
Remember me


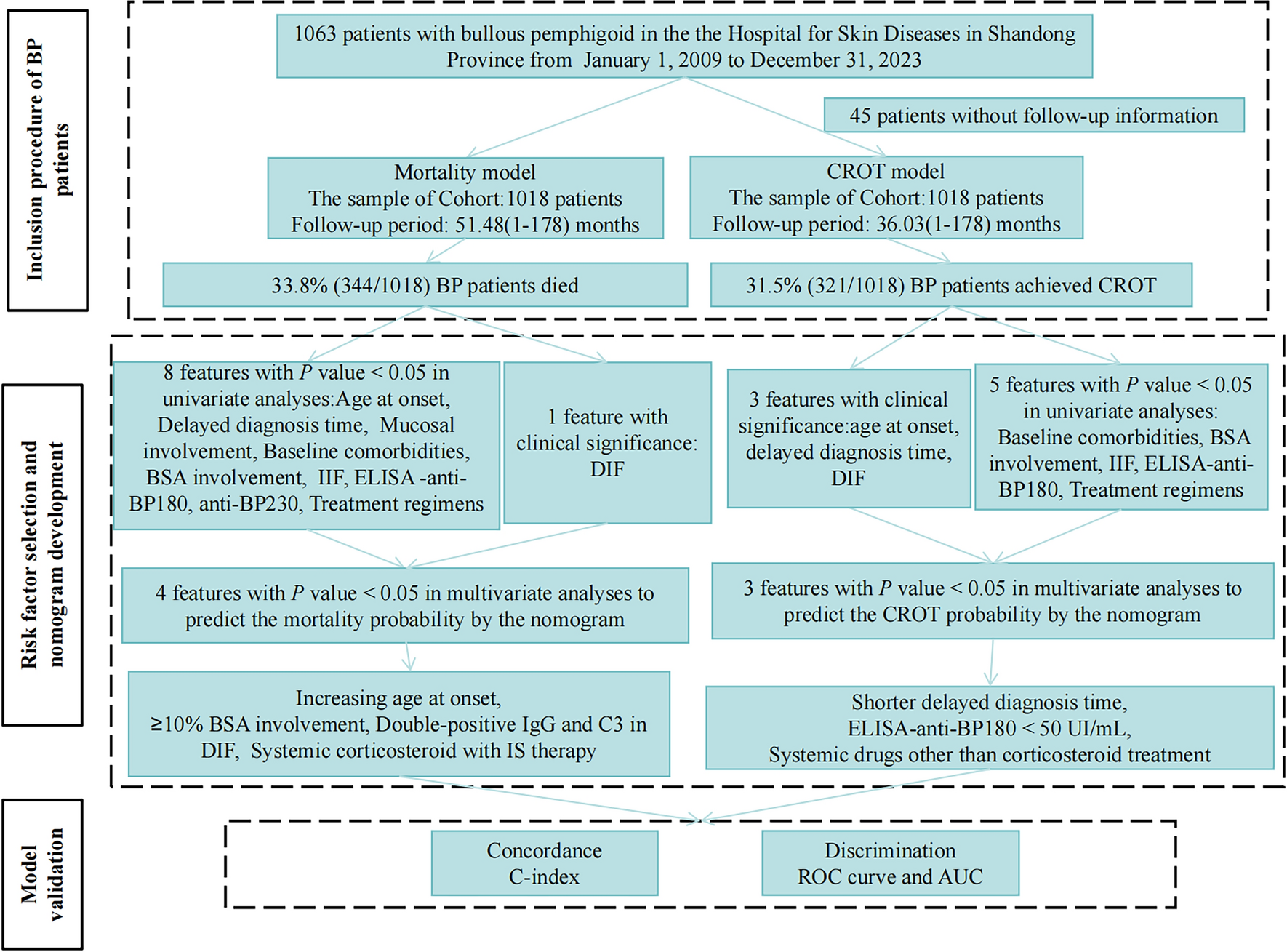
Of the 1063 BP patient, 45 were excluded due to loss to follow-up. Consequently, the study cohort comprised 1018 BP patients, consisting of 589 (57.9%) males and 429 (42.1%) females, all of Chinese nationality. The mean age at BP onset was 69.7 years. The mean delay from onset of skin symptoms to diagnosis was 7.3 months. Comorbidities were present in 821 (80.6%) patients, with hypertension being the most common (496, 48.7%), followed by neurological diseases (175, 17.2%). Regarding disease severity, 462 (45.4%), 223 (21.9%), and 333 (32.7%) patients had mild BSA involvement (<10%), moderate BSA involvement (10–30%), and severe BSA involvement (> 30%), respectively. Mucosal involvement was observed in 260 (25.5%) patients with BP.
