
Remember me
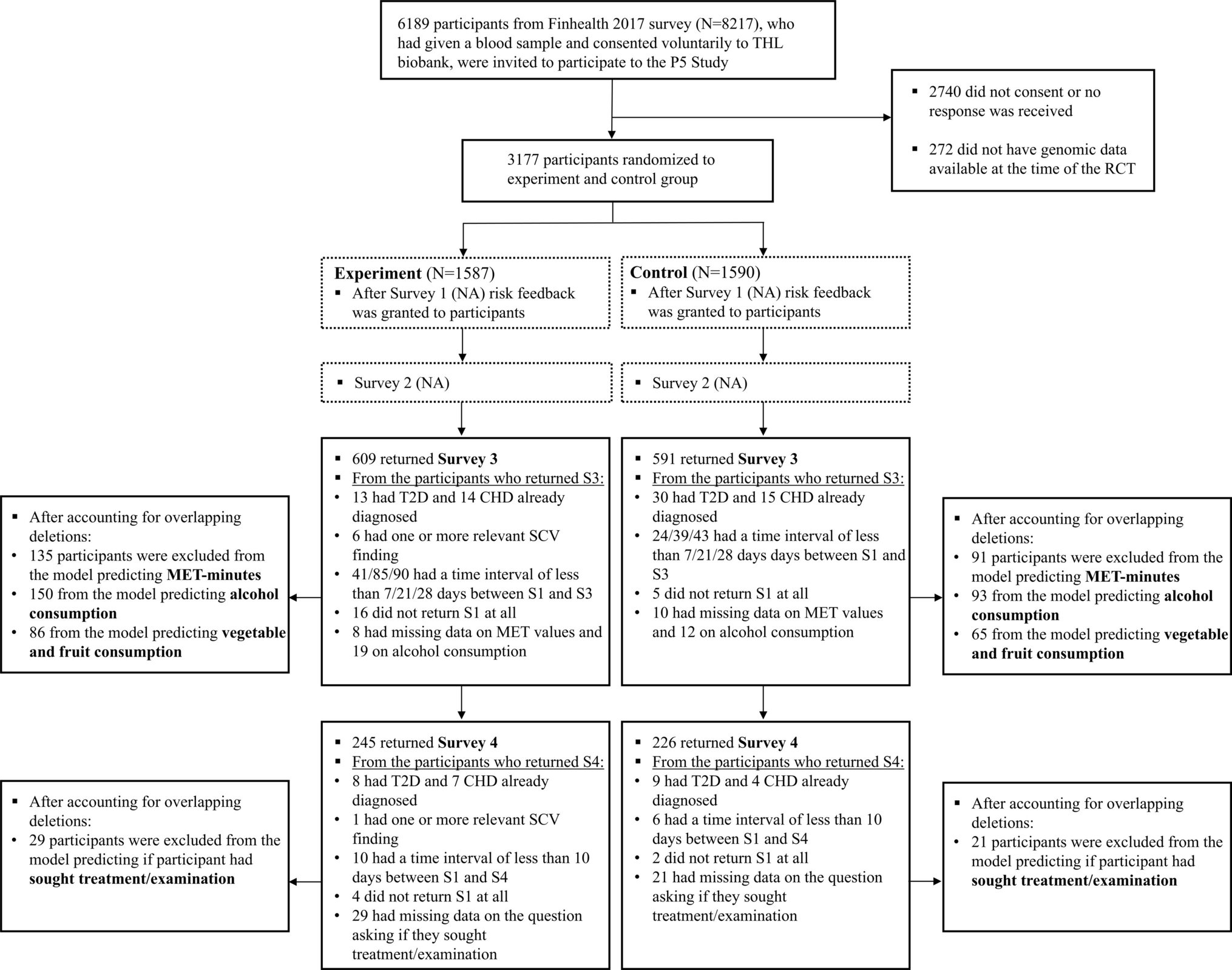
In total, 17/23 participants, who were directly approached, agreed to participate and were interviewed (74% recruitment rate). We are unsure how many people saw the study invitation through mailing lists for NHS email networks and professional bodies and as a result the overall response rate cannot be calculated. Interviews lasted between 34 and 92 min (median = 51 min).
