
Remember me

Mobilizing patients in the NICU presents unique challenges specifically due to the complex pathophysiology of neurological conditions. Medical management of the NICU patient not only involves monitoring physiologic parameters but requires close attention to cognitive status.
Physiologic BarriersWhen considering ICU mobilization, patients with neurologic injuries pose distinctive challenges due to their dynamic and complicated disease process. Patients often exhibit altered consciousness, impaired cognition, compromised comprehension, motor dysfunction, hemodynamic instability, and increased susceptibility to secondary neurological injuries, necessitating a cautious approach to minimize the risk of adverse events [3,4,5]. Determining eligibility for mobilization in these patients requires careful consideration of patient-specific factors [6]. Establishing standards for mobilization regarding timing, dose, frequency, and duration remains challenging due to heterogeneous trials and the lack of well-established protocols.
When considering medical factors that influence the dosage or timing for mobility, one must account for the patient’s primary neurological injury, potential for secondary injury, and other medical conditions resulting from their neurological injury. Mobility that is too intense or initiated too early after a neurological injury may provide no benefit and could be detrimental [6,7,8]. Resolution of shock and intracranial pressure (ICP) crises are imperative prior to ICU mobility. Additionally, ensuring adequate perfusion to the central nervous system helps mitigate the risk of ischemic events [9]. Traditional management of intracranial hypertension such as: hyperosmolar therapy, cerebral spinal fluid diversion, hyperventilation, hypothermia, analgesia, sedation, barbiturate coma, and decompressive surgery, come with significant side effects and limitations to mobilization [10,11,12,13,14,15,16,17,18,19].
Patients with spinal cord injury (SCI) serve as a prime example of such complexity. These patients may have unstable injuries requiring early surgical stabilization. The sequelae of SCI, such as respiratory failure, bradycardia, hypotension, and neurogenic shock, must be well managed before mobilization can be safely initiated. In some cases, this necessitates interventions like temporary pacemaker placement [20] and tracheostomy insertion [21,22,23]. Proper management of these conditions is crucial to mitigate the risks associated with mobilization.
The heterogeneity of trials and the lack of well-established protocols make it difficult to standardize mobilization practices. Each patient’s unique medical condition necessitates a tailored approach to determine the appropriate timing, dose, frequency, and duration of mobilization activities. For instance, the mobilization of patients with traumatic brain injury (TBI) must consider the risk of increased intracranial pressure with careful assessment of neurologic status to avoid exacerbating injury [24,25,26]. Protocols for patients with SCI may involve staged mobilization strategies starting with passive range of motion exercises, progressing to active assisted movements once hemodynamically stable [7]. This progression helps to prevent complications such as deep vein thrombosis (DVT) and muscle atrophy while ensuring patient safety.
Although there are medical challenges for mobilization in the NICU, current evidence demonstrates this practice is safe and beneficial. Verticalization and mobility have shown promise in improving functional outcomes in neurologic populations [27, 28]. In addition to functional benefits, mobility can aid with many goal-directed therapies. Use of specialty beds not only facilitates mobility, but also treats medical issues like intracranial hypertension. Studies have shown that patients with refractory intracranial hypertension who were treated with verticalization had lower ICP, fewer ICP spikes, and decreased total number of medical interventions needed after verticalization compared to prior [29]. With proper preventative measures such as compression stockings and abdominal binders to mitigate orthostatic hypotension, verticalization has been well tolerated in this patient population, with cautious attention to pressure wounds [29, 30]. Integrating verticalization early in the treatment of intracranial hypertension may help mitigate the side effects seen with traditional treatments.
Mobilizing patients in the NICU is fraught with medical and physiological challenges that require a nuanced and individualized approach. Understanding the complex interplay between neurological injuries and systemic medical conditions is crucial for developing safe and effective mobilization protocols. Ongoing research and clinical trials are essential to establish evidence-based guidelines that can standardize practices and improve patient outcomes in the NICU. By carefully considering patient-specific factors and potential risks, healthcare providers can optimize mobilization strategies to enhance recovery while minimizing the likelihood of adverse events.
Cognitive ChallengesCognition can be defined as the process of acquiring or maintaining knowledge through the interpretation of thoughts, prior experiences, and various sensory inputs. It encompasses multiple domains, including memory, attention, arousal, affect, language, and executive function, to name only a few. Neurologic disorders are the leading cause of cognitive disability [31]. Critically ill patients with respiratory failure or shock are at risk of developing long-term cognitive deficits [32].
