
Remember me



Three participants were referred to an outpatient clinic that specialized in the assessment and treatment of dangerous behavior. The caregivers scheduled two to three 1-hr visits per week and all services (from intake to discharge) were completed within approximately three months for all participants. The session rooms were approximately 3 m by 3 m. Each room had a padded play area where the child had access to preferred items. The rooms also had a table and two chairs to complete tasks or academic work. Each room was equipped with a camera that was live-streamed during each phase of the PFA and SBT, and caregivers could view the livestream from the waiting room. We attempted to include the family in the decision-making process by encouraging them to ask questions and provide feedback while watching every session live throughout the process. The door of the therapy room was always left open during each phase of the PFA and SBT, allowing the child to leave and go to the clinic waiting room with their caregivers at any time. This did not occur during any of the performance-based IISCAs.
RichFootnote 1 was a 9-year-old, European American boy diagnosed with ASD, attention-deficit/hyperactivity disorder, a language and speech disorder, and a learning disability. His vocal abilities included 1-word utterances. Rich was homeschooled due to the severity of his challenging behavior. Rich’s mother reported that when the doors of their home were closed, Rich would become visibly distressed and punch a hole through the doors. Doors remained open at all times in their home to decrease the chances of evoking dangerous behavior. In their everyday life, Rich’s mother had to remain by Rich’s side at all times because he would engage in challenging behavior if they separated. He engaged in dangerous behavior including aggression, disruptive behavior, and SIB, and associated nondangerous behavior including physical intimidation. His aggression involved using closed or open fists to hit others, SIB involved hitting his head with a closed fist, and property destruction involved tearing and throwing items. His physical intimidation involved raising a closed fist above his head and taking a step toward another person.
Troy was a 5-year-old, African American boy diagnosed with ASD. He communicated using brief, disfluent sentences. Troy’s mother reported that Troy would often exhibit extended tantrums that could last for hours. During these tantrums, Troy would elope to break or tear any items he could reach. If others were around him during an extended tantrum, he would aggress toward them; however, Troy would engage in SIB, by using his closed fist to hit his head, if no one was within arm’s reach. Troy’s mother reported that it was often difficult to manage his dangerous behavior and she was afraid for his safety as well as the safety of others around him, including his other young siblings.
Chung was a 4-year-old, Chinese American boy diagnosed with ASD. Although Chung could make some verbal approximations when vocally prompted, he did not exhibit any independent vocal communication skills. Caregivers reported his dangerous behavior as aggression, which involved scratching faces and pulling the hair of others. Caregivers reported his most difficult behavior to manage involved extended tantrums where he would begin to swipe or throw items and engage in SIB such as scratching himself while rolling on the floor screaming and crying. These extended tantrums would often cause him to have nosebleeds.
MeasurementDuring the participants’ first visit to the clinic, the caregivers were asked to complete questionnaires and a consent form to participate in research. The questionnaires included the Aberrant Behavior Checklist Second Edition (ABC-2; Aman & Singh, 2017) and the Parenting Stress Index Fourth Edition Short Form (PSI-4-SF; Abidin, 2012). These were administered to collect measurements and to include family members in the therapeutic process. The ABC-2 is a questionnaire that delineates between four subscales of challenging behavior. The clinician converted the raw scores from the completed ABC-2 forms into percentile rankings for youth with ASD (see p. 84 of ABC-2 manual). The PSI-4-SF categorizes parental stress into three domains: parental stress, parent–child dysfunctional interaction, and difficult child. The scores from each of the domains are summed to create a total stress value and create a percentile profile. Both questionnaires, the ABC-2 and the PSI-4-SF, were completed by caregivers during intake and again before discharge.