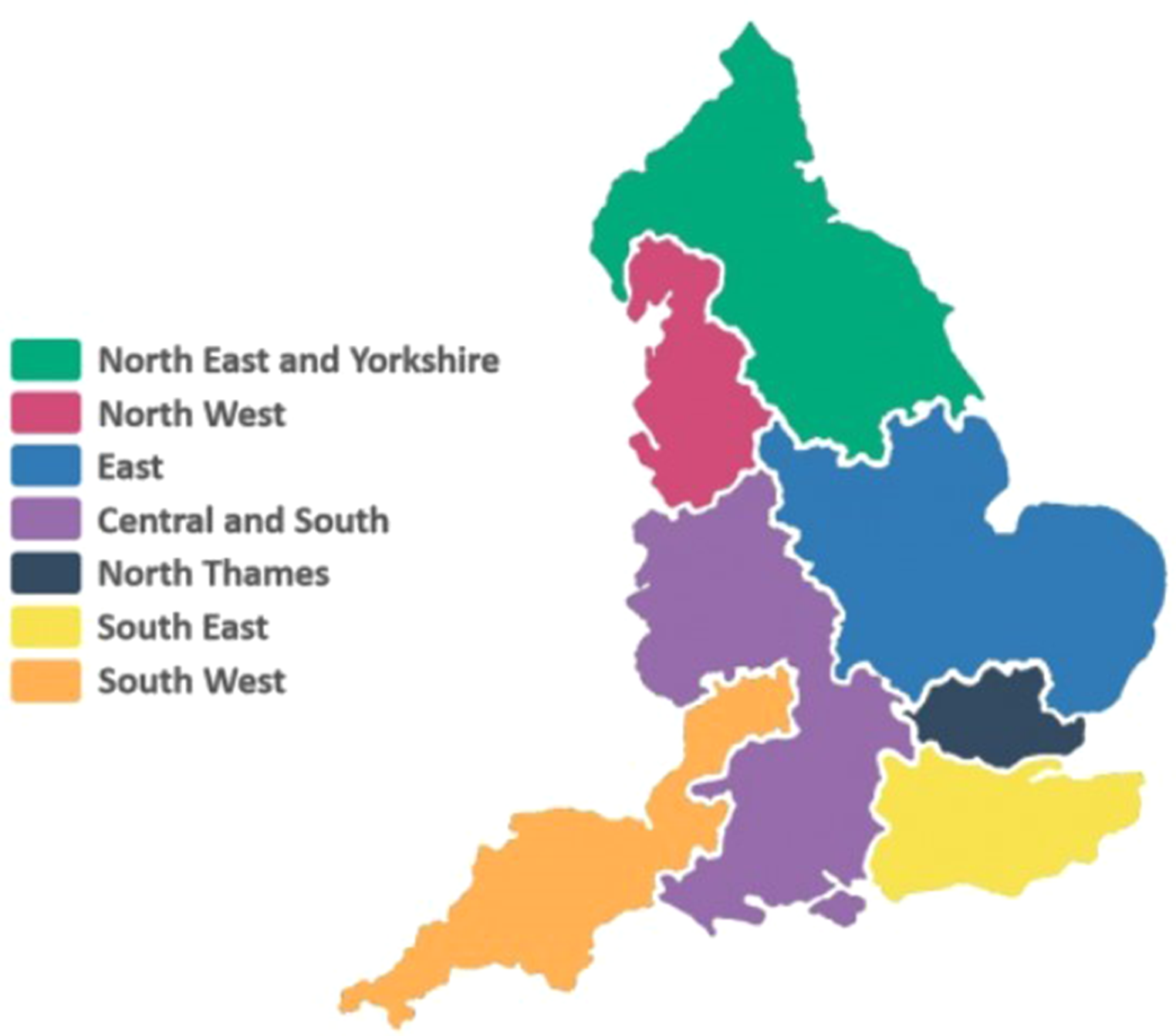
Participant characteristics are summarised in Table 1. Most participants were between 45 and 54 years old, were at consultant level and had been in their current role for over one year. In total, participants from 14 different NHS trusts participated, with most based in the North Thames GMSA. Most (n = 16) participants were community-based at the time of interview; however, one was currently a hospital-based paediatrician, but whose recent training comprised 1 year in community paediatrics.
Table 1 Summary of participant characteristicsFindingsOur findings are presented according to the domains (in bold) and sub-domains (underlined) of the COM-B model: Capability (psychological and physical); Opportunity (physical and social); Motivation (reflective and automatic) along with the inductive codes within each of these subthemes (in italics). We have also highlighted where findings relate to strategies for interventions which most notably occurred in the Opportunity and Motivation domains. The study-specific findings are depicted diagrammatically in Fig. 2.
CapabilityThe capability domain refers to whether participants have the knowledge, skills and abilities required to engage in a particular behaviour, in this context incorporating genomic medicine in their practice.
