
Remember me






Anemia is a condition that develops when hemoglobin concentration in the blood is two standard deviations below the mean for the person’s age [1]. It affects close to half a billion women between the ages of 15 and 49, with a global prevalence of 29.6% among non-pregnant women of reproductive age and 36.5% among pregnant women [2]. Anemia results in poor cognitive and motor development in children, and it also affects their language skills [3, 4]. In adults, it reduces work capacity, enhances risks during pregnancy, and can lead to preterm births [2].
India has the world’s fifth highest prevalence of anemia among women of reproductive age [2] and is primarily caused by deficiencies in micronutrients, such as iron and Vitamin B12 [5, 6]. Latest data from the National Family Health Survey (NFHS-5) show that the prevalence of anemia in India has worsened since the last national survey, now standing at 57% among women of reproductive age. In the state of Odisha, prevalence is higher than the national average, at 64.3% [7]. The Government of India has spent significant resources to reduce anemia, including: promoting and distributing iron folic acid for free for pregnant and lactating women since 1970 [8]; running the Adolescent Girls Anemia Control Program that provides free supplements through the school system [9]; adopting a lifecycle approach under the National Iron Plus Initiative; and implementing the Intensified National Iron Plus Initiative (“Anemia Mukt Bharat”) since 2018 [10].
A key feature of these efforts has been the almost exclusive focus on supply-side issues, to ensure the health system is adequately prepared to acquire and distribute medications. Largely missing has been a concomitant demand-side focus to ensure that facilitators of and barriers to consumption of iron and adherence to medical guidelines are properly understood and addressed [10]. Focusing on iron-deficient anemia, with consumption of iron folic acid as the underlying outcome behavior, we ask whether a focus on social norms can serve as a theoretically informed entry point to improve behaviors and ensure their sustainability.
The study of the relationship between social norms and behaviors has a long scholarly history in a variety of disciplines [11, 12], but the conceptualization of social norms itself has tended to vary. In early social psychology research, Sherif [13] conceptualized the role of social norms as setting the social frame of reference against which one’s own judgment could be compared and contextualized, which is a perspective adopted by other influential researchers [14, 15, 16]. Sharper distinctions have emerged since those early days, with two types of norms – descriptive norms (to refer to people’s perceptions about others’ behaviors) and injunctive norms (to refer to pressures people feel to conform) [17]. Despite this focal distinction, a common thread in prevailing definitions of norms had been limited it to the realm of perceptions. Descriptive and injunctive norms all pertain to how people perceive the environment around them; it is these perceptions that, in turn, drive the underlying behavior.
Two limitations are worth noting in this conceptualization of norms. First, researchers have documented the mismatch that exists between actual behaviors and their perceived prevalence for a variety of topics – including alcohol consumption among college students [18], dietary behaviors [19], gender relationships [20], and tax compliance [21], to name a few. Perceptions need not be accurate and, indeed, research on the false consensus effect [22] and pluralistic ignorance [23] has demonstrated that they seldom are, and that media depictions further exacerbate this inaccuracy by disproportionately depicting aberrant behaviors because of their newsworthiness [24]. Interventions to change behaviors by correcting these misperceptions show mixed results [25, 26, 27, 28, 29].
The second limitation of relying solely on perceptions is that this approach neglects other important aspects of social norms, such as normative volume (the size of the prevalence and its acceptability) and normative subscription (the extent to which people endorse and internalize the norm as a behavioral guide) [24]. Lapinski and Rimal [30] proposed the idea of collective norms to refer to the actual prevalence of behavior and urged scholars to incorporate this concept in their theorizing [31]. In this extension, social norms are consequential in driving behaviors not only because of how people perceive those norms but also because the objective distribution of behaviors matters, regardless of how accurately they are perceived. The underlying mechanism here is less clearly understood, but one notion is that, when a behavior is highly prevalent, factors that guide its prevalence at the collective level also likely guide the behavior at the individual level.
The relationship between collective norms and individual behaviors is likely due to other factors that are not measured [30]. This idea of collective norms has since been incorporated in the extended theory of normative social behavior (TNSB) [11], which discusses the interactions across the three norms – descriptive norms, injunctive norms, and collective norms – to propose how they jointly affect behaviors [32]. This idea has taken hold in a number of studies [33, 34, 35], but the underlying causal mechanism has yet to be tested more rigorously.
In this paper, we test the causal linkages between the three normative factors, on the one hand, with iron folic acid supplement consumption, on the other. We do so in the context of a field experiment, specifically designed and implemented based on the TNSB [36]. The three innovative aspects of the work are that we (a) manipulate norms through an experimental design, (b) include collective norms as one of the normative factors that extend beyond perceptions, and (c) collect data longitudinally over the course of 18 months to test whether changes in norms from Time 1 to Time 2 drive behaviors at Time 3.