Patients that present with cognitive impairments or disorders of consciousness in the NICU are especially challenging to mobilize [1]. Patients that are confused, difficult to redirect, or unable to follow commands are more likely to unintentionally remove invasive lines, drains, and monitors; therefore, constant vigilance is necessary when attempting mobility in this setting. Some may even require the use of physical restraints to prevent the disruption of necessary medical equipment, further inhibiting a patient’s likelihood to mobilize out of bed thus leading to deconditioning [33]. When considering all factors, many providers may be hesitant to mobilize patients out of bed.
Despite these challenges, ICU mobility has been shown to reduce cognitive dysfunction, particularly in critically ill patients that require invasive monitoring or mechanical ventilation [34]. Prompt consultation with physical and occupational therapy can facilitate early mobility in patients that are cognitively impaired. Additionally, therapists can provide cognitive interventions and further recommendations to healthcare staff regarding safe mobilization of these patients, including mechanical lifts or alarm systems. Evidence to support the use of restraints is mixed, with some studies suggesting the risks outweigh the benefits of use [35]. Patients can often still be mobilized out of bed with restraints if a provider can provide direct supervision for a short time, assuming the patient is not combative. In addition, one-to-one supervision can also facilitate early mobility and improve time out of bed. Recent advances in medical technology allow for remote supervision via video monitoring surveillance when in-person staffing is limited, assuming these patients can be redirected easily.
Additionally, patients with unresponsive wakefulness syndrome (formerly known as vegetative state) and minimal consciousness can be mobilized out of bed despite low levels or arousal or awareness. Studies have shown that the use of tilt tables and verticalization beds can improve arousal and consciousness [27, 36]. Outcome measures such as the Coma Recovery Scale-Revised (CRS-R), Coma Recovery Scale Revised-For Accelerated Standardized Assessment (CRSR-FAST), and Motor Behavior Tool-Revised (MBT-r) are validated measures that can detect subtle signs of consciousness and be used to track improvements in consciousness when using mobility interventions in these populations [37,38,39].
DeliriumDelirium is a condition characterized by an acute, significant decline in attention and cognition [40]. This condition is common in adults over the age of 65 in the acute care setting. Delirium can manifest as hyperactive, hypoactive, or a mixture of both [41]. Patients that experience delirium tend to have longer length of stay, increased healthcare costs, earlier loss of independence, and increased morbidity and mortality [42,43,44,45]. This becomes even more prevalent in the neurocritical care setting [46, 47]. Providers often choose to reduce light and stimulation in response, either to promote sleep or reduce agitation. Unfortunately, this only hastens the development of delirium. The symptoms of this condition are often missed in neurologic populations, largely because it can be attributed to the patient’s primary neurologic diagnosis [48]. In turn, this often leads to an increase in the frequency of bedside neurologic examinations to assess for changes in patient presentation, further exacerbating delirium. Increased frequency of neurological exams can hasten the development delirium in some neurologic populations [49].
Preventive measures play a crucial role in managing delirium and promoting appropriate sleep cycles. Mobilization out of bed, exposure to light during waking hours, and establishment of a daily routine are fundamental strategies in this regard [50,51,52]. Collaboration with the multidisciplinary team is essential, particularly in the selection of sedation and analgesics. Continuous sedation should be minimized. Employing the lowest effective dose of analgo-sedation to achieve treatment goals is imperative not only for serial neurological examinations and maintaining alertness but also for preventing delirium [50]. Moreover, the implementation of a delirium bundle focused on promoting sleep-wake cycles for all NICU patients can serve as both a treatment and prevention measure for delirium, facilitating mobilization efforts in the process [50, 52].
Some delirium risk assessment tools can also be beneficial in predicting patients who are at risk for developing delirium. For instance, the AWOL is a mnemonic phrase in which a patient is assigned one point in four different domains; a score of two or more indicates a patient is at high risk for developing delirium [53]. Another measure is the CAM-ICU, which can help identify patients that have already developed delirium so that appropriate interventions may be implemented [54] (Table 1).
Once a patient has been deemed at risk or has already developed delirium, bedside nurses can implement strategies to optimize patient recovery in the NICU. One of the most effective strategies to improve delirium in the NICU is the ABCDEF bundle. When all components of the bundle are used together, it can be an extremely effective tool to prevent delirium. This mnemonic includes the following components [55].