Psychological capabilityThis relates to CPs’ preparedness for GM as well as their current perceived knowledge of genetics, genomics and the GMS.
Preparedness for GMThere was variability in how prepared participants felt they were to deliver GM in their practice. A lack of preparedness amongst participants was reported with some describing themselves as “not knowing enough”. One participant commented that:
“I think if you asked me to write an essay on what I thought an exome and genome and what everything was, I think I’d fail.” (Participant 13).
However, most understood that they would soon be required to have greater involvement with GM and therefore needed to upskill.
Knowledge of genetics and genomicsMost participants felt that they had a baseline understanding of genetic concepts, e.g., including inheritance patterns, monogenic conditions, and disorders seen more frequently in consanguineous populations.
“So I was talking to them about. obvious syndromic and not obvious syndromic, and going through chromosomes, recessive and different syndromes. and mitochondrial diseases and things, so I could do that in my sleep actually.” (Participant 13).
“I’d say a lot of them [patients] do have consanguinity, so even when we don’t have a diagnosis from microarray or whatnot, you get the idea is that it probably is genetic in some degree” (Participant 3).
Several participants made comments that highlighted their familiarity in identifying a child that might have a genetic condition and had ordered genetic tests in the past including microarray:
“We can often see that there’s a family history or there’s a pattern and it doesn’t always show up anything on microarray but it’s quite clear that there’s something going on genetically” (Participant 11).
Participants had a greater involvement with earlier forms of gene testing i.e., karyotyping, microarray and single gene testing, than advanced genomic testing. However, some participants demonstrated a greater understanding, referencing WGS diagnostic rates and the genes on specific panels. There was no observable pattern with regards to knowledge (about genomic testing) and participant characteristics (such as age or location). Some participants displayed an understanding of issues pertinent specifically to WGS, e.g., the greater chance of detecting variants of uncertain significance with WGS compared with when doing targeted tests:
“If you already know exactly what monogenic condition you’re thinking about then it’s probably more appropriate just to test for that, considering we know that WGS has significant increased risk of variants of uncertain significance” (Participant 3).
Overall, responses suggested participants were well-versed in the aspects of genetics that related to their specific roles and experience. Most participants had no formal genetics education prior to the initiation of the GMS and had acquired their knowledge through professional experience. Some reasoned that this was due to how long ago they trained in medicine; genomics was not part of their syllabus, and they trained before the development of advanced sequencing technologies.
Understanding the purpose of the genomic medicine serviceAll participants except one was familiar with the GMS. Participants identified several different objectives for the GMS; the most common related to improving patients’ access to genomic testing regardless of where in the country they live:
“It was to make sure there was equitable coverage across England” (Participant 13).
Some were familiar with the restructuring of regional services into the seven GLHs, with specific laboratories responsible for specialised testing: “Experts level of analysis can take place in certain centres” (Participant 3). Additionally, some participants referenced the National Genomic Test Directory, which was described as useful for standardising genomic testing for patients with a given phenotype regardless of geographical location.
Physical capabilityThis relates to participants’ current level of ability to carry out GM-related work, for example, pre-test counselling, taking consent, ordering tests, interpreting and delivering results.
Experience with genomic testing: consenting and requesting testsMost participants were experienced in consenting for earlier forms of gene testing, though not for larger panels, WES or WGS. Only a small number had consented patients for WGS in the 100,000 Genomes Project. There was an observable difference between the one hospital-based participant and community-based participants in terms of their experience consenting for WGS in the GMS. The hospital-based paediatrician had significantly greater experience: “The Record of Discussion [consent form used for WGS] I’ve definitely done over say fifty times” (Participant 16). In comparison, few of the other participants were well-versed with the consent process.
“I think I’d have to do some homework in terms of the consent process” (Participant 7).
One participant was critical about consent more broadly for genetic testing undertaken by non-genetics specialists:
“The whole consent process that happens in the NHS, I mean as a genetic counsellor I think you would cringe when you hear how genetics are discussed in the majority of cases” (Participant 12).
The minority of participants who had ordered larger gene panels, reported difficulties obtaining clarification on which genes could be tested individually vs. only on WGS testing.
Experience with genomic testing: delivering resultsParticipants acknowledged the complexities brought about by WES and WGS. Most participants had not yet delivered results from these tests but felt that they would be more confident in communicating results if they had direct experience with the condition:
“If it’s straight-forward, if it’s a condition I know things about then I think I would feel comfortable. So, I think it just depends on the condition” (Participant 12).
