
Remember me
Anorexia nervosa (AN) is a severe psychiatric illness with a high rate of mortality [1]. Long-term outcomes are often disappointing, marked by high rates of relapse and chronicity [2, 3, 4]. Understanding why maladaptive behaviors persist, even in individuals seeking recovery, is crucial. To do so researchers have turned to the neurocognitive mechanisms underlying these behaviors, increasingly with particular attention to habits. This review examines the status of neurocognitive research on the role of habits in AN, focusing on recent insights from task-based assessments and their contributions to advancing our understanding. Recent studies of the relevant neural circuitry and general methods of assessing habits will be briefly reviewed, followed by a more detailed analysis of the main task-based approaches. Finally, the challenges to this program of research and approaches for meeting those challenges will be outlined.
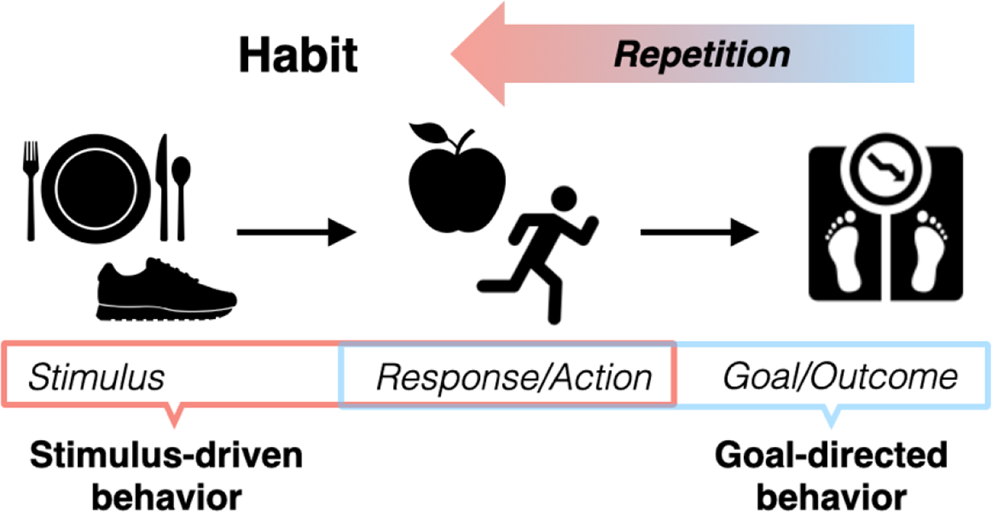
The Habit Framework as a Guide for Studying Neurocognitive Mechanisms of Anorexia NervosaHabits are learned behaviors that through repetition become fixed and relatively insensitive to their outcomes [5, 6]. This process is adaptive, allowing efficient execution of frequent behaviors, freeing cognitive resources for other tasks. However, in psychiatric illness, this learning process may be co-opted towards maladaptive ends. Habits may begin as intentional, goal-directed behaviors, guided by response-outcome associations but, through repeated reinforcement, shift to automatic responses triggered by specific cues or contexts (i.e., guided by stimulus-response associations) [6, 7, 8, 9, 10] (see Fig. 1).
Fig. 1
Habit development. Habits are learned behaviors that emerge through repetition. Behavior may begin as an intentional and goal-directed action (dieting to lose weight) in response to a stimulus or setting (food/mealtime) and reinforced by a rewarding outcome (weight loss). As the behavior is repeated and reinforced, it may shift to a more automated response triggered by food stimuli or contexts, regardless of whether the outcome of the action is still desired
Maladaptive eating behaviors observed in AN, such as extreme food restriction, align with this habit framework. Restrictive eating behavior may begin as casual dieting, reinforced by positive feedback or a sense of achievement, but over time it may persist without reinforcement—despite awareness of its harmful consequences [11, 12]. Similar trajectories may apply to other behaviors, such as excessive exercise [13]. The automaticity of habits is also relevant. Behavioral routines can become “chunked” into sequences that, once initiated, continue until conclusion without deliberate control [14]. In a similar vein, eating behavior in AN can take on a relatively stereotyped character, including limited diet variety [15, 16, 17] and rigid routines around eating [18, 19]. The challenge associated with avoiding automatic behavior patterns and the effort required to modify or eliminate entrenched routines, is a challenge familiar even in everyday habits (e.g., when you take the usual route home instead of buying groceries as intended).