HypothesesThe relationship between social norms and behaviors has been tested through observational studies [37, 38], as revealed by a recent review [39]. These studies are important in understanding the underlying relationships, but they do not lend themselves to establishing causal linkages. Longitudinal studies can do so, and a number of them have been used to predict behaviors from norms over time [40, 41]. They do not, however, account for extraneous variables that confound, mediate, or moderate the relationships in complex ways.
To control for these factors, randomized studies are more robust, and findings reveal that norms are manipulable, and that they have a quantifiable impact on attitudes and behaviors, as revealed by a recent meta-analysis that included 110 articles in which norms were manipulated [42]. The fact that so many studies have manipulated social norms is, indeed, demonstrative of tremendous progress in the scholarship on social norms. However questions about the durability of norms-induced behavioral outcomes can also be addressed going beyond short-term changes in a laboratory setting, as pointed out by scholars [43]. We answer that call in this paper by manipulating norms in a field experiment and assessing their impact on iron folic acid consumption over 18 months.
We draw on the three social norms constructs (descriptive, injunctive, and collective norms), hypothesizing that the intervention resulted in improvements in each of these norms from Time 1 to six months later at Time 2. Second, we expect that changes in norms from Time 1 to Time 2 to predict iron folic acid consumption (behavioral outcomes) at Time 3 (a year after Time 2), after controlling for the Time 1 consumption behavior. Third, we also expect that, overall, there were significant improvements in behaviors after the intervention. Hence, our hypotheses are:
H1: From Time 1 to Time 2, improvements in descriptive norms (H1a), injunctive norms (H1b), and collective norms (H1c) will be greater in treatment than in control communities.
H2: Improvements in descriptive (H2a), injunctive (H2b), and collective (H2c) norms from Time 1 to Time 2 will predict iron folic acid consumption at Time 3, after controlling for the behavior at Time 1.
MethodsData for this study come from the Reduction in Anemia through Normative Innovations (RANI) Project, a field experiment run in the state of Odisha in eastern India over an 18-month period [44]. The primary aim of the study was to determine whether a social norms-based intervention could reduce anemia among women of reproductive age by promoting the consumption of iron folic acid tablets according to the World Health Organization guidelines (once per week for nonpregnant women and daily for pregnant women). Informed by the TNSB [36], the intervention itself was developed based on findings from a six-month long, mixed methods formative evaluation which included 16 focus groups and 21 individual interviews with stakeholders [45] which sought to understand the role that gender and other aspects of self-identity played in women’s decisions to take iron supplements, and the extent to which their mothers-in-law, husbands, and other community members could be mobilized to facilitate women’s iron consumption.
Development of the RANI interventionA key finding from the qualitative formative assessment [10, 46] was that the drivers of taking iron folic acid tablets resided at multiple levels in the socioecological continuum. Apart from individual level factors, such as perceived side effects and low risk perceptions, drivers of the behaviors were also manifest at the interpersonal (how husbands and other influential people perceived the importance of anemia), structural (having access to the tablets), and cultural (the importance of prioritizing the health of women in the community) levels.
An outcome from this work was the tentative affirmation of the team’s idea that a social norms-based approach was probably an effective strategy for a longer-term behavior change approach. Over a week-long participatory workshop, this proposed approach was then shared with stakeholders, which included members from the local Panchayat (political leadership), leaders from women’s self-help groups (which have a long-standing engagement in the community), frontline healthcare workers (in Odisha, they are the Aganwadi workers, accredited social health activists [also called ASHAs], and auxiliary nurse midwives [also called ANMs]), community residents themselves, and members of nongovernmental organizations engaged in nutrition activities in the state. During the workshop, we shared our findings from the formative assessment, discussed the role of social norms, and collectively co-designed and subsequently refined a few social norms-based approaches.
Because the key elements of the RANI intervention are published elsewhere [47], we do not describe them again here, except to note that activities were specifically designed to change: descriptive norms (by highlighting the fact that more and more women of reproductive age were now consuming iron folic acid as part of a healthy behavior); injunctive norms (by enlisting the support of husbands, mothers-in-law, community leaders, and the health system to facilitate, prioritize, and promote the distribution of iron folic acid for free to all women of reproductive age in the community); and collective norms (by displaying in community centers and other prominent locations the increasing hemoglobin levels, which are measures of improvements in anemia, in the community through graphically-based results).