All patients tested positive for IgG and/or C3 antibodies by DIF. Of these, 35.6% showed double positivity for IgG and C3, while 64.4% showed single positivity. Additionally, IgM positivity was observed in only 23.8% of patients, double positivity for IgM and IgA in 5.1%, and positive IgA in only 1.0%, with the remaining 70.1% negative for IgM and IgA. A total of 78.2% (577/738) patients were IgG-positive by IIF with median IgG titers of 40.0 (0–2560.0). Additionally, 77.4% (652/842) patients were positive by anti-BP180 antibody and 37.3% (314/842) patients were positive by anti-BP230 antibody; the median anti-BP180 antibody and anti-BP230 antibody were 191.8 (0–246.0) and 2.0 (0–209.9). Therapeutic regimens included systemic corticosteroid with IS treatments (492, 48.3%), systemic corticosteroid monotherapy (335, 32.9%), and systemic drugs other than corticosteroid therapy (191, 18.8%). The IS medications consisted of cyclophosphamide (372, 75.6%), mycophenolate mofetil (83, 16.9%), methotrexate (26, 5.3%), cyclosporine (6, 1.2%), and azathioprine (5, 1.0%). Further details of clinical characteristics at baseline are provided in Table 1.
Table 1 Baseline demographics and clinical characteristics of 1018 patients with bullous pemphigoid3.2 Mortality AnalysisWith a median (range) follow-up period of 51.48 (1–178) months, 344 (33.8%) patients with BP had passed away and 674 (66.2%) had survived. The 1-, 3-, and 5-year mortality rates were 22.8%, 31.2%, and 34.5%, respectively (Fig. 2a). Of the patients who died, 123 (35.8%) died of known diseases including cardiovascular diseases (43, 35.0%), neurological diseases (32, 26.0%), COVID-19 infection (19, 15.4%), cancer (15, 12.2%), renal failure (13, 10.6%), and accidents (1, 0.8%). Among 32 patients who died of neurological diseases, including stroke (27 cases), cerebral hemorrhage (4 cases), and Parkinson’s disease (1 case). Among the three treatment groups, mortality rates were highest in the systemic drugs other than corticosteroid group (40.8%), followed by the systemic corticosteroid group (34.6%) and the systemic corticosteroid combined with IS therapy group (30.5%) (Supplementary Table S1).
Fig. 2
Mortality outcome and prediction of bullous pemphigoid (BP): a Survival probability of BP; b Receiver operating characteristic curve with survival prediction model in the 1 year (blue), 3 years (green) and 5 years (orange); c The nomogram of mortality prediction
After both the univariate and multivariate Cox regression analyses, we identified three significant factors increasing mortality with increasing age at onset (HR = 1.08; 95%CI 1.06–1.10; p < 0.0001), > 10% BSA involvement (10–30%, HR = 7.19; 95%CI 4.35–11.86; p < 0.0001; > 30%, HR = 9.84; 95%CI 6.30–15.40; p < 0.0001), and double-positive for IgG and C3 antibodies on DIF (HR = 1.37; 95%CI 1.0–1.87; p = 0.049). Notably, systemic corticosteroid in combination with IS treatments (HR = 0.50; 95%CI 0.33–0.75; p = 0.00080) significantly decreased the risk of mortality compared to systemic drugs other than corticosteroid group (Table 2).
Table 2 Multivariate Cox regression analyses of mortality factors with bullous pemphigoidA predictive model for mortality was formulated, utilizing these significant risk factors, including age at onset, BSA involvement, positive antibodies on DIF, and treatment regimens. This model demonstrates excellent predictive abilities for 1-, 3-, and 5-year mortality rates, with AUC values (0.83, 0.86, and 0.88, respectively) (Fig. 2b). The C-index of survival predictive model is 0.81 ± 0.01. For further validation, the results of a 5-fold cross-validation, including AUC and C-index, were described in Supplementary Table S2.
Furthermore, incorporating these aforementioned significant indicators, we have constructed a nomogram to simplify the practical application of mortality prediction (Fig. 2c). For instance, consider a 70-year-old patient with BP, BSA involvement exceeding 20%, and both IgG and C3 positive on DIF. According to the nomogram, this patient's total score would be 95 points (70 points for age, 22.5 points for BSA involvement, and 2.5 points for both IgG and C3 positivity on DIF. Based on this score, the predicted one-year mortality rate with a treatment regimen of systemic corticosteroid combined with IS would be 25%, with a projected mortality rate of 45% by the fifth year. In comparison, if the patient receives systemic drugs other than corticosteroid therapy, the one-year mortality rate rises significantly to 45%, with a long-term mortality rate of 70%. Conversely, with systemic corticosteroid monotherapy, the one-year mortality rate is 35%, and the long-term mortality rate is 55%.
