistic life expectancy impacts for MG patients in China with survey manageability. MG, a chronic condition with fluctuating severity, imposes long-term HRQoL challenges despite modern treatments preserving near-normal lifespan. These 5-year increments align with standard health state valuation practices (e.g., QLU-C10D), offering plausible horizons for respondents to assess health state trade-offs while supporting statistical modelling. Considering it is not feasible to include all possible combinations of profiles in a valuation survey, we used the D-optimality criterion, as recommended by International Society for Pharmacoeconomics and Outcomes Research, to determine the optimal experimental design for this study. This criterion aims to maximise the determinants of the information matrix for parameter estimation. Each item’s response level was treated as a categorical variable, whereas the duration item was treated as a continuous variable.
A designed experiment was used to select 40 choice sets within four blocks to maximise statistical efficiency for estimating the main effects from the DCE data to estimate the MQGoL-6D utility weights. In the valuation survey, each participant was presented with 10 choice sets and asked to indicate their preference between two different MGQoL-6D health states (Situations A and B). Each was described by the 10 MGQoL-6D domains, with an additional attribute of survival duration. To reduce the cognitive burden of the choice task, each choice set included only four differing attributes (four of the six HRQoL attributes and duration), which were highlighted in yellow. The remaining three unhighlighted attributes were held constant, as illustrated in Fig. 1. The levels of the changing attributes were selected using a balanced incomplete block design, and a generator-based approach was used to determine how these four dimensions differed between options A and B. The levels of the attributes that were constant were selected using an orthogonal main-effects plan. The order in which participants observed the MGQoL-6D attributes in the DCE survey was randomised across participants; however, the order was maintained for each participant when completing all 10 choice sets. A pilot test was conducted with 10 patients with MG to confirm the feasibility and acceptability of this design before the formal valuation survey.
Fig. 1
Utility decrements for the MGQoL-6D
DCE surveyThe survey began with an information sheet, and informed consent was obtained before commencing the study. The survey consisted of five stages: First, respondents provided information about their socio-demographics, health, and HRQoL (EQ-5D-5 L). They also completed the MGQoL-6D classification system to familiarise themselves with the health state profiles used in the survey. Second, participants watched a video that explained DCE, its purpose, and how to answer its questions. Third, respondents completed a DCE question that included a dominated choice set, where Option A described a clearly better health status than Option B. Only data from those who answered this question correctly were included in the final analysis. Fourth, participants answered one block of 10 DCE questions. Finally, respondents answered four questions about the difficulty of understanding and completing the DCE tasks.
Data analysisA descriptive analysis was used to describe the participants’ sociodemographic characteristics and HRQoL. DCE data were analysed using a conditional fixed-effects logit model (CLM). To calculate the preference weights, the utility of option j (health status A or B) in choice set s for respondent i is described by the following formula:
Uisj = αTIMEisj + βXisj'TIMEisj + εisj,
i = 1,…, I respondents; j = options A and B; s = 1,…, 40 choice sets.
where TIMEisj represents the survival time in option j, and the coefficient α denotes the utility associated with a life year. X′isj is a vector of dummy variables representing the levels of MGQOL-6D health status described in each health state option j in a choice set, with β being the corresponding vector of coefficients associated with each level in each dimension within X′isj for each life year. The error term εisj is assumed to follow a Gumbel distribution. Preference weights on the full health-dead 1 to 0 scale were generated using the marginal rate of substitution. The coefficient for each severity level of each item was divided by the duration coefficient (the ratio of β to α), which reflects the trade-offs between quality and quantity of life. Health-state utilities were generated by summing 1 and the relevant (negative) utility weights. All data analyses were conducted using STATA version 15 (StataCorp LP, Texas, USA).
Comments (0)