However, it was acknowledged that when microarrays were first introduced, CPs had to upskill in this technology and, in that respect, WGS was comparable.
OpportunityThe opportunity domain refers to factors outside the control of the individual that impacts their adoption and implementation behaviour such as resources and time.
Physical opportunityThis relates to the resources that are currently available for implementation of GM.
General resources and fundingFunding constraints underpinned many participants’ concerns with regards to implementing GM. Some described being asked to do something that they are “not funded for”, and healthcare being in “severe austerity”, which made the prospect of additional funding unlikely.
“The thing is that we’re not trying to be difficult, it’s just that they keep giving us stuff without extra resources, time or money” (Participant 15).
Relatedly, a further concern was balancing resources against the potential increase in children eligible for WGS. Participants reflected that it would be like “opening up a can of worms”. One participant estimated that they had around 250 existing patients who could be eligible for WGS.
“What I’m not sure about is how ready genetics services are for quite how many patients there are going to be that would then be referred for genomic testing! … that’s almost every child that I see in my clinics!” (Participant 3).
TimeParticipants communicated being already overstretched, without the additional burden of organising genomic testing. They expressed concern that discussing the pros and cons of testing, consenting patients, and completing the associated forms would be excessively time-consuming. One described the burden of adding in these tasks to their existing workload as “the straw that’s breaking the camel’s back” (Participant 13).
Some participants felt that other areas of patient care would suffer if they had to include genomic testing within a standard appointment:
“I just can’t see how I can do that without compromising on the rest of my clinical care for that patient” (Participant 15).
WorkforceAround two thirds of participants commented on the lack of human resources to deliver GM within their roles. Participants highlighted a lack of clinical and administrative support for tasks including pre-test counselling, consenting, obtaining trio samples for WGS, and chasing blood samples. One participant summarised: “I think the big elephant in the room that’s always there is ‘who’s going to do it?’” (Participant 12). Others were more optimistic, suggesting that the process would become more streamlined over time, and would ultimately reduce resource burden.
Some participants perceived a workforce disparity between hospitals having seen support roles advertised at other sites.
“What I think people have not understood very clearly is how certain regions have been able to get resources with genomic assistants, whereas other regions are saying no we can’t, we can’t provide that” (Participant 1).
Involvement in mainstreamingParticipants agreed that offering genomic testing in the GMS was not a departmental priority and models of service delivery had not yet been established in any of their departments. There were disparities in participants’ experiences with regards to ordering WGS. In some, there was confusion about whether their specialty was permitted to order WGS:
“It’s all been a bit confusing, so basically it’s like well I’m not doing that then, I’ll refer you to genetics!” (Participant 13).
One participant knew of neurology colleagues within the same trust who were able to order WGS, an option not available to CPs. Only a small minority of participants reported already having ordered WES or WGS tests themselves.
Social opportunityThis includes access to educational opportunities and support from colleagues, including genetics specialists and management.
EducationParticipants reflected on specific interventions such as education and training, that had been set up to upskill mainstream clinicians. Many participants had accessed educational sessions, delivered mainly by GMSA representatives and colleagues from Clinical Genetics departments. Participants had engaged with training opportunities on topics including the sequencing technologies available, paediatric mainstreaming, consenting and communication skills. The varying formats included virtual webinars, continuing professional development (CPD) modules, workshops and signposting to educational websites. Participants cited the online resources they had accessed genomics education through, including Genomics England, FutureLearn, the GMSA, local Clinical Networks, British Academy of Childhood Disability and the Royal College of Paediatricians and Child Health. A small number of participants had not accessed educational resources on GM, citing that they were not sure where to locate resources or whether the resources were intended for CPs. The following quote relates to accessing genomic medicine educational resources:
“Where is it advertised? Where can you find out about these things? Because there must be people like me that are interested and just haven’t managed to find that education resource” (Participant 6).
Most participants knew where to access GM educational resources but recognised a demand for more, and highlighted the need for improved accessibility amongst their colleagues:
“It has happened quite quickly and yes there has been education, but not everybody’s been able to access it. I think a lot of people haven’t realised that they need to” (Participant 4).
Competing priorities were mentioned as a barrier to participants accessing educational sessions.
“This is the first time I’m attending tomorrow so it’s on a fixed day and then many people if they clinic on that day, we can’t attend” (participant 2 referring to an educational genetics meeting).
“But again, it comes down to time to be able to attend all these things and so forth. There isn’t unlimited time to access these things.” (Participant 7).