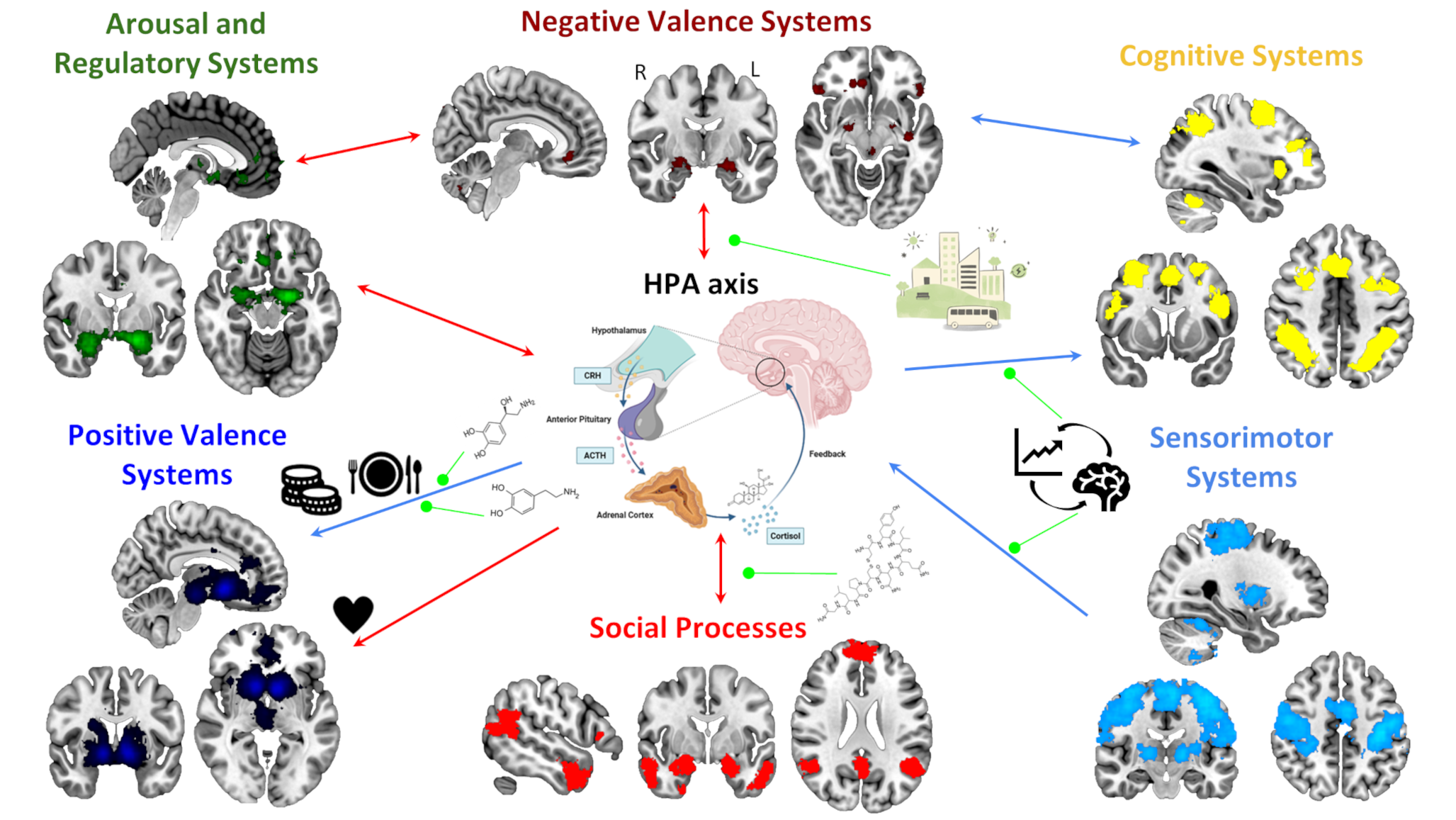
Considering behaviors as habits is only a starting point for understanding the neurocognitive mechanisms of AN and improving treatment [12, 20, 21, 22]. The habit model provides a framework for investigating AN at neural and behavioral levels, leveraging extensive research on habits in psychology and neuroscience. The distinction between goal-directed and habitual behaviors has been studied in the context of learning theory, cognitive neuroscience, and computational models [6, 8, 9, 10, 23, 24, 25, 26, 27, 28]. Behavioral paradigms to measure habitual and goal-directed behavior [29] complement self-report measures [30], while studies across animals and humans [27, 31, 32, 33, 34, 35] have identified ventral and dorsal frontostriatal circuits (Fig. 2) [6, 36, 37] and dopamine as critical for learning and behavior [38, 39, 40, 41].