A)Assess, prevent, and manage pain.
B)Both spontaneous awake trials and spontaneous breathing trials should be performed regularly.
C)Choices of analgesics and sedatives are key and should be used sparingly when possible.
D)Delirium should be frequently assessed and managed.
E)Early mobility and exercise facilitate improvements.
F)Family engagement and empowerment are key.
Fall RiskFalls are generally defined as an unintentional event in which a person comes to rest at the ground or a lower-level surface in an uncontrolled manner, excluding certain intrinsic (stroke, syncope) and extrinsic (natural disasters, physical violence) circumstances [56]. Each year, up to one million adults fall in the hospital setting [57]. Falls in the inpatient setting often occur when patients ambulate without required assistance, attempt to perform elimination-related activities, or are mobilized at night [58, 59]. Although falls occur less frequently in the critical care setting, patient harm is reported up to 51% of the time [60]. Patients in the NICU are at particular risk when considering the increased frequency of cognitive and motor deficits in these populations [61,62,63]. Additionally, the need for invasive monitors, lines, drains, and medical devices in this population presents additional risks if a fall were to occur, including infection and dislodgement.
Initial risk assessments regarding falls are typically deferred to bedside nurses. However, a multidisciplinary approach to fall prevention education may reduce the frequency of falls on neurologic care units [64]. In addition, a multi-faceted approach to mitigate falls risk, including the use of fall-risk bracelets, lowered beds, use of alarm systems, restraints (as needed), and polypharmacy assessment, can be effective at reducing the number of falls on an inpatient neurology unit, whereas many of these interventions are less effective as a stand-alone method [65]. Physical and occupational therapists with advanced skills in the NICU setting are especially useful for preventing falls. Tests such as the Five Time Sit-To-Stand Test (FTSST), Timed Up & Go (TUG), and the Two Minute Walk Test (2MWT) are easy, safe, and reliable measures for assessing falls risk in ambulatory patients in the neuro ICU [66]. Additionally, the Tyndall Bailey Falls Risk Assessment Tool (TB FRAT) is a reliable assessment that specifically measures falls risk in the ICU setting [67].
Table 1 Useful tools and measures to facilitate mobility in the NICUChallenges and Opportunities: SurgicalMobilization in the Neuro Intensive Care Unit (NICU) is essential for enhancing patient recovery and minimizing complications related to prolonged immobility. However, specific surgical challenges exist that can hinder mobilization efforts.
Activity RestrictionsPatients with neurologic injury are particularly prone to impulsivity and agitation, increasing the risk of falls and other complications [71, 72]. This risk is amplified in patients who have undergone neurological surgery, such as craniotomy, decompressive hemicraniectomy (DHC), or the placement of an intracranial device. Post-procedural activity restrictions, including bed rest, head of bed level restrictions, and movement precautions due to arterial access can delay mobilization efforts. For example, patients undergoing cerebral angiogram face a risk of arterial bleeding from the access site, especially when timing of mobilization is considered for those with arterial groin access [73].
Neuro-interventional proceduralists have demonstrated the safety and efficacy of using transradial access for diagnostic and interventional procedures compared to the transfemoral site with equal rates of aneurysm securement for both locations [74] The major benefit of transradial access in neurocritical care patients is the reduced need for post-procedure immobility and bed rest restrictions. This advancement allows for earlier and safer mobilization of patients [75].