The voluntary nature of the sessions also meant that engagement relied on the individual “drive” of CPs to engage with the educational resources. Notably, one participant had a colleague who “didn’t believe in genetic testing, because he didn’t see the value of it” (Participant 17) and this participant had worked to engage their colleague through resources evidencing its clinical utility.
Organisational structure and management supportParticipants reported that there had been a lack of discussion and engagement initiated by those implementing the new service.
“At a strategic level there did not seem to have been any conversations, which is really sad, and I would’ve expected that to happen” (Participant 1).
Several participants expressed feeling left to “fight on their own”.
Support from colleaguesOverall, participants felt well-supported by their peers, including colleagues from clinical genetics. There were examples of colleagues from general paediatrics who were highly supportive in directing CPs to mainstreaming education. However, a small number of participants thought that their genetics colleagues should be taking on more of the work around genomic testing as it was their field of expertise and they perceived them to have more time allocated to this.
One interviewee suggested that the differences in engagement between their colleagues might be due to differences in the genomics training experienced by older and younger colleagues:
“There’s that risk that often you’ll see that the trainees coming through and the younger members of the team are more au fait with this sort of stuff and the older stick-in-the-muds like me are kind of less well versed in it than some” (Participant 7).
Multidisciplinary team (MDT) meetings and interest groupsRoutinely organised MDT meetings were valued as being beneficial for up-skilling and seeking input for complex patients. Approximately half of participants had attended MDT meetings with clinical genetics colleagues. Many found the virtual nature of the meetings helpful, allowing them to join despite other clinical priorities.
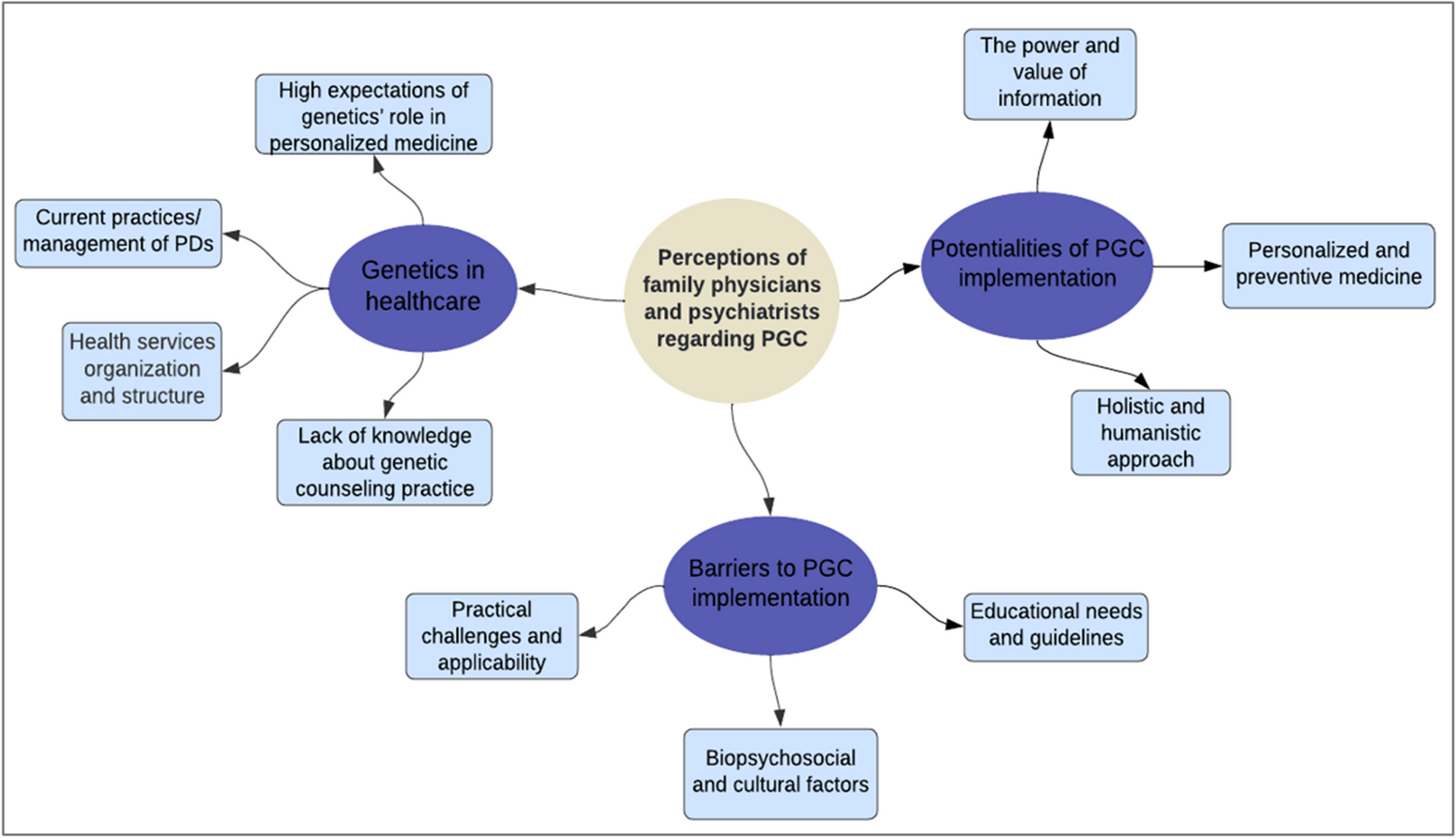
Fig. 2
Radial cluster diagram summarising our study-specific findings within each sub-theme of the COM-B model
MotivationThis domain refers to the internal processes that influence decision-making in the context of carrying out the behaviour.
