This analysis is based on the first five years of implementation of a nutrition initiative with a focus on infant and young child feeding to save lives, prevent illnesses, and contribute to healthy growth and development in LMICs from 2009 to 2014. The information provided in this article is intended to support the planning and implementation of improved large-scale child nutrition programs, specifically for complementary feeding during 6 to 23.9 months of age. Bangladesh, Ethiopia, and Vietnam were selected for their large populations and different contexts. The costs represent expenditures on additional activities layered onto existing services to generate impacts on nutrition practices. The cost to participants is not included. Therefore, these costs are incremental expenditures incurred to enable/facilitate significant improvements in existing programs. In collaboration with national authorities and as noted in country policies and strategies, six CF practices were prioritized in all programs: timely introduction of foods at 6 months; dietary diversification through the use of four or more specified nutrient-rich foods daily; meal frequency of 2–3 times a day at 6–8 months and 3–4 times a day at 9 months or older; discouraging unhealthy foods; continued feeding and fluids during illness and increased feeding after illness; and breastfeeding through two years of age [38, 39]. In this analysis we focus on dietary diversity combined with recommended meal frequency as a single indicator for assessing adequate diets of young children [7].
For costs, we used a top-down, gross costing method based on actual expenditures incurred in each county program to estimate the incremental financial costs of the three large-scale CF programs in US dollars ($). The costs represent a payer perspective and include expenditures incurred for CF over and above existing activities and personnel already working in program areas. We extracted data on financial expenditures from records maintained by each country-specific program’s accounting database. The methodology is an accounting of financial expenditures rather than an economic analysis of costs [40]. We compared the total costs, average total costs per year, costs of program components, and cost per participant in CF programs implemented in each country. The data sources for costing were similar across the countries and involved researching expenditure records from a standardized accounting system maintained by the overall initiative. Standardization was maintained in the countries’ accounting records for categorizing expenditures on CF programs and allowed us to make cross-country comparisons of total and program component costs. Details on the programs are provided in Additional File 1.
Calculating incremental financial costs
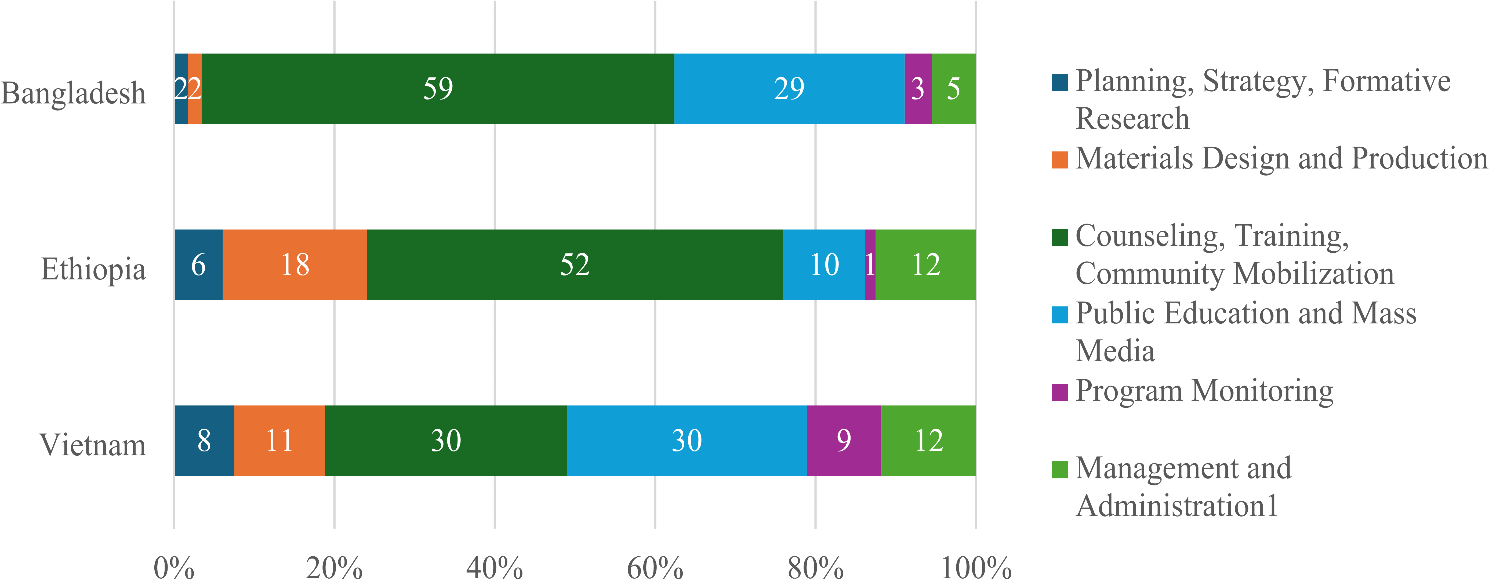
We extracted data on payments made to field implementing agencies for various tasks such as formative studies and assessments used for developing and planning activities; designing, printing, and disseminating tools and materials; building the capacity of frontline workers; providing supervision and monitoring; conducting community events; and public education and mass media design and dissemination. We entered information on invoices paid to implementing partners into our accounting database. All expenditures were converted by accounting managers to $ using the prevailing exchange rates. Conversion into 2022 $ was done using the Consumer Price Index ratio of the year of expenditure to the Consumer Price Index in 2022 using data obtained from the World Bank World Development Indicators available online at https://data.worldbank.org/products/wdi. We aggregated the cost components to calculate the total incremental costs of each country’s program. Program reports provided the total program durations, and the total costs incurred over the life of each country program were divided by the number of project years to calculate the average annual costs per year. We calculated costs per program component per country, across the three countries.
