
Remember me
The study included 123 patients with HAE (Table 1). The majority of patients were female (81%) compared to male (19%), and a mean age of 44.9 years (18–83; 14.4 standard deviation (SD)), with most patients being between 34 and 44 years of age (28%). The majority of patients reported HAE-1 (46%), followed by HAE nC1-INH (24%), and HAE-2 (14%); additionally, 16% of patients were unsure of the type of HAE they had. The mean ages of HAE symptom onset, HAE diagnosis, and HAE treatment initiation were 17.6 (15 SD), 29.7 (30 SD), and 32.4 (16 SD) years, respectively. Most respondents were diagnosed between 0 and 5 years after their first symptoms (47%). Many of these respondents began medication within the same year as diagnosis (56%), though 24% started treatment between 1 and 5 years after diagnosis, and 19% of respondents started treatment longer than 5 years after diagnosis.
Table 1 Demographic characteristics of study populationWith regards to current treatment type, the majority of patients reported the use of long-term prophylaxis (LTP) plus on-demand (85%), and the remaining patients used on-demand only (15%). LTP therapy was taken by 89% of HAE-1 patients, 76% of HAE-2 patients, 80% of HAE nC1-INH, and 90% of patients uncertain of HAE type. Most respondents used subcutaneous pdC1inh for routine prophylaxis (49%). For on-demand treatment, the majority of respondents used intravenous pdC1inh (63%).
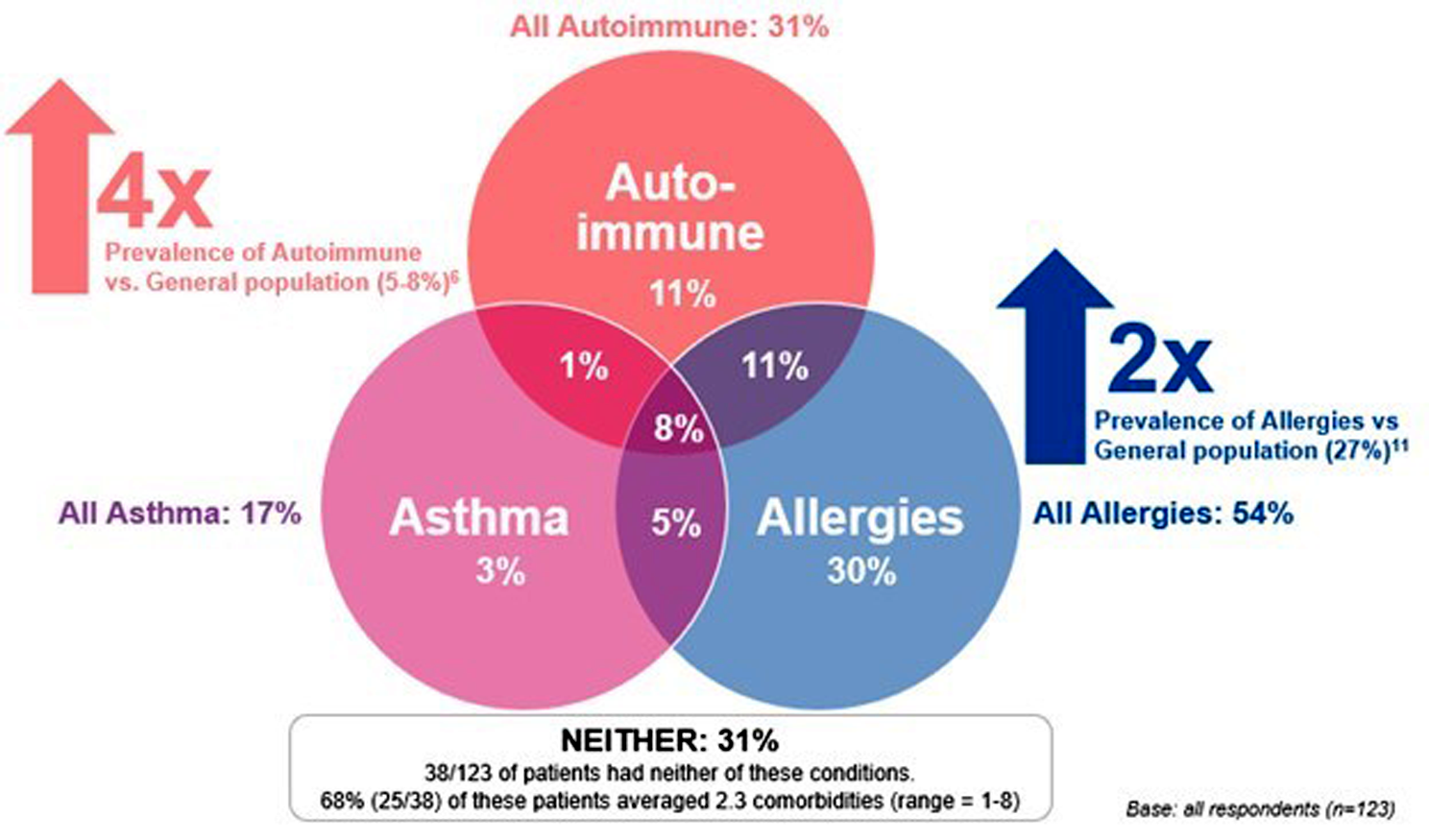
ComorbiditiesOverall, when grouped by International Classification of Diseases (ICD) class, the most common comorbidities reported were related to the respiratory system (e.g., allergies/asthma) at 39%, the immune system at 38%, and neurological systems (e.g., anxiety and depression) at 37%. HAE patients (69%) had at least one of the following conditions: autoimmune, asthma, and allergy. Autoimmune conditions were reported by 31% of patients, while 54% of patients reported allergies, and 17% of patients reported asthma. There is also overlap between these three conditions, with 29% of respondents with autoimmune conditions also reporting asthma, 61% reporting allergies, and 44% of allergy sufferers also reporting an autoimmune condition and/or asthma. 31% of patients did not report any of these three conditions (though they did report other comorbidities). Table 2; Fig. 1 illustrate the proportion of patients living with autoimmune, allergic, and asthma conditions and the proportion of patients living with only one, two, or all three of these conditions.
Table 2 Number of patients with autoimmune, allergies, and asthmaFig. 1