Building on this literature, research on AN has begun to examine the neural circuits involved in habit formation and goal-directed behavior. Recent studies have linked neural abnormalities to habitual tendencies, and a small, but growing, number of behavioral experiments directly examine habits in this population. These efforts will be the focus of the current review.
Fig. 2
Frontostriatal circuits loops involved in habitual and goal-directed behavior
Abnormalities in Frontostriatal Circuits Associated with Habitual and Goal-Directed BehaviorIf dysregulation of habitual vs. goal-directed control of behavior plays a role in AN, neural circuits supporting these behaviors should show evidence of dysfunction. Indeed, structural neuroimaging studies, across a variety of measures [42, 43, 44, 45, 46, 47, 48], have identified abnormalities in frontostriatal circuits. Functional neuroimaging studies, both resting state [21, 49, 50, 51] and task-based [52, 53, 54, 55, 56, 57, 58, 59, 60, 61], provide additional evidence for abnormalities in these circuits.
Most studies have not, thus far, assessed habits directly, but some recent studies have attempted to do so indirectly. One study reported greater white-matter connectivity measures in habit-associated pre-motor/SMA-putamen circuits among individuals with AN, relative to healthy controls, and that connectivity measures were associated with severity on the Rituals subscale of the Yale-Brown-Cornell Eating Disorder Scale [46] among individuals with AN. Another study reported an association between cerebral metabolite measures in inferior frontal cortex and Automaticity scores on the Creature of Habit ScaleFootnote 1 among individuals with the binge-eating/purging subtype of AN [62]. Finally, Lloyd et al. [63] reported (in exploratory analyses) that among individuals with AN, choice-related activity on a Food Choice Task [64] in the anterior caudate region of the striatum was associated with scores on the Self-Report Habit Index (SRHI). Other recent neuroimaging studies have linked abnormalities in frontostriatal circuits to weight or food intake. For example, Gorrell et al. [65] found that OFC response among patients with AN when expecting a sweet taste was related to longer-term BMI and BMI change after treatment. A set of studies using the Food Choice task showed associations between food choice-related activation in the caudate and caloric intake in a laboratory meal [56] and between pre- to post-treatment changes in caudate activity and changes in food choices [55] among individuals with AN. Although these studies do not affirm a role for habits in food restriction or other maladaptive behaviors, they demonstrate that dysfunction in brain circuits implicated in habitual and goal-directed behaviors is related to self-reported habitual tendencies or illness.
Notably, frontostriatal circuits are critically innervated by dopamine [66], which is thought to be important for both habitual and goal-directed behaviors [39, 40, 67]. Dopamine plays a role in propagating learning signals and conveying motivational significance [41, 68, 69, 70, 71] and has been linked to feeding in animals [72, 73]. Consequently, it is speculated that dopaminergic dysfunction plays some role in AN and, though they do not measure dopamine function, fMRI studies are often discussed as implicating a role for dopamine. Few studies have directly measured dopamine function in individuals with AN and have yielded mixed result—increased, decreased, or no differences in dopamine levels or activity [74, 75, 76]. Until recently, examination of dopamine has depended on somewhat invasive measures (lumbar puncture, PET, blood draws), but developments in imaging techniques [77] will likely yield more investigations of dopamine function in AN (e.g [78]).
Studying Habits in Anorexia Nervosa: Self-ReportSeveral studies testing the role of habits in AN have used the Self-Reported Habit Index (SRHI; [30] and found that habit strength of food restriction predicted (self-reported) restriction [79], that interventions to interrupt maladaptive eating routines by interfering with trigger cues can decrease habit strength [22], and that longer illness duration and illness severity is associated with greater habit strength [80]. These studies established that behaviors central to illness were characterized as habitual in nature by individuals with AN.