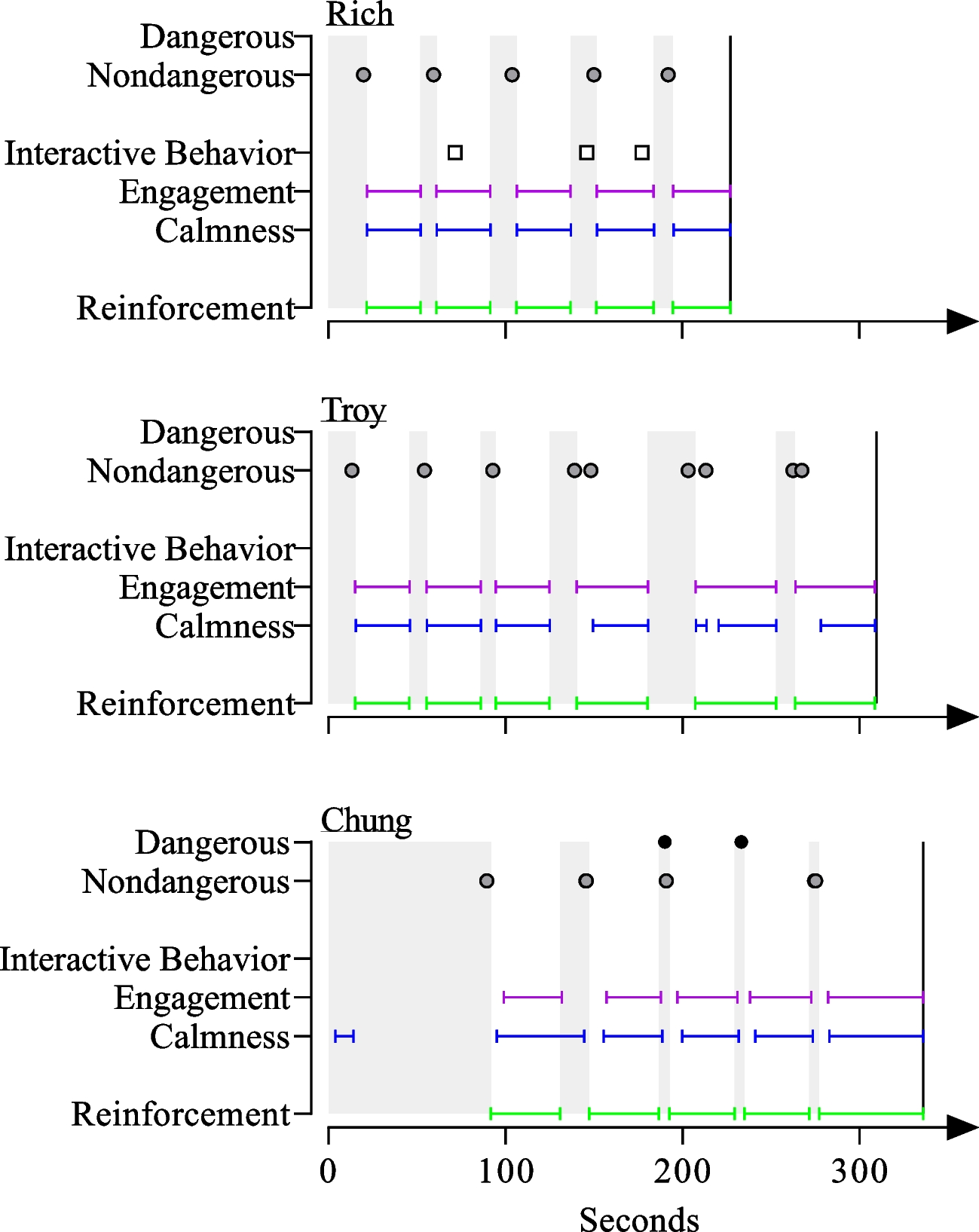
To ensure safety, we measured and targeted dangerous and nondangerous topographies of challenging behavior in an open-contingency class during the assessment and treatment process. Dangerous and associated nondangerous behavior were only included in the open-contingency class if they were reported by caregivers to be functionally similar (Warner et al., 2020). We considered dangerous behavior to be any topography that posed a serious risk or resulted in injury to oneself or others (e.g., SIB, aggression, property destruction). We considered any associated nondangerous behavior as any topography that did not result in injury to oneself or others (e.g., whining, crying, inappropriate vocalizations, physical intimidation). The performance-based IISCAs display the count of challenging behavior and distinguishes between dangerous and nondangerous behavior. All challenging behavior (dangerous or nondangerous) was aggregated into a single measure during the treatment evaluation and calculated as a rate by dividing the frequency by the session duration.