Reflective motivationThis refers to participants’ confidence as well as their considered opinions about the GMS, including their desires to be involved with it, and suggested solutions and improvements to enabling GM.
Confidence in involvement with genomic testingSeveral participants highlighted their hesitancy and discomfort in using WGS, mainly due to their unfamiliarity with the process and concerns about interpreting complex results.
“People have anxieties about filling a form, simple as that. You know the first thing which comes to mind for a person who you are asking to – ‘which form do I fill?’ ‘Where do I send?’ ‘How do I do the test?’ (Participant 2).
Others described feeling less confident about their involvement, “I’m sure we don’t do it as well as we should do and it’s very basic” (Participant 14).
Many participants communicated that they would feel most comfortable referring a patient to clinical genetics for their support when more complex testing discussions were indicated. This included covering the “grey areas” of testing such as unexpected results and discussing additional complexities like non-paternity.
Strategies noted by participants to address lack of confidence amongst CPs included having greater involvement with GM, which participants expected would lead to an improvement in their competence and confidence over time: “If they’ve [CPs] done it ten times they will feel more confident” (Participant 2). They also appreciated the need to understand the “nuts and bolts” of the process, referencing practical elements such as navigating the lengthy National Genomic Test Directory, using the correct forms, and knowing the correct testing turnaround times.
WorkforceOther strategies identified by participants to counter the behavioural barriers to implementing GM in community paediatrics related to the workforce. This included additional funding to recruit staff such as genomic associates whose main roles would be to support the department, including: consenting patients, completing paperwork, chasing samples and submitting test requests to the lab. They felt that this would ensure the GM processes were “joined-up”. They recognised that employing someone to this role would be cheaper and more efficient than a consultant having to take on this work which was currently taking away valuable time from their main role. Participants also proposed developing a ‘genomics champion’ role within their community paediatrics team who would be responsible for promoting team training, and support colleagues with consenting patients and delivering results.
ProcessesSuggestions were also made to streamline the WGS process included improving pathways, making consent procedures tighter, and reducing the paper-based workload. Some participants proposed more easily accessible guidelines, “cheat-sheets” and provision of standard operating procedures, for example, around how many times to chase missing consent forms or blood samples.
Automatic motivationThis refers to the more instinctual and impulsive processes and opinions about the GMS held by participants, for example, whether they perceive it to be valuable.
Attitudes towards GMMany participants had a positive attitude towards GM, viewing it as having an important place within CP: “The value added I have no question about it, it is adding to our understanding” (Participant 18). Other participants foresaw their roles evolving to have a specialist interest in genomics and felt that genomic tests should be standard practice and “become [an] inseparable part of our job” (Participant 5).
The potential benefits for patients were cited as being key drivers behind their motivation for supporting the implementation of GM. They thought that the diagnostic potential in using WGS offered great opportunity for families without diagnoses.
Most participants were receptive to the implementation of GM and thought that their colleagues would feel similarly. Some described their own excitement at the prospect of utilising advanced genomic testing and described their colleagues as passionate. However, a small number of participants perceived a lack of receptivity from their colleagues, particularly those who were more senior and closer to retirement who were perhaps less open to learning something new.
“There was some apprehension from more senior members of the team who are maybe closer to retirement stage and how they then learn something new and different” (Participant 11).
Comments (0)