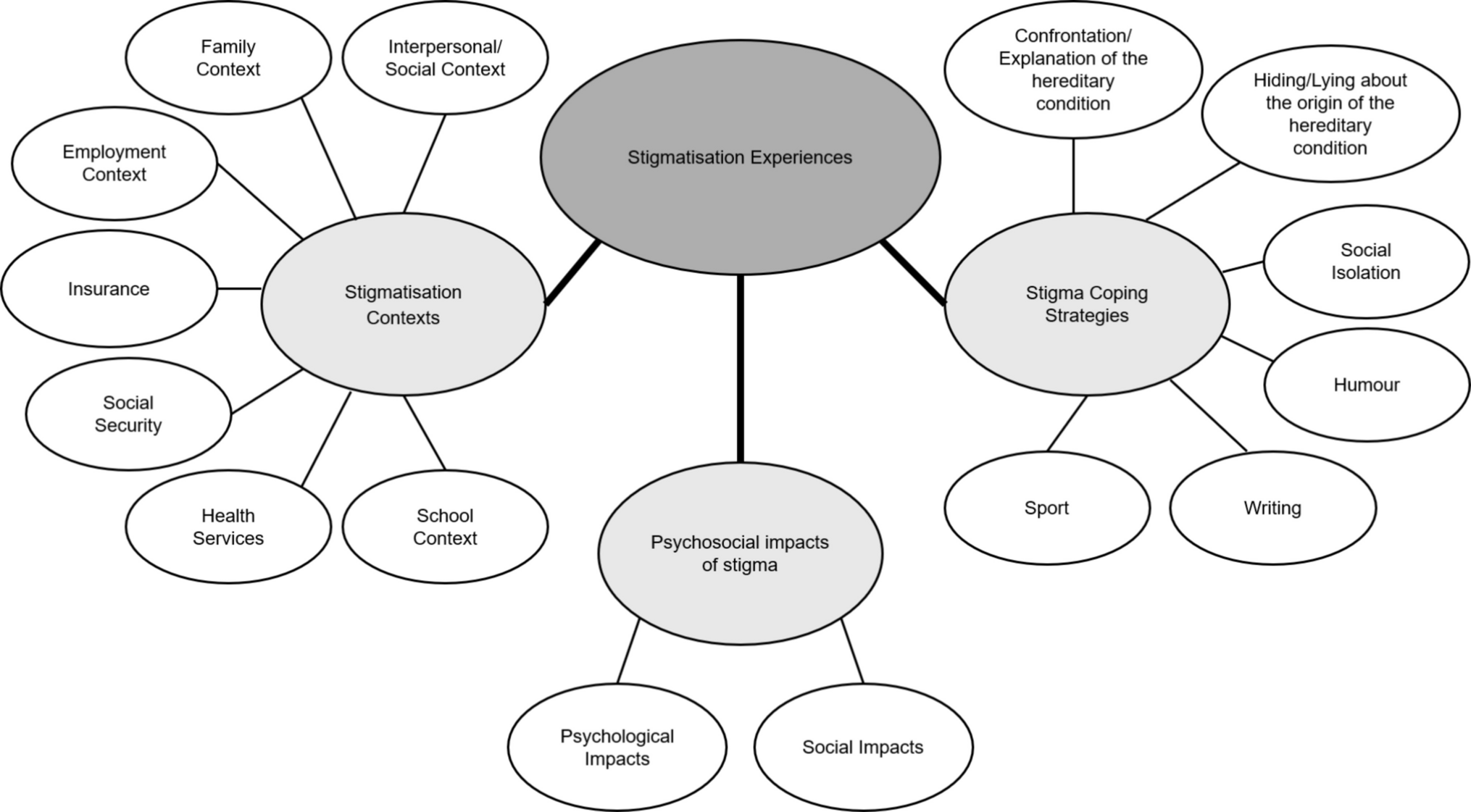
This is the first study that reports stigmatisation experiences of people with a group of hereditary conditions and their families in Portugal. The main results suggest that: (i) stigmatisation can be found in familiar, social, school, employment, health systems, social security and in insurance contexts; (ii) stigmatisation experiences trigger frustration, anger, sadness, shame, discouragement, fear of sharing that they have a hereditary condition and worry about “being a burden”, on a psychological level; and, on a social level, isolation, withdrawal from colleagues, friends and family and disinvestment in love relationship; (iii) individuals have different ways to cope with stigma impacts, some face and explains the condition to stigmatisers, while others isolate themselves, hide and lie about the inherited condition origin, and others resort to humour, writing and sport.