We measured two alternative behaviors, calmness and engagement, as durations during the performance-based IISCA. We also measured reinforcement as a duration, beginning with the termination of the establishing operation and the presentation of preferred items or events (i.e., synthesized reinforcement context). We converted the duration measures to a percentage of the session by dividing the duration of the behavior by the session time. Other alternative behaviors that were measured or targeted included interactive behavior, functional communication responses (FCRs), tolerance responses, and cooperation.
The count of interactive behavior was only included in the performance-based IISCAs. FCRs were measurements of the participants’ communication skills and we distinguished between simple FCRs, intermediary FCRs, and complex FCRs. The rate of communication and tolerance responses was reported by dividing the count of the FCR or tolerance response by the session duration.
We chose the instructions and tasks that targeted cooperation based on the participant’s developmental level and individual goals, which were co-developed with caregivers during the open-ended interview and throughout SBT. We reported cooperation as a percentage by dividing the number of tasks completed by the number of instructions given and multiplying the quotient by 100. A summary of dangerous behavior, nondangerous behavior, calmness, engagement, interactive behavior, and cooperation is presented in Table 1. The FCRs and tolerance responses for each participant are presented in Table 2.
Table 1 Summary of dependent variablesTable 2 Summary of functional communication and tolerance responsesInterobserver Agreement (IOA)A secondary observer collected interobserver agreement (IOA) on all of the participants’ performance-based IISCAs and at least 30% of the treatment evaluations. We calculated a partial interval agreement by dividing each session into 10-s intervals and dividing the smaller number of the data collected by the larger number and multiplying that average by 100 to obtain a percentage. We calculated IOA for all challenging behavior (nondangerous and dangerous), appropriate behavior (interactive behavior, calmness, engagement, FCRs, tolerance, and cooperation), and reinforcement. The mean IOA for all participants was above 90%. A summary of IOA for all participants is presented in Table 3.
Table 3 Interobserver agreement obtained during the performance-based IISCA and treatment evaluationExperimental DesignThe frequency of challenging behavior when the reinforcers were absent was compared to the frequency of challenging behavior when the reinforcers were present during the performance-based IISCA. Experimental control was demonstrated when instances of challenging behavior occurred more when the reinforcers were absent and the establishing operation was present. We conducted the SBT treatment validation using a multiple baseline across responses with a brief return to baseline following the first phase of FCT. Experimental control was demonstrated when challenging behavior increased during the return to baseline and was eliminated or decreased once FCT was reinstated. Functional control of FCRs was demonstrated with the elevated rates of the appropriate FCR during each phase.
ProceduresOpen-Ended InterviewThe PFA began with an open-ended interview conducted with the caregivers (see appendix of Hanley, 2012). The open-ended interview included questions about the (a) participants’ language abilities and preferences, (b) topographies of challenging behavior, and (c) context in which challenging behavior had occurred. The questions regarding language abilities were used to categorize the participants’ baseline abilities (i.e., nonspeaking, 1-word utterances, disfluent sentences, fluent sentences) and helped the clinician determine what simple communication to begin teaching once the treatment was introduced. The clinician used the questions regarding topographies of challenging behavior to identify an open-contingency class targeting a collection of responses the caregivers had experienced ranging from dangerous (e.g., aggression, property destruction, SIB) to precursors to dangerous behavior (e.g., screaming, whining, yelling, swearing). All the topographies described by the caregivers to be functionally related were then included within the open-contingency class. The remaining questions regarding the context in which challenging behavior occurred were most important for designing the performance-based IISCA. The clinician asked caregivers questions about any potential antecedents that were likely to evoke challenging behavior and consequences that were likely to de-escalate behavior. The answers from the caregivers helped the clinician develop a unique contingency representative of the context in which the caregivers were likely to experience challenging behavior in the home, school, or community. Developing a unique contingency based on the caregiver’s answers was important not only for ecological validity but also for following the trauma-informed guideline of including family and shared governance (Pollack et al., 2024). This unique contingency, including preferred and evocative events, was then evaluated in the performance-based IISCA.