3.3 Complete Remission Off-Therapy AnalysisA total of 321 (31.5%) achieved CROT and 697 (68.5%) patients were non-CROT. The cumulative rates of CROT at 1, 3, and 5 years were 10.9%, 32.9%, and 47.5%, respectively (Fig. 3a). The median time to achieve CROT was 66.0 months. Among non-CROT patients, 233 (22.9%) achieved complete remission on minimal therapy, 380 (37.3%) achieved partial remission on minimal therapy, and 84 (8.3%) achieved partial remission off therapy. Among three treatment groups, the percentages of patients achieving CROT were 39.8% (systemic drugs other than corticosteroid treatment group), 31.7% (systemic corticosteroid combined with IS therapy group), and 26.6% (systemic corticosteroid treatment group) in the Supplementary Table S1, respectively.
Fig. 3
Complete remission off-therapy regression (CROT) and prediction of bullous pemphigoid (BP): a CROT probability of BP; b Receiver operating characteristic curve with CROT prediction model in 1 year (blue), 3 years (green) and 5 years (orange); c The nomogram of CROT prediction
Through univariate and multivariate Cox regression analyses, patients with a shorter diagnosis delay time, baseline anti-BP180 antibody (< 50 IU/mL) and systemic drugs other than corticosteroid treatment had a 1.01-fold (HR = 1.01; 95%CI 1.0–1.03; p = 0.0069), a 1.48-fold (HR = 1.48; 95%CI 1.06–2.07; p = 0.020), and a 1.68-fold (HR = 1.68; 95%CI 1.12–2.52; p = 0.013) chance of achieving CROT (Table 3). This model demonstrates medium predictive abilities for 1-, 3-, and 5-year CROT rates, achieving AUC values of 0.67, 0.62, and 0.63, respectively (Fig. 3b). The C-index of CROT predictive model was 0.65 ± 0.02. The 5-fold cross-validation’s AUC and C-index were described in Supplementary Table S3.
Table 3 Multivariate Cox regression analyses of complete remission off-therapy factors associated with patients of bullous pemphigoidA CROT predictive model was depicted as a nomogram for practical application with these aforementioned significant indicators, including diagnosis delay time, baseline anti-BP180 antibody, and treatment regimens (Fig. 3c). For example, consider a 65-year-old BP patient with a diagnosis delay of less than 20 months and an anti-BP180 antibody level of 100 IU/mL (> 50 IU/mL). According to the nomogram, this patient's total score would be 85 points (85 points for diagnosis delay and 0 point for anti-BP180 antibody levels). Based on this score, the predicted one-year CROT rate with a treatment regimen of systemic drugs other than corticosteroid is over 10%, with a projected CROT rate over 55% by the fifth year. In contrast, if the patient receives systemic corticosteroid combined with IS therapy, the one-year CROT rate is less than 10%, with a long-term CROT rate of 40%. With corticosteroid monotherapy, the one-year CROT rate is less than 10%, and the long-term CROT rate is less than 40%.
3.4 Relapse AnalysisRemarkably, a total of 749 (73.6%) patients had experienced relapses, including 233 (31.1%) patients after achieving CROT and 516 (68.9%) during non-CROT, with cumulative rates at 1-, 3-, and 5-years of 21.9%, 46.6%, and 60.9%, respectively. Most relapses were attributed to patients adjusting their medication themselves (606, 80.9%). The remaining factors of relapses were linked to exhaustion (65, 8.7%), trauma (3, 0.4%), and other unspecified causes (75, 10.0%).
Patients with baseline comorbidities, ≥10% BSA involvement, and higher anti-BP180 antibody level had a 1.81-fold (relative risk [RR], 1.81; 95%CI 1.09–2.96; p = 0.020), 4.83-fold (10–30% BSA, RR, 4.83; 95%CI 2.17–12.90; p = 0.00042), 2.51-fold (> 30% BSA, RR, 2.51; 95%CI 1.45–4.55; p = 0.0015), and 1.006-fold (RR, 1.006; 95%CI 1.003–1.009; p < 0.0001) higher likelihood of occurring a clinical relapse, as detailed in Supplementary Table S4.
3.5 Side EffectsIn our cohort, 573 (56.3%) experienced side effects which need to be treated. The most common side effects were hypertension (207, 36.1%), hyperlipidemia (204, 35.6%), elevated blood glucose (183, 31.9%), leukopenia (150, 26.2%) and neutropenia (143, 25.0%). A particularly concerning side effect was severe femoral head avascular bone necrosis, which was found in 13.3% of BP patients.
Comments (0)