Calculating the number of participants
The number of participants consists of the number of mothers and children 6-23.9 months of age who were reached by the two main categories of interventions interpersonal communication (IPC) or counseling and public education and mass media (PE/MM). Participants were calculated from program coverage results and population figures.
We use three measures of participants as the denominator for estimating coverage: (1) number of mothers and children 6 to 23.9.9 months of age residing in areas of intensified implementation (where the evaluations were conducted), other areas where the same model of IPC was adapted and implemented, and areas reached through PE/MM; (2) all individuals reached that were needed to produce an impact consisting of mothers and children 6 to 23.9 months of age based on coverage evaluation surveys and influential individuals, including family and community members, peers and health personnel; and (3) number of children 6 to 23.9 months of age in IPC areas with improved CF practices as measured through evaluations using minimally adequate diet (MAD) as the indicator (WHO 2008).
Number of mothers and children reached
Program records, monitoring data and impact evaluation results provided coverage percentages for each country. For exposure to public education/media, we used the percentage of mothers who recalled seeing or hearing messages on CF from any public education or media channel. For IPC, we measured the percentage of mothers who recalled being counselled or attending community groups/events where CF was discussed face-to-face with mothers. Data sources for calculating participants reached by country are shown in Additional File 2. The numbers of mothers and children under two years were those residing in program areas from program monitoring data, 2012–2014 national and regional population data, and World Bank population databases, accessed at https://data.worldbank.org/indicator/SP.POP.TOTL. Coverage was determined by cluster-randomized surveys conducted by external agencies in representative samples of program areas using standardized methods across the three countries. The coverage in scaled up or expansion areas was calculated by using control-arm coverage for public education/mass media, media monitoring reports from advertising agencies involved in implementation, process evaluation studies of service delivery, descriptions of expansion models, and monitoring and supervision data combined with implementation records.
For Bangladesh, data from household census of mothers and children collected by national health services combined with program coverage from evaluation surveys showed that 1.7 million mothers of children < 2 years were reached in 50 upazilas over 2 years [41], with a coverage of 92% for IPC, 73% for PE/MM (coverage measured in program areas), and 67% PE/MM coverage measured in control or non-IPC program areas [10]; 74% is the 20% discounted IPC coverage in scaled up areas based on comparing details of the intensive and scaled-up program implementation models [42].