The open-ended interview identified preferred and evocative events to be assessed during the performance-based IISCA for all participants. Rich’s preferred events included independent play with his phone and tablet. Interrupting this play with any sort of requests or instructions was identified as the evocative event. Troy preferred to play independently with a tablet and boxes of various alphabet letters. The evocative event included academic work completed at the table. The preferred events for Chung included interactive play with activities such as kinetic sand, marble towers, and dinosaurs. The evocative event included discrete trial instructions at the table.
The open-ended interview required approximately 15 min to conduct with each caregiver. During this time, the participant was provided with noncontingent access to preferred events and any reasonable requests were honored to build a healthy relationship between the participant and clinic assistant. The clinician brought the caregiver to a separate room and procedures were implemented to promote the participants’ comfort and safety. For Chung, the door of the interview room was left ajar so that he could see his caregivers and choose to leave and spend time with his caregiver at any point during the interview. To ensure safety, the clinician conducted the open-ended interview with both Rich and his mother in the same room to prevent distress that might be caused by separation from his mother. Troy displayed an initial discomfort leaving his father’s side; however, after a few min of playing with the clinic assistants, the father was able to leave the room for the open-ended interview and Troy continued to play with the clinic assistants without incident.
Performance-based, Interview-Informed Synthesized Contingency Analysis (IISCA)Prior to the performance-based IISCA, the clinician provided three min of noncontingent access to the preferred activities identified during the open-ended interview to build rapport and ensure the participant was comfortable before beginning the analysis. If challenging behavior consistently occurred during this time, the clinician would have discontinued the session and returned to open-ended questioning with the caregiver. This did not occur with any of the participants. The clinician initiated the performance-based IISCA as long as the participant was calm during the final 30 s of access to the preferred activities.
The performance-based IISCA began with the simultaneous removal of the preferred activities and the presentation of the individualized evocative events. This change in the environment often coincided with an instruction, such as, “Playtime is all finished, it is time to do some work.” The evocative events continued to progress if the participant cooperated with all instructions (i.e., instruction to stand up, then walk to the table, then begin completing work) until 10 min had elapsed. If no challenging behavior occurred within the 10 min, the performance-based IISCA would have been discontinued and the clinician would have asked the caregiver additional open-ended questions about other potential evocative events. This did not occur. The clinician reinstated access to all reinforcers immediately following the first instance of any nondangerous or dangerous challenging behavior. The clinician also provided a statement of support (e.g., “It is okay, we can play. Don’t worry.”). The preferred events were then available for 30 s after the onset of calm behavior. After 30 s of calm behavior, the evocative events were re-presented. Any challenging behavior or any indices the participant was not calm during access to the preferred events resulted in the 30-s timer being reset.
The performance-based IISCA was discontinued after 5–6 instances of challenging behavior corresponding to 5–6 evocative events. The criteria for ending the performance-based IISCA was the presentation of five consecutive establishing operations that successfully evoked challenging behavior and the de-escalation of behavior following the reinstatement of synthesized reinforcement. There was no set minimum duration and the clinician interpreted the results in real-time with a differentiated outcome indicated by challenging behavior reliably occurring during periods in which the evocative events were present and not occurring when the participant had access to the preferred events.
BaselineThe clinician began SBT once the performance-based IISCA empirically identified caregiver-informed evocative events that reliably evoked challenging behavior and preferred events that reliably de-escalated behavior. The baseline phase was similar to that of the performance-based IISCA in that the evocative events were presented and any challenging behavior resulted in the simultaneous removal of the evocative events and presentation of the preferred activities. Baseline sessions were 3 min.