To promote social and behavior change, we engaged the community in participatory learning modules through hands-on activities [47, 48], and we also developed and disseminated six videos that provided education about the link between iron and anemia and role modeled people who were supporting women in their consumption of iron supplements. The videos targeted our focal populations (adolescent girls and married women of reproductive age) as well as other influential people in their social networks, including husbands, mothers-in-law, and community members. The underlying idea, based on the TNSB, was that the appeal to change needed to be made to both parties – the target audiences themselves and their social network members. This is what sets apart a social norms-based intervention from an individual-focused intervention. Whereas an individual-focused intervention makes the case for change directly to the target audience, a social norms-based intervention also includes an appeal that is made to influential others, whose opinions would be consequential in the target audience members’ decisions about whether to enact the recommended behavior. For these reasons, we showed the videos not only to the target audience (for whom the specific video was produced) but also to their influential parties – so that our target audience members would know that others had seen the video and that those others were also expected to support the target audience members in their decisions to consume iron supplements. These videos were shown in small groups, and they were also screened publicly for residents during community events.
Study designThe evaluation design consisted of a three-wave longitudinal cluster randomized trial in which we collected data from the same women at baseline (Time 1) in September 2019, six months later at midline (Time 2) in February 2020, and a year after that at end-line (Time 3) in August 2020. At each wave, we conducted one-on-one interviews (approximately an hour in duration), obtained women’s height and weight measurements, and assessed psychosocial variables. The same procedures were adopted in both treatment and control communities.
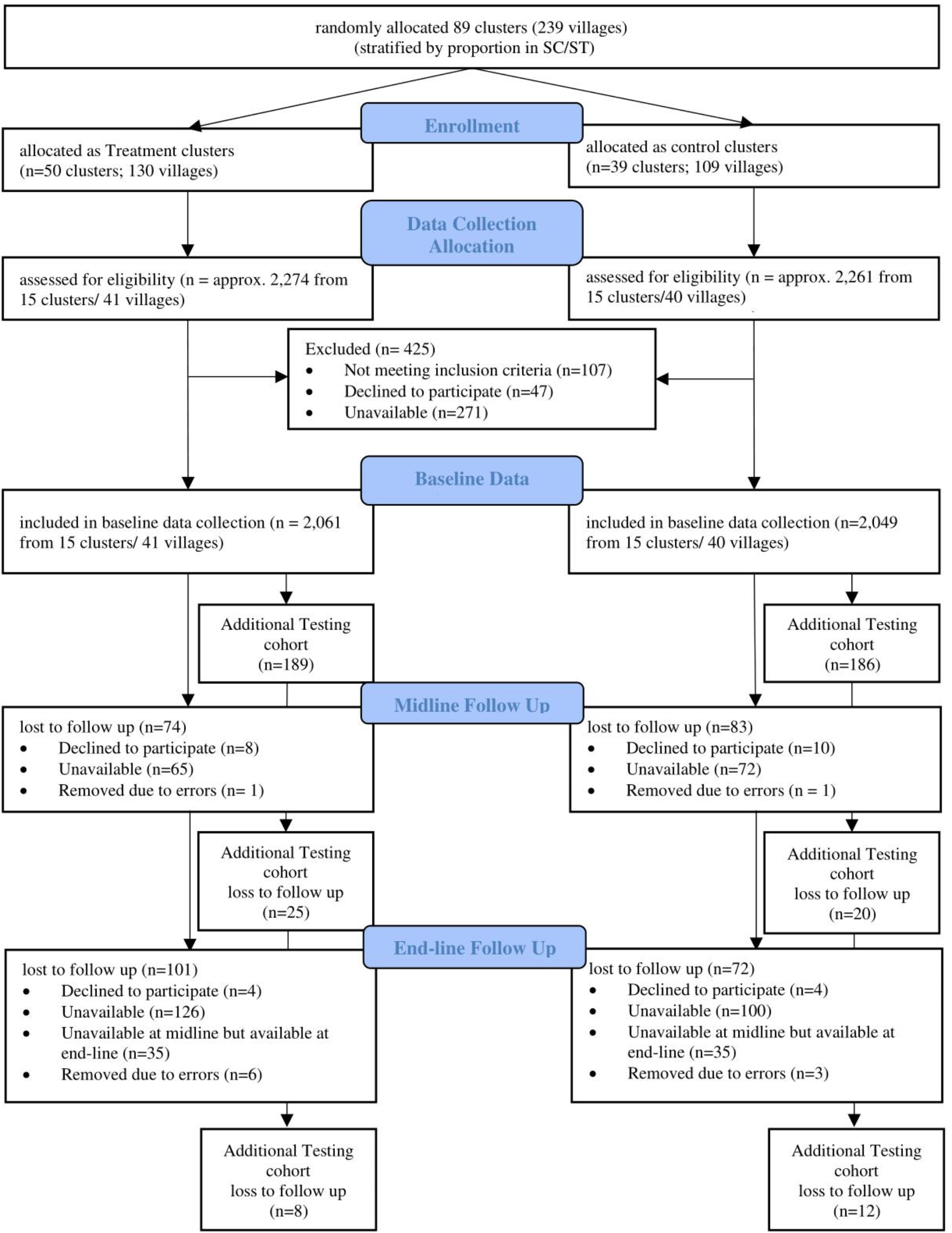
Randomization into treatment and control communities was done in three stages (Fig. 1). First, all villages in our study area (k = 239) were formed into 89 clusters, with each cluster including two to four geographically contiguous villages. Second, all adjacent clusters were excluded from sampling in order to minimize contamination. Third, all remaining clusters (which now had a buffer of at least one or more contiguous clusters) were randomly assigned to either the treatment (50 clusters that comprised 130 villages) or the control (39 clusters with 109 villages) arm.