For Ethiopia, data from household census of mothers and children collected by national health services combined with program coverage from evaluation surveys showed that 1.5 million mothers of children < 2 years were reached in 295 woredas over 2 years [41, 43]. About 38% of mothers were measured through cluster-randomized evaluation surveys as having received IPC, with 30% coverage of PE/MM found through evaluation surveys in 89 intensive areas [9]; a lower coverage reduced by 40% is used to calculate coverage in low-intensity expansion areas based on a process evaluation study showing lower fidelity to the program model in expansion areas [44].
For Vietnam, data from household census of mothers and children collected by national health services combined with program coverage from evaluation surveys showed that 2.3 million mothers of children < 2 years were reached nationally over 3 years [45]. The catchment area population of CHCs where the intervention was located provided the numerator; for the denominator we used 42% coverage measured through cluster-randomized evaluation surveys for IPC. About 36% PE/MM coverage was measured through cluster-randomized evaluation surveys in intense areas, with 31% PE/MM coverage in low intensity areas [11]. Additionally, 30,000 mothers and children 6-23.9 months were reached through community support groups for IPC [46] with coverage of 50% according to program records.
Number of influential persons reached
Special efforts were made in IPC areas to engage community thought leaders such as local ‘doctors’, priests, imams, fathers, elder women, food sellers, and members of women’s networks. We included five potential influential groups, and information used for specifying and calculating those engaged in the respective programs is shown below. In all country programs, the number of health personnel trained in CF and equipped with tools was included; family members in areas reached with IPC and/or PE/MM were included. Data sources for calculating influentials reached by country are shown in Additional File 2. In all countries, formative studies conducted for program design and baseline surveys identified categories of influential persons who needed to be reached. Monitoring data and information from program implementation and supervision reports provided the basis for calculating influentials reached through program interventions such as training, community forums, home visits, and mass media. Endline evaluation surveys measured improvements among some groups, e.g., knowledge and activities of health workers, and community and family members.
Bangladesh
In Bangladesh, 75,000 health personnel were trained according to training lists; they were drawn from government health services, private clinics and NGO agencies, validated through observation visits, spot checks, surveys and receipts of training per diems paid, and training materials distributed. Evaluation surveys showed that in addition to three cadres of BRAC workers who delivered IYCF services, there were trained allopathic doctors, trained traditional birth assistants, government health workers, and traditional village doctors in each community who influenced practices and were reached by the program through orientation and training, community forums, and mass media.
Family members were calculated based on survey results on household characteristics and mothers’ responses to from whom they seek guidance; we used a ratio of 1 family member per mother-child dyad that was reached by any intervention (1 dyad = 1/2 of mothers and children) to calculate numbers. Formative research and baseline survey showed that mothers sought help for CF problems from respondents’ mothers/mothers in law, and family members; subsequently BRAC and other NGOs and government workers held community forums for female family members and women who were pregnant and mothers of young children and engaged them during home visits; additionally, mass media was targeted to male family members and female members of the family were exposed to mass media.
Community leaders were calculated based on monitoring data on community events and mothers’ responses to from whom they seek guidance; we use a ratio of 1/500 dyads reached by any intervention. Formative research and the baseline survey showed that mothers sought help for CF problems from doctors (including the village doctor); community inventions included BRAC and other NGOs conducting community forums and a special newspaper and radio campaign implemented by commercial advertising agencies that was targeted to private and local doctors to raise awareness and fill knowledge gaps on evidence-based IYCF practices and problem-solving.
Religious leaders were based on program design and monitoring records for community events using a ratio of 1 per 500 mother-child dyads reached by any intervention. To build on Koranic teachings that support IYCF, special IYCF materials and sessions were held for religious leaders.
Peers included neighbors, adolescent girls, and visitors from nearby communities, assuming 1 per 4 dyads in reached by any intervention, based on feedback from qualitative studies and media and materials testing that showed these categories of peers shared IYCF information; mass media monitoring showed high to reach to young women 20–40 years.
Ethiopia
Health personnel were based on national norms of health provider training; 21,000 facility, outreach and community workers, and volunteers were trained based on a cascade model of training according to training lists. All trainees were drawn from government health services and community health agents approved by government. The numbers in program records were validated by the external project supervisors through observation visits, spot checks, surveys, receipts of training per diems paid, and training materials distributed.