Functional Communication Training (FCT)The first phase of SBT included FCT to teach increasingly complex responses (Ghaemmaghami et al., 2018). The complexity of responses increased from the simple FCR to the terminal FCR by adding to the response effort of the FCR through additional letters or words, social niceties (e.g., “Please”), and social interactions. The variables added to the complexity of responses were determined by the participant’s communication abilities and progression during FCT. The clinician selected a simple FCR that was at or below the baseline abilities identified during the open-ended interview. The intermediary FCR extended the sentence structure or added additional nonverbal response requirements (for those who were nonspeaking). The terminal complex FCR included conversational niceties along with an interaction with the clinician. For example, Troy’s complex FCR involved him first saying “Excuse me” in order to get the attention of the clinician. Once the clinician acknowledged Troy, his complex FCR continued with, “My way, please” before the clinician returned access to the reinforcers for 30 s.
The clinician taught the target communication response during training prior to each treatment evaluation phase. Teaching Chung to emit his FCRs (i.e., 4 by 4 in. and 2 by 2 in. communication cards) involved the clinician using a most-to-least prompting hierarchy to show Chung how to place the communication card in the clinician’s hand. The clinician began with an immediate physical prompt to use the communication card and began fading the prompt to partial physical and gestural prompts. The clinician used a full verbal prompt for Rich and Troy and gradually faded the verbal prompt (e.g., My way, my w…, my…, m…) while inserting a time delay of 2 to 5 s. The clinician provided 30-s access to individualized reinforcers for prompted or independent communication. If the participant engaged in nondangerous challenging behavior during training, the establishing operation was slowly progressed, meaning we continued to introduce transitions or instructions, and a prompt was provided to emit the FCR when the participant was calm and not engaging in nondangerous challenging behavior. In the event of dangerous problem behavior during training, the participant was immediately prompted to emit their FCR. If the participant emitted the FCR following the prompt, the reinforcers were provided, regardless of the presence or absence of dangerous challenging behavior. If the FCR was not emitted following the prompt and dangerous challenging behavior continued, all reinforcers were provided immediately, to ensure safety.
Participants met criteria to begin the treatment evaluation following two training sessions of five trials with 100% independent responding and little to no challenging behavior. The only difference between training and the treatment evaluation was that the clinician no longer provided prompts. If the participant did not emit the target FCR, the clinician continued to progress the evocative events, meaning continued to instruct them to transition or work on the present task. If the participant engaged in nondangerous challenging behavior, the evocative events continued to be progressed. If they emitted a dangerous response, reinforcement was provided to ensure safety. Sessions during the FCT treatment evaluation were 3 min and the reinforcer duration was 30 s.
Baseline ProbeFollowing the first phase of the FCT treatment evaluation for each participant, a baseline reversal was implemented. During the reversal, reinforcement was not provided contingent on the simple FCR. Instead, the FCR was denied and the evocative events were progressed until the participant engaged in challenging behavior. Reinforcement was provided for 30 s contingent on challenging behavior and the session was 3 min. The purpose of the reversal was to demonstrate continued functional control. It also provided additional evidence for the necessary subsequent skills to be taught in the next phase of SBT.
Delay/Denial Tolerance Training (DDTT)The clinician introduced delay/denial tolerance training (DDTT) following the participant successfully acquiring the complex FCR with little to no challenging behavior during the FCT treatment evaluation. If the participant was engaging in no challenging behavior or significantly less challenging behavior relative to baseline, DDTT was introduced. The clinician began DDTT by teaching the participant a tolerance response to emit following a denial to the complex FCR (e.g., “I’m sorry, we can’t right now, we need to do a little work first”). During tolerance training, the clinician reinforced the complex FCR for approximately 50% of the trials. During the other half of the trials, the clinician initiated the denial and only re-presented the reinforcers following the tolerance response. The clinician did not signal the reinforcement contingency; there were no discriminative stimuli signifying if the complex FCR was going to be reinforced or denied. Tolerance training used the same prompting strategies as FCT and included a separate treatment evaluation phase. Sessions during the tolerance treatment evaluation were 3 min and the reinforcement interval continued to be 30 s.