Overlap between autoimmune, allergies, and asthma
Patients reported living with 4.3 comorbidities on average, while some reported over 10 comorbid conditions. Patients most commonly had 1 comorbidity (19%), followed by 2 comorbidities (16%). Notably, 13% of patients had 10 + comorbidities. Figure 2 depicts the distribution of patients by number of comorbidities.
Fig. 2
Number of reported comorbidities per patient
The most frequently reported comorbidities in the survey were allergies (e.g., medication, pollen, and pets/dander), depression, and hypertension. When compared to the general population, allergies were reported by 54% percent of respondents compared to 27%[18] in the general population, depression was reported in 28% of HAE patients compared to 21–25% [19] in the general population, and hypertension was reported in 24% of HAE patients which is similar to the general population (23% [20]). Prevalence of reported cancers were either similar to the general population or significantly lower as in the case of prostate, breast and skin cancer.
Autoimmune diseaseApproximately one-third of respondents reported having diseases that are classified as autoimmune. This was significantly higher than the estimated prevalence in the overall population, approximately four times greater (31% versus 5–8%) [21]. This was supported by the higher observed occurrence of several autoimmune conditions, namely psoriasis (9% versus 3%), [22] RA (7% versus 1%), [23] inflammatory bowel disease (IBD) (4% versus 0.7%), [24] chronic urticaria (3% versus 0.5-1%), [25] lupus (2% versus 0.1%) [26] and psoriatic arthritis (2% versus 0.3%) [27, 28]. Prevalence of autoimmune conditions was similar between HAE-1, HAE-2, and HAE nC1-INHpatients, with non-statistical differences noted in thyroid disease (8% versus 3%), IBD (3% versus 7%), chronic urticaria (3% versus 7%), diabetes mellitus (1% versus 7%), and ankylosing spondylitis (0% versus 7%). In relation to gender differences in patient-reported autoimmune conditions, 34% of women in this study reported an autoimmune condition compared to 17% of men.
A higher prevalence of non-autoimmune comorbidities was reported by HAE patients in the survey with autoimmune conditions when compared to patients without autoimmune conditions. This difference was statistically significant with regards to hypertension (40% vs. 18%), sleeping disorder (40% vs. 11%), asthma (32% vs. 11%), irritable bowel syndrome (IBS) (29% vs. 9%), migraines/cluster headaches (32% vs. 7%), and arthritis (26% vs. 7%) (Table 3).