Family members were calculated based on household survey results on family characteristics and mothers’ responses to qualitative research on from whom they seek guidance. We used a ratio of 1 per mother-child dyad reached by any intervention (1 dyad = 1/2 of mothers and children), assuming that at least additional member of the family was engaged as instructed by program staff during each home visit and during health post and health center visits where mothers were accompanied by family members. In addition, families attended community dialogues on IYCF and were exposed to mass media implemented through local audio-visual channels.
Community leaders were calculated based on monitoring data on community events and mothers’ responses to from whom they seek guidance; we used a ratio of 1/1000 dyads reached by any intervention. Formative research and the baseline survey showed that mothers sought help for CF problems from traditional healers and elders. Community inventions involved community dialogues and local media campaigns that were implemented by commercial advertising agencies to reach community-wide audiences.
Religious leaders were calculated based on program design and monitoring records for community events using a ratio of 1 per 500 mother-child dyads reached by any intervention. To build on religious teachings that support IYCF, special IYCF materials and sessions were held for leaders of the Ethiopian Orthodox Church, community-level priests, and lay leaders.
Peers included neighbors, church members, adolescent girls, and visitors from nearby communities, assuming 1 per 4 dyads in reached by any intervention, based on feedback from qualitative studies and media and materials testing that showed these categories of peers shared IYCF information; feedback from local media events showed high to reach to young women 20–40 years.
Vietnam
Program records showed that 16,500 health personnel from government health centers, village volunteers, and NGOs managing community support groups were trained. The numbers in program records were validated by the external project supervisors through observation visits, spot checks, surveys of health workers and receipts of training per diems paid, and training materials distributed.
Family members were calculated based on survey results on household characteristics and mothers’ responses to who influences IYCF; we used a ratio of 1 family member per mother-child dyad that was reached by any intervention (1 dyad = 1/2 of mothers and children) to calculate numbers. Formative research and baseline and end-line surveys showed that mothers were influenced by their husbands. The project utilized village volunteers to make home visits and issued invitations to families to bring children for IYCF counseling. Additionally, mass media, supermarket/outdoor displays, internet home pages on IYCF, and competitions for husbands were introduced to engage husbands and family members.
In communities served by Community Support Groups, we calculated 3 facilitators or community leaders per Support Group. This was based on training and supervision reports, materials used for counseling, and monitoring records. No religious leaders were attributed in Vietnam.
Peers were reported to play an important role. We calculated 1 per 2 dyads in Vietnam reached by any intervention.
Number of children with improved CF practices
The number of children with improved CF practices was measured through external evaluation studies that calculated incremental changes over time [9,10,11]. The findings estimated difference-in-differences in key CF practices attributable to the program interventions in Bangladesh (22%) and Vietnam (5.7%), and a pre- and post-intervention adequacy evaluation using regression models and plausibility analyses in Ethiopia (3.5%) [9,10,11]. We applied the percentages to the population of children 6-23.9 months of age residing in the IPC program areas.
Calculating unit costs
We used the average annual total cost per year and participants reached per year to estimate the unit costs defined for three metrics: (1) the cost per mother and children reached; (2) the cost per mother, child, and influential individual reached, and (3) the cost per additional child 6 to 23.9 months of age who benefited from MAD, as defined by WHO. We divided the total annual cost by the number of participants reached each year, using the numbers for mother and child reached, the number of mothers, children and influential individuals reached, and number of target children 6-23.9 months old in IPC areas each year with improved practices.
Sensitivity analysis
We identified the calculation of mothers and children reached as a topic of uncertainty since rigorous evaluations were conducted in a sub-set of IPC program areas where the intensity of program efforts may have been higher than in scaled-up program areas. In the ‘base scenario’ we lowered participant coverage as warranted by the program models in each country. In addition, the percentage of participants reached in each country was further reduced by 15% in all countries and used to calculate alternative unit costs.







Comments (0)