All skill-based teaching occurred within the same treatment evaluation contexts after the participant acquired the tolerance response and sessions were no longer time-based. In addition, the reinforcement interval was increased from 30 s to 1 min. Each session consisted of five (Rich and Troy) or six trials (Chung). Sessions with five trials consisted of (a) one trial in which the complex FCR was reinforced, (b) one trial in which the tolerance response was reinforced, and (c) three trials in which cooperation was reinforced (the six trial session included an additional trial in which the complex FCR was reinforced). Each of the three trials in which the clinician reinforced cooperation varied in the number of instructions that were provided. The cooperation trials with the least, middle, and most amount of work were designated as easy, moderate, and difficult, respectively. That is, the clinician presented reinforcement in a probabilistic fashion and no discriminative stimuli were included that signaled the response requirement to the participant. The order of the trials was determined randomly. The clinician created laminated cards, mixed them up, and selected each card until all trials for the session were determined. The clinician repeated this process for each session.
To maintain rapport, the clinician provided an empathetic statement and continued to present the evocative event if the participant exhibited an associated nondangerous behavior (e.g., “I know it’s hard but we can do this. Only a little more left!”). To avoid escalation and promote emotional safety (Rajaraman et al., 2022a), dangerous behavior resulted in the immediate discontinuation of the evocative events and a return to the preferred items. By returning reinforcers following dangerous behavior, the clinician treated these dangerous responses as a form of removing assent to participate (Breaux & Smith, 2023). Had the participant left the room entirely for more than 1 min, their choice would have been honored and the session would have been discontinued until the participant chose to return to the room on their own in a calm manner. The clinician never blocked a child from leaving the room or physically prompted the child to return to the room. Chung’s sessions were discontinued twice in this manner. This did not occur for any other participant.
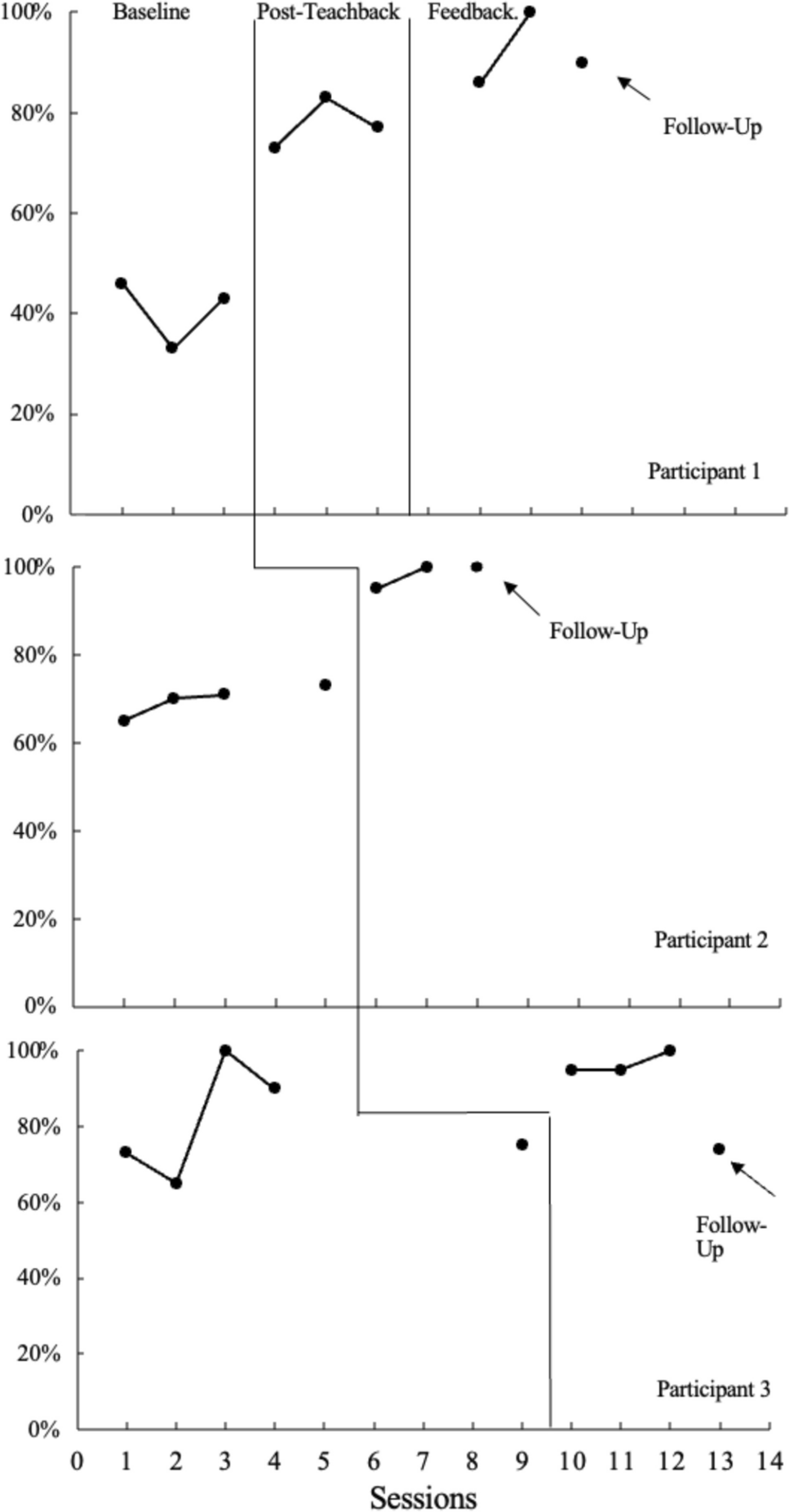
