
Remember me


Hyperphagia is a clinical symptom associated with some rare diseases of obesity described as an insatiable form of hunger characterized by a severe preoccupation with food [1,2,3,4,5]. Investigations into rare forms of obesity such as Bardet-Biedl syndrome (BBS); leptin, leptin receptor (LEPR), or proopiomelanocortin (POMC) receptor deficiencies; and acquired hypothalamic obesity have advanced our understanding of the biology of hyperphagia and its distinction from other overeating behaviors [2, 4, 6,7,8,9,10,11]. Underlying these rare forms of obesity are key signaling pathways, such as the leptin–melanocortin-4 receptor (MC4R) pathway, which centrally regulates energy balance and food intake through select hypothalamic structures [2,3,4, 6,7,8, 10, 12]. Disruptions in this signaling can occur with genetic disorders or acquired hypothalamic damage, both of which can frequently lead to pathologic hunger (i.e., hyperphagia), resulting in subsequent obesity and a pervasive, negative impact on quality of life [2, 3, 6,7,8, 10, 12, 13]. As compared with other overeating behaviors or “food noise,” patients with hyperphagia have a marked preoccupation with food and abnormal food-seeking behaviors that result from a shortened duration or failure of satiety following food intake [2, 4, 13,14,15,16]. While these and other characteristics can distinguish hyperphagia from other overeating behaviors, hyperphagia remains underrecognized and as a result is underdiagnosed [3, 13, 15]. In 2012, the 2nd International Conference on Hyperphagia was convened to focus on ongoing and future research opportunities regarding hyperphagia, primarily in the context of Prader-Willi syndrome (PWS) [4]. Continued research investigating the MC4R pathway has increased the understanding of the biology of hyperphagia. These advancements, combined with an increased availability of genetic testing, draw attention to the need for a standardized definition that can distinguish hyperphagia from other overeating disorders to support improved diagnosis and management of affected patients [4, 15]. In response to this need, an international group of physicians and scientists with expertise in hyperphagia convened in October 2023 during ObesityWeek, the annual meeting of The Obesity Society. The group discussed the need for a clear definition, a practical and accurate approach for screening and identification of affected patients, and management strategies for hyperphagia in patients with MC4R pathway–associated diseases [15]. This work serves as a summary of the proceedings from this discussion and provides potential approaches to improve the recognition and management of hyperphagia in patients with these underlying diseases.
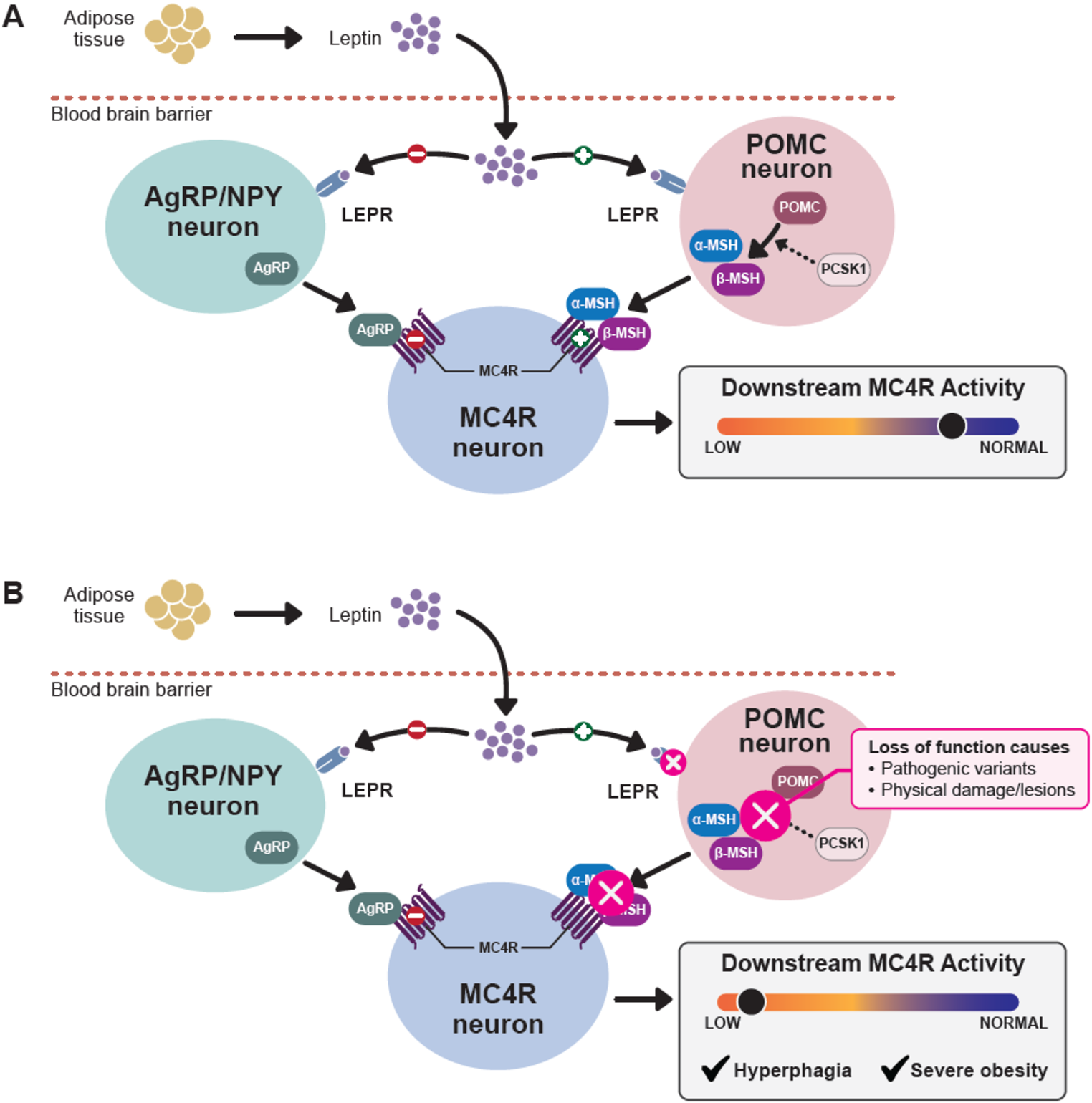
The Biology of HyperphagiaResearch investigating hunger and energy expenditure has identified the MC4R pathway within the hypothalamus as a key regulator of these functions. This pathway and its contribution to food intake have been extensively reviewed elsewhere (e.g., Baldini and Phelan 2019) [17]. Studies of genetic and acquired impairments of the MC4R pathway have improved the understanding of the mechanisms that underlie hyperphagia [1,2,3,4, 6, 7, 10, 17, 18]. Briefly, under physiological conditions, upstream activation of MC4R by release of α–/β–melanocyte-stimulating hormone (α-/β-MSH) from hypothalamic POMC-expressing neurons decreases food intake and increases energy expenditure; these effects are balanced through inhibition of MC4R by