Several international studies corroborate the presence of stigmatisation in different contexts (Baynam et al. 2024; Bombard et al. 2007; Estrada-Hernandez 2018; Foji et al. 2021; Henderson et al. 2009; Williams et al. 2010). Similarly to the study by Williams et al. (2010), which includes participants from Australia, Canada and United Status of America (USA), the present study pointed to experiences of stigmatisation within the family context through rejection, withdrawal and humiliation. In social context, the aforementioned study (Williams et al. 2010) and the literature review article by Baynam et al. (2024) reports that discrimination, withdrawal and rejection by strangers, acquaintances and even friends, data that are consistent with the present study. Regarding the school context, were described, in this study, episodes of physical violence, rejection by peers and extreme concern from teachers and staff, perceived as a marker of difference. The behaviour of peers is in line with the study’s results by Estrada-Hernandez (2018), conducted in Puerto Rico, where participants affected with Albinism, described being labelled and teased by their peers, and with Henderson et al. (2009) study, where Californian participants affected by Niemann-Pick Type B disease, reported difficulties in making friends and participating in events. Foji et al. (2021), which studied the experience of living with Neurofibromatosis in many provinces of Iran, highlighted in their results the difficulty in finding a job and reported that they had been fired from their jobs due to the physical limitations of the disease and the observable characteristics of the condition. In our study, in the employment context, the participants felt and believed that they were not chosen for jobs because of the presence of the condition. Our results further corroborate the results of Bombard et al. (2007) in relation to misunderstanding of work colleagues concerning the experience of Huntington disease in Canada. In the present study, social security seemed to emphasize the difference felt by the participants throughout the lack of response regarding the acquisition of certificates and monetary funds to which they are entitled and the reimbursement of necessary therapies. The same happened with healthcare services, the perceived insensitive treatment of both patients and their families by doctors and nurses was felt as a marker of difference, in particular, compared to the treatment of acute situations. The reduced accessibility to health services, as well as discrimination felt within them, were also highlighted in Silva et al. (2013) study, in Brazilian context in participants with Sickle Cell Anaemia. Regarding insurance companies, in the study by Williams et al. (2010), the results indicate life insurance denied due to the presence of a hereditary condition, that may explain the participants fear in this study of being harmed by the existence of a hereditary condition, as reported in Bombard et al. (2007) study, from Canada.
Also, the psychological impacts associated with stigma found in this study are consistent with the literature: frustration, anger and sadness (Fournier et al. 2023), shame (Baynam et al. 2024; Fournier et al. 2023), discouragement (Williams et al. 2010), the fear of sharing they have a hereditary condition (Bombard et al. 2007) and concern about “being a burden” (Estrada-Hernandez 2018). In social context, stigma experiences seemed to generate isolation, but also withdrawal from colleagues, friends and family. Foji et al. (2021) mentioned the disinvestment in love relationships due to the belief that no one will want a person with a hereditary condition (Neurofibromatosis), also observed in our results. In addition, the present study suggests as a reason for disinvestment in love relationships the concern about “being a burden” and the participants knowledge of other stories of couples who have broken up due to the presence of a hereditary condition.
In Bombard et al. (2007) study, Canadian participants faced and explained characteristics and symptoms of Huntington disease to stigmatisers as a way of protecting themselves. In present study, these were also the ways more used by participants to cope with stigma, alongside social isolation. Isolation, due to rejection fear and to avoid hearing discriminatory comments also arises as a strategy to cope with stigma in Foji et al. (2021) study with participants affected by neurofibromatosis. In our study other participants choose to try to hide the hereditary condition and lie about their origin. The strategy of hiding the hereditary condition as much as possible or sharing the diagnosis only with close family members was also documented in the Bombard et al. (2007) and Williams et al. (2010) studies, both with participants affected or at risk of inheriting the Huntington disease. Other strategies reported in the current study, that seemed to improve people well-being regarding stigmatisation experiences, included writing, humour and sport.
In summary, these results suggest that living with a hereditary condition has implications which make psychosocial adaptation difficult for those affected and their families, with social isolation standing out. The presence of a hereditary condition in a family already brings several challenges of high complexity on its own: frequent role changes, particularly due to loss of autonomy and consequent dependence on (in)formal care; adaptation to the condition, in particular, when it manifests itself at a younger age; communication about the hereditary condition with family; among others (Street and Soldan 1998). All these challenges have impacts on the family life cycle and on family dynamics (Rolland 2018). When a disease arises in the family, this tends to turn inwards, and despite the support the family can give each other in this phase of heightened fragility, this centripetal movement can immediately reinforce the isolation of the family and the individual with a hereditary condition and increase their suffering (Rolland 2018). Besides this, when a inherited condition involves informal care, the responsible member often must quit their job and doesn’t have much time to devote to social gatherings, which is why people in their social support gradually distance themselves. Naturally, these changes in family life bring a lot of fear, worry and sadness. Our study suggests that these families also face social difficulties amplified in various contexts, which reinforce isolation. Rejection, exclusion, the stares, comments, the labelling that people living with a hereditary condition receive make them feel different, frustrated and ashamed, which leads them to develop ways of dealing with stigmatisation, namely through isolation. In other words, the exclusion of other people leads to their own exclusion, as if it were a “vicious cycle of isolation”. This isolation is associated with intense emotions of fear, sadness and shame, which in many cases translates into deep psychological suffering. In this regard, it is important to work with these families to help them integrate these experiences and “re-signify” the experience of living with a hereditary condition, for example, through family therapy (Dane et al. 2024; Zarei and Roohafza 2018), multifamily therapy (Guerra et al. 2023) or group therapy (Dane et al. 2024). Multifamily and group therapies seem very suitable for counteracting isolation, since this allows families to explore realities like their own, which is essential to normalise their experiences, emotions and thoughts (Dane et al. 2024; Guerra et al. 2023). Moreover, membership in support associations for patients and families with inherited conditions can also be a good way to counteract the difference felt. Associations seem to have a positive impact on the lives of those living with a hereditary condition, since by mobilising meaningful relationships between members, associations reduce isolation and, more importantly, seek opportunities to integrate patients into the community (Costa et al. 2022). Therefore, it is possible to rebuild identity and find more positive strategies for coping with stigma, such as education about hereditary conditions.

Comments (0)