A recent study used ecological momentary assessments (EMA) to assess the frequency of both food and non-food related (hygiene) habits in daily life [81] and found that patients with AN reported more food and non-food habits relative to healthy controls. However, surprisingly, patients with AN did not report higher habit strength, per the SRHI, for those habits relative to controls, nor for food relative to non-food habits. Perhaps the sample, comprising mainly adolescents with a short duration of illness, or the types of habits it is possible to report in an inpatient setting, played a role. Regardless, capturing habits more directly, as they unfold in the real world, will be important to better understand how they contribute to illness.
Studying Habits in Anorexia Nervosa: Learning TasksA promise of the habit framework is that it might illuminate the mechanisms of maladaptive eating (and other) behaviors—how they arise, are maintained, why they are so persistent, and why they are prone to reoccurrence after treatment. Self-report questionnaires are not informative on this topic and more experimental behavioral research to examine habit mechanisms in AN has been encouraged [21]. Yet studies remain scarce and results mixed.
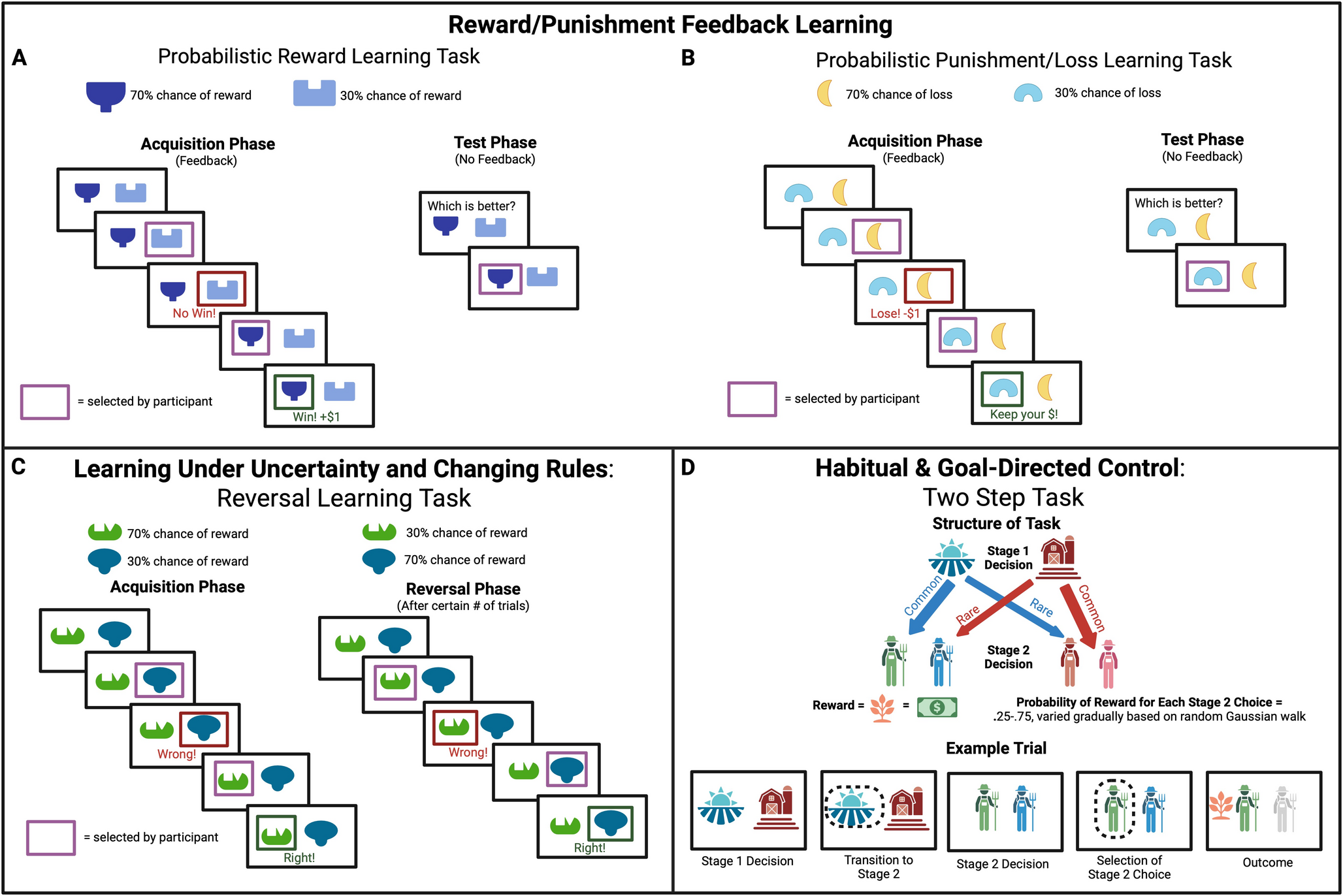
The limited number of studies directly examining habits may stem from the inherent challenges of studying them in a laboratory setting [29] paired with additional challenges in eating disorder populations. In real-world contexts, habits develop gradually over time, and much of our understanding of habits comes from animal studies with extensive training sessions. One paradigm that captured habitual behavior over extended training relied on consumption of desirable foods until satiation [32] making it unsuitable for use in individuals with AN in addition to the practical difficulty with long training protocols. However, other approaches developed to study habits in humans (Fig. 3) have been employed widely in psychiatric illnesses (e.g., OCD [82]; substance use disorder [83]; alcohol dependence [84]) and have now been applied to the study of AN.
Outcome Devaluation TasksOutcome devaluation, decreasing the motivational value of an outcome (e.g., pairing a food with illness or feeding until satiation), is a standard tool to test whether behavior is habitual or goal-directed [84, 85, 86]. If an action is triggered by cues in the environment rather than the value of its associated outcome, then behavior should be insensitive to the value shift resulting from devaluation.