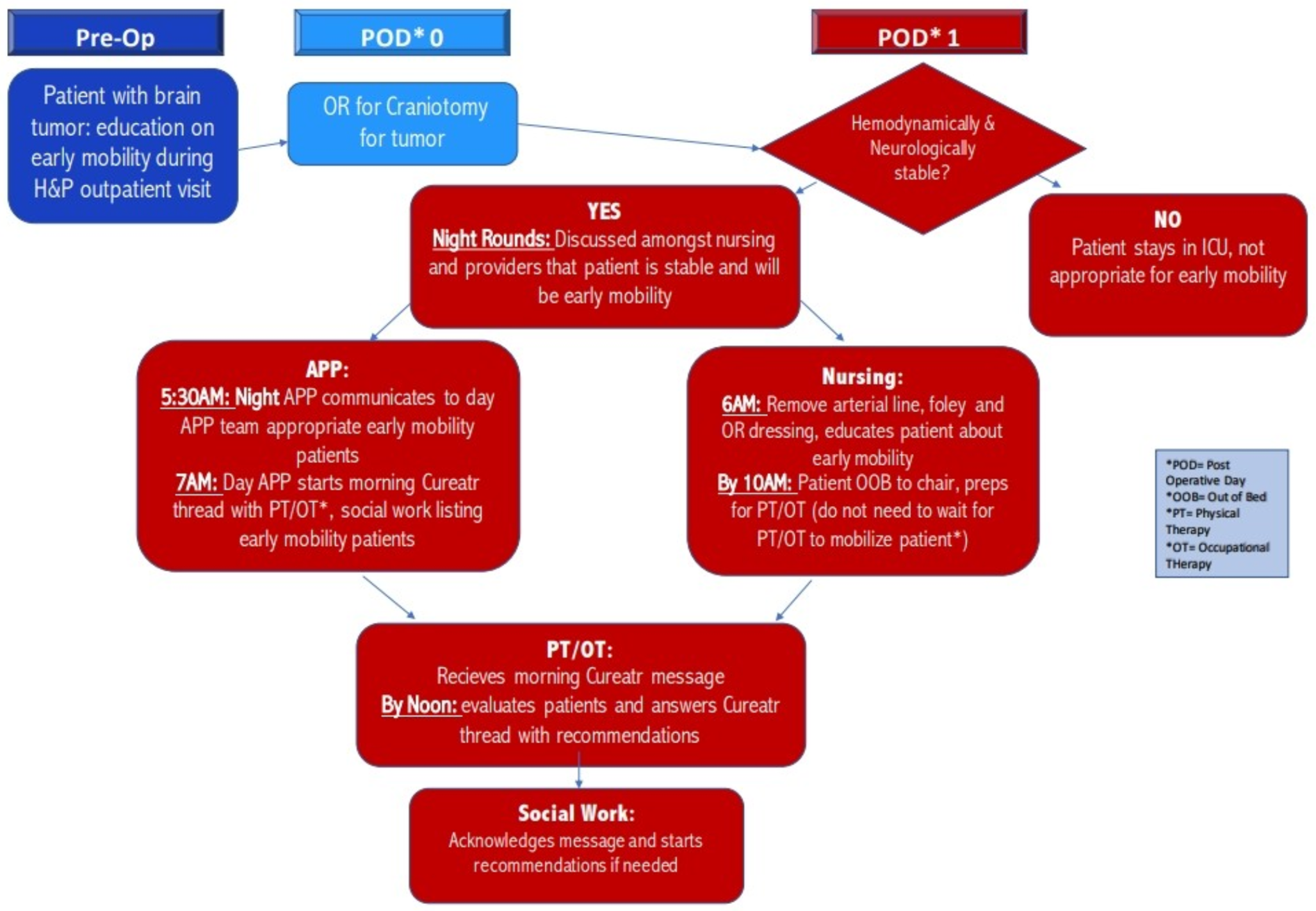
The creation of postoperative mobilization protocols presents the greatest opportunity to improve mobilization in post-surgical patients within the NICU. These protocols enable staff to mobilize patients confidently, while incorporating built-in safety checks. Standardizing utilization of Enhance Recovery After Surgery (ERAS) protocols among the NICU population has been shown to decrease ICU length of stay (LOS), opioid needs, and insulin requirements [76]. ERAS protocols applied specifically to the craniotomy population can expedite postoperative care without increasing complications [77]. Standardized mobilization protocols for patients with craniotomy on the first day post-operatively ensure safe early mobilization while also decreasing ICU LOS (Fig. 1).
Fig. 1
Example mobility protocol for patients status post craniotomy at penn medicine. The redesign and implementation of a protocol to improve early mobility and decrease length of stay in intensive care unit (ICU) patients following elective craniotomy [2021]. Source Permission: Kathryn Kessler, DNP, CRNP
Invasive Lines and DrainsInvasive devices such as external ventricular drains (EVDs) and lumbar drains pose risks of dislodgement during mobilization, potentially leading to over or under-drainage of cerebrospinal fluid (CSF), altered intracranial pressure (ICP), infection risks, and neurologic decompensation [78,79,80]. The procedural risk of re-inserting invasive drains after dislodgement must be carefully consid
Comments (0)