Table 3 Differences in comorbidities reported between respondents with and without autoimmune conditionsPatients with autoimmune conditions were found to have a less positive overall health status. Respondents without autoimmune conditions were more likely to have a very good to excellent state of health (53%), whereas only 18% of those with an autoimmune condition similarly reported having very good to excellent state of health. Respondents with an autoimmune condition were more likely to report being overweight compared to those without an autoimmune condition: obese (8% vs. 1%), overweight (50% vs. 39%), normal/healthy weight (40% vs. 57%). 32% of patients with autoimmune conditions reported having mobility issues, which is much higher than patients without autoimmune conditions (12%).
Allergies and asthmaOverall, the numbers for patient-reported allergies are two times higher than that of the general population (54% vs. 27%18). Allergies were classified as allergies to medication (55% vs. 28%18), pollens (55% vs. 41%18) and pets/dander (44% vs. 29%18). The occurrence of these three allergies is significantly higher than that observed in the general population and were more commonly reported in patients with an autoimmune condition and among patients with HAE nC1-INH.
HAE patients reported a higher rate of asthma in the survey. Asthma was reported by 17% of respondents, which is significantly higher than the general population (8–11%) [29].
HAE treatment initiation and evolution of comorbiditiesIn most cases, except for endocrine, nutritional, or metabolic conditions, patients were diagnosed with a comorbidity before their HAE diagnosis. The level of control of comorbidities varied by patient and by disease. For example, thyroid disease was reported as the most controlled and IBD was reported as the least controlled (Fig. 3). Overall, 27% of patients have seen an improvement in their given comorbidity since starting on HAE treatment, while 17% reported a worsening of their condition. Also, 63% of patients reported their current comorbidity condition as well to very well controlled, while only 16% of respondents reported poor to very poor controlled conditions.
Fig. 3
Current status and level of control of comorbidities varies by disease
In particular, patients on C1-INH prophylaxis therapy (subcutaneous or intravenous pdC1inh) reported their comorbidity being better controlled compared to those on other prophylaxis treatments (lanadelumab, danazol, tranexamic acid, icatibant, and other). On a scale of 1 to 5 (1 being very poorly controlled and 5 being very well controlled), mean scores were significantly higher among patients currently on pdC1-INH compared to those on other HAE prophylaxis treatments (3.7 vs. 3.1). Patients with HAE-1 (3.8) and HAE nC1-INH (3.8) reported their comorbidity being better controlled compared to those with HAE-2 (3.6) or those who were unsure of their HAE type (2.9) (Figs. 4 and 5).
Fig. 4
Current status of comorbidity by HAE prophylaxis taken. *Note: Low base. **Mean scores were significantly higher among patients currently on C1-INH compared to those on other HAE prophylaxis treatments (3.7 vs. 3.1). ***The study was not designed nor powered to detect a link between C1-inh and comorbidities. Other Prophylaxis treatments include: lanadelumab, danazol, tranexamic acid, icatibant, and other prophylaxis treatments
Fig. 5
Current status of comorbidity by HAE Type. *Note: low base. **Mean scores were significantly higher among patients HAE-1 & HAE nC1-INH compared to those unsure of their HAE type. ***The study was not designed nor powered to detect a link between C1-inh and comorbidities
Family history and predisposition to comorbiditiesPatients also reported a family predisposition, with 45% of patients reporting a shared comorbidity with a family member, which is as high as 53% of HAE nC1-INH patients (most of these family members being a first degree relative, namely the mother). One third (30%) of these family members also have been diagnosed with HAE. This is as high as 40% of HAE nC1-INH patients that also have a relative with HAE.
Hospitalization history due to comorbiditiesVery few patients reported an unplanned emergency room (ER) visit or hospital stay due to their comorbidity in the previous 24 months. Only 12 reported unplanned ER visit or hospital stay for RA, arthritis, IBD, migraines, asthma, restless legs syndrome, and fibromyalgia (each represented by 1 respondent, requiring 1 to 2 ER visits). Some conditions required numerous ER visits and at least 1 hospitalization (represented by 1 patient each): allergies, chronic pancreatitis, mast cell activation syndrome, and eosinophilic asthma.
Comments (0)