agouti-related peptide (AgRP), an inverse agonist, released by hypothalamic AgRP-expressing neurons [4, 7, 10, 12, 17, 19, 20] (Fig. 1A). Deficiencies in upstream generation of α-/β-MSH can occur through a variety of mechanisms, including variants in genes involved in the MC4R pathway (Fig. 1B) and those that contribute to the formation of the BBSome, a collective group of proteins that guide cilia formation and regulate LEPR trafficking [20,21,22]. Additionally, stimulation of serotonin receptor 2 C expression in POMC neurons can further regulate MC4R signaling by enhancing POMC-mediated release of α-MSH and suppressing inhibitory AgRP activity on MC4R receptors [23, 24]. Thus, alterations in expression or splicing of serotonin receptor 2 C, potentially resulting from loss of paternal expression of SNORD116 (as in PWS) and BBS1 (as in BBS) could further dysregulate MC4R signaling [1, 18, 24,25,26]. Impairments in these upstream components of the MC4R pathway ultimately result in hyperleptinemia, in the context of leptin resistance resulting from LEPR deficiencies, and hyperinsulinemia, facilitating the development of hyperphagia and increased energy intake [9, 11, 12, 27, 28].
Fig. 1
The hypothalamic melanocortin-4 receptor (MC4R) pathway. (A) MC4R signaling under physiological conditions. (B) Disruption of MC4R signaling
Variations in the underlying pathophysiology and resulting impairment of MC4R pathway signaling influence the severity of symptoms and behaviors of hyperphagia [6, 10, 12, 29]. While symptoms of hyperphagia have been observed to cluster across underlying pathologies, genetic variants that may result in hyperphagia can be associated with differing severity of functional impacts to MC4R signaling [6, 10, 30]. Additionally, these presentations can be confounded by a level of neurocognitive impairment within individuals with a specific underlying disease [4, 14, 31]. Thus, the presentation of hyperphagia does not always strictly follow such pathology-specific distinctions and there can be significant overlap of the symptoms of hyperphagia among the diseases that underlie this condition [15].
Defining HyperphagiaA variety of obesity-related diseases can present with hyperphagia, each with a cluster of common symptoms related to the underlying pathology (Table 1). Given the wide range in symptoms and severity, there is a need to establish a clear lexicon that includes both a general definition of hyperphagia along with separate expansions to differentiate underlying pathologies [15, 31]. Such a definition must take into consideration the age of the patient and the impact of cognitive status [4, 5, 15]. Although symptoms overlap between diseases, hyperphagia with PWS is considered the most severe presentation and is characterized by a relentless, overwhelming preoccupation with food (i.e., food noise), extreme hunger, and obsessive or unusual behaviors regarding food (e.g., waking at night to eat, eating nonfood items) [1, 4, 15, 31,32,33,34]. Patients with PWS can also experience extreme anxiety around food and exhibit tantrums, outbursts (especially during attempts at food restriction) [1, 4, 15, 33], and compulsive behaviors [31, 32]. These symptoms likely result from the underlying etiology of PWS, namely deletion of the paternally inherited chromosome 15q11-q13 region (and rarely microdeletions including the SNORD116 gene cluster), or duplication of maternally inherited chromosome 15, which affects the expression of several maternally imprinted genes [1, 4, 18,
Comments (0)