Reinforcement was thinned during DDTT using a contingency-based progressive delay (Ghaemmaghami et al., 2016). The three trials incorporating instructions were gradually increased in a systematic fashion while maintaining the same distinction between easy, moderate, and difficult. For example, the clinician initially presented the participant with only one instruction to cooperate with before reinforcers were returned. Once the participant met the criteria for successfully mastering cooperation with one instruction, sometimes the participant was then presented with one instruction (easy), two instructions (moderate), or three instructions (difficult) to complete. The next reinforcement thinning step could have included two instructions (easy), three instructions (moderate), or six instructions (difficult). The thinning steps were client specific and dependent on observed comfort level with evocative events (i.e., an increase in challenging behavior resulted in the need for smaller incremental steps). The criteria for moving on to each step primarily depended on three potential factors. This included challenging behavior remaining low, appropriate and stable use of the target communication and tolerance responses, and high levels of cooperation. After Troy took a vacation and a long time had passed after the last session, the clinician repeated a step and did not introduce a new step. This only occurred for Troy (see thinning level 4 in Fig. 3).
Novel ImplementersTo include family in the therapeutic process, sessions with novel implementers were conducted after DDTT with Rich and Troy. Rich’s mother was included in every session and she agreed to conduct sessions once he had mastered all thinning steps. Troy had a novel student observer who was a volunteer for the university-based clinic and had never worked with autistic individuals before but was interested in applied behavior analysis (ABA). Troy’s father also agreed to conduct one session after training. Chung’s father agreed to be trained but did not consent to formal sessions with video recordings or data collection. All novel implementers were trained using modeling, rehearsal, and feedback to conduct the final thinning level reached with the participant. No data were collected during the training. The clinician remained in the room during sessions to provide in situ feedback and instruct the novel implementer on what trial to conduct.
Social ValidationThe clinician provided caregivers with a social validity questionnaire following the participants’ discharge from services. The questionnaire included two sections with seven questions in total. The first section included three questions regarding the acceptability, safety, and representativeness of the functional assessment procedures. The second section included four questions regarding the satisfaction with improvement in challenging behavior and communication, helpfulness, and acceptability of the treatment procedures. Caregivers answered each question on a Likert scale ranging from 1 (lowest score) to 7 (highest score). Each question also included room for any open-ended comments and space was provided at the end of the questionnaire for any additional comments.
Comments (0)