Godier and colleagues, who conducted one of the first task-based assessment of habits in AN, used two tasks with outcome devaluation procedures [88]. One, the Slips of Action task, pits habitual stimulus-response learning and goal-directed response-outcome learning against each other to assess their relative influence (see Fig. 3b). Participants learn whether to make a left or right button response in the presence of a discriminative stimulus to receive a specific outcome picture and reward. In an outcome devaluation manipulation, participants are informed which outcomes no longer are valuable and which still are valuable. Then, in a “slips-of-action” phase, participants are shown the discriminative stimuli and should respond to those that lead to still-valuable outcomes and not to those that lead to devalued outcomes. Stronger stimulus-response habits should yield more responses to the stimuli that previously led to reward despite the outcomes no longer being valuable. Across two experiments, the balance between habitual and goal-directed responding did not differ between individuals with AN and controls [88].
Another experiment reported by Godier and colleagues used an avoidance task in which participants learn by trial-and-error to make responses to avoid an aversive outcome (here an unpleasant noise, commonly a mild electric shock) signaled by discriminative cues. Following training, one outcome is “devalued”, in this study by disconnecting the headphone delivering noise to one ear, and participants continue to make responses to the discriminative cues. Habitual behavior is indicated by continued response to cues signaling devalued outcomes. In this study, individuals with AN and control participants did not differ significantly [88].
Two recent task-based assessments of habits among AN used Slips of Action tasks. Favier and colleagues found a shift towards habits among patients with the restricting subtype of AN [89], whereas Westwater and colleagues, who included only AN participants with the binge-eating/purging subtype, did not find significant differences between AN and control participants [62]. Thus, for outcome devaluation type tasks, a preponderance of the evidence does not indicate a stronger propensity towards habits among individuals with AN.
Two-Step TasksTwo-step Markov decision tasks have been used extensively in psychiatric populations [83] and recently also with individuals with AN [90, 91]. The task design stems from the idea that habitual and goal-directed behaviors are associated with distinct computational algorithms identified as model-free and model-based learning [26, 38]. Whereas model-free learning is characterized by direct reinforcement of actions that lead to reward, model-based learning additionally accounts for task structure when evaluating actions. To capture this distinction, the task proceeds in two steps. Choices at the first step lead to distinct second steps at which choice can lead to reward (or punishment). Critically, choice at the first step is probabilistically associated with a transition to a given second-step cue pair. This transition structure allows dissociat
Comments (0)