Fig. 1
Flow chart of the RANI project
Within each cluster, villages were stratified by their concentration of tribal populations (to ensure we captured a sufficient number in our study) and then homes were sampled in proportion to population size. In each selected home, we invited one woman of reproductive age to participate in the study (randomly selecting from a list if more than one eligible woman resided in the home). Women were considered eligible if they were between 15 and 49 years old, a resident of the village in Odisha, spoke Odiya, and did not have a plan to move out of the village for the next two years.
Baseline data were collected from all participants before the start of the intervention. In the control arm, we only collected the three waves of data, without any intervention activities. In the treatment arm, the same procedures were adopted for data collection, with the intervention being rolled out immediately after the baseline data collection was completed. At baseline, interviewers were blinded about the treatment or control status of the village from which participants were recruited; although the treatment/control status was never revealed to data collectors, it is likely that they came to learn about the status after conducting a few interviews at midline. On the research team, only the statistician knew the treatment or control status of any given participant; the principal investigator and others were shielded from this information through a password-protected file.
Informed consent was obtained by data collectors before beginning the interview. Participants signed a form to indicate their consent. Ethics approvals were obtained from the Institutional Review Board at George Washington University in Washington DC, USA (FWA00005945), the Institutional Review Board at Sigma Science and Research in New Delhi, India (10031/IRB/D/18–19 for baseline 10059/IRB.19–20 for midline, and 10036/IRB20-21 for end-line), and from the India Council for Medical Research (ICMR)’s Health Ministry Screening Committee (HMSC) (2018 − 0921/F1).
MeasurementAll variables used in this study were obtained through one-on-one interviews conducted by Oriya-speaking women interviewers who had received a weeklong human subjects and interviewing training.
Demographic measuresWe measured age in years, education as the number of years spent in school, tribal status as whether the participant belonged to one of the tribes recognized by the government, whether the participant was pregnant at the time of data collection, and the number of children she had.
Descriptive normsInformed by the TNSB [36], we assessed descriptive norms as the average of three questions that asked participants to estimate what proportion of women in their communities took iron folic acid tablets. Responses, measured on five-point scales (from 0 to 4) were averaged into an index α = 0.45 at baseline and α = 0.63.
Injunctive normsFollowing the TNSB [36], we assessed injunctive norms through six questions by asking participants how many others in their social network (including other women in their community, their mother-in-law, husband) thought the participant should take iron folic acid. Responses, coded on five-point scales (from 0 to 4) were averaged into an index, α = 0.71, α = 0.77 at midline.
Collective normsFollowing the method proposed by Sedlander and Rimal [49], we assessed collective norms as the “non-self mean”–by calculating the total iron folic acid consumption in the village (based on everyone from the village in our sample), subtracting out the consumption level of the participant, and then dividing this difference by the total number of women from the village in the sample, minus one. Numerically, the collective norm measure is:
$$\:collective\:norms=\:\frac^\left(IFA\right)\right]-\left(_\right)}$$
where k = number of participants in the given village in our data set and IFA = whether each person reported consuming iron folic acid (coded as 1) or not (coded as 0).
Iron folic acid consumption was asked through a single item, whether the participant had ever taken iron folic acid in the past, with three response options: never taken in the past, taken in the past but not taking now, and taking now. The last option was coded as 1 and the first two options (never consumed or only prior consumed) was coded as 0.
Change scoresChange scores in the three (descriptive, injunctive, and collective) norms were calculated by subtracting baseline values from the corresponding end-line values of the norms.
Statistical testsDue to the nested nature of the data, we used hierarchical linear models whenever appropriate; in longitudinal comparisons, individuals were treated as Level 2 and clusters as Level 3 in mixed effects regressions.
Ethical considerationsThis trial is registered with the Clinical Trial Registry of India (CTRI/2018/10/016186).
Comments (0)