Studies Overview
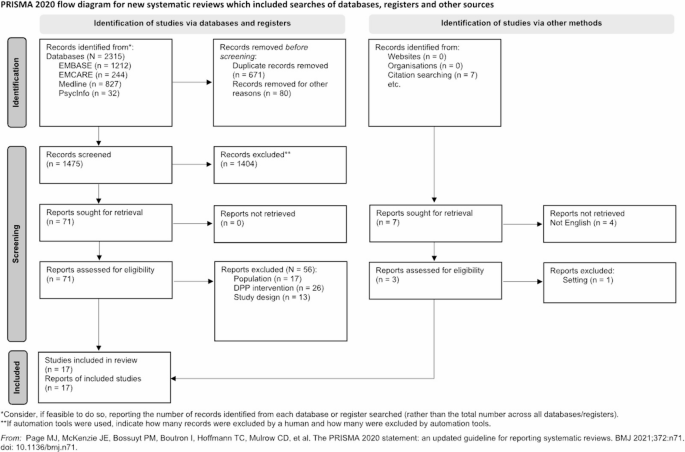
Out of the 28 manuscripts included, five focused on intervention development, eight described intervention protocols, and 15 were intervention outcome studies. Among the latter outcome studies, experimental designs varied: six were randomized controlled trials (RCTs) [49,50,51,52,53,54], six were single-group, pre-post studies [55,56,57,58,59,60], two were pilot RCTs [61, 62], and one was a non-randomized pragmatic effectiveness trial [63]. All protocol manuscripts detailed RCTs [64,65,66,67,68,69,70,71]. Out of the five intervention development manuscripts, four qualitatively described the phases of text-messaging development [72,73,74,75], and one included a survey where participants evaluated and refined the intervention’s text-message library [76]. Geographically, the studies were widely dispersed: 16 were conducted in the U.S., three each in Australia and the UK, and two in South Africa. Additional countries represented included India, Spain, Saudi Arabia, Sri Lanka, Bangladesh, and Thailand.
Text-messaging integration took two forms. Often, the integration of text-messaging aimed to evaluate whether additional content delivery through text-messages could enhance participant engagement, improve outcomes, sustain behavior changes, or nudge participants to enroll in in-person programs. Yet, many studies utilized text-messaging as the primary delivery method for T2DM prevention content [49, 50, 53, 56, 57, 59, 62, 68, 71, 73, 75].
Settings and Recruitment
Many studies were integrated within healthcare settings, including primary care clinics, federally qualified health centers, and hospitals. Four studies explicitly focused on implementing text-messaging interventions within these settings, aligning with existing workflows, and using Electronic Health Record (EHR) data for recruitment [55, 58, 63, 64]. Ritchie et al. (2020) and Fischer et al. (2019) applied the SMS4PreDM program in a safety net healthcare system [58, 63]. The myAgileLife DPP study was also implemented in a large healthcare system and identified participants through laboratory data, EHR mentions of prediabetes, or direct provider referrals, with self-enrollment via a web portal to facilitate recruitment [55]. The BEGIN study conducted a pragmatic trial in a federally qualified health center, using an EHR algorithm for participant identification and an opt-out recruitment letter to explain study objectives and participation [64]. Studies also utilized community-based strategies for participant recruitment, including participation in health fairs, local events, health promotion activities, and sporting events. Additionally, studies employed various additional recruitment methods, such as research databases, invitation letters, newspaper and social media advertisements, phone calls, and emails.
Intervention Development and Content
Studies focused on intervention development provided the most detailed insights into this process, but summaries were also available in protocols and outcome studies, though with varying levels of detail. Researchers typically employed multi-phase processes to develop text-message content. Some investigators developed the content themselves, leveraging their expertise and insights from literature reviews [51, 52, 60, 61]. Others collaborated with experts such as clinicians (physicians, dietitians), certified lifestyle change educators/coaches, and physical activity trainers [49, 55, 56, 62, 64,65,66]. These collaborations often involved multiple meetings with the expert team, utilizing interviews, focus groups, or workshops. Additionally, some researchers included potential participants and individuals with prediabetes or T2DM in the program development process [50, 53, 58, 63, 67, 70, 75]. One study utilized artificial intelligence to develop the intervention content [59]. While some authors independently developed the message library and later sought feedback for refinement, others employed a fully co-designed approach, engaging collaborators throughout the development process. For instance, Hill et al. (2023) used an 11-step approach, which included evidence review, needs assessment, expert input, content development, readability and acceptability evaluation, and refinement based on participant feedback [74].
Commonly, included studies modified evidence-based content and curricula developed through RCTs, such as the DPP trial, whose curriculum includes strategies for lifestyle modification with information about nutrition, physical activity, and behavioral self-management [77]. In studies conducted in the U.S., authors often utilized the National DPP curriculum, which is based on the DPP trial materials [78]. Adaptations to the curriculum were sometimes made to suit the population served or the context in which the study was being tested. For studies outside the U.S., adaptations of DPP content were tailored to fit the specific cultural and contextual needs of the respective countries. For example, in Lifestyle Africa the investigators adapted the National DPP curriculum to make cultural, educational, and language adaptations relevant to the local community [67]. A few studies relied on general lifestyle change content about diet and physical activity, without specific references to using content from DPP or other evidence-based programs.
As expected, the text-messages were primarily focused on promoting physical activity and healthy dietary practices for weight loss, with content and behavioral strategies around these topics similar to those included in the DPP curriculum. This included goal setting, promotion of self-efficacy, motivation, coping with barriers, stress reduction, and skill teaching (e.g., tracking calories and exercise), among others. Additionally, some studies included content about T2DM pharmacotherapies (i.e., metformin). A few studies incorporated other topics to fit the study objectives, such as sleep goals, prompts to join in-person programs, and breastfeeding.
Text-messaging DetailsFrequency
The frequency of messages and the duration of text-messaging programs varied widely across studies. Due to differences in program lengths and intensities, it is challenging to estimate the average number of messages typically sent as part of the interventions. Some programs were more intensive, sending multiple messages per day (up to four), while others sent a few messages per week or only monthly messages (Table 1).
Table 1 Characteristics of studies on text-messaging interventions for type 2 diabetes preventionTailoring
Some studies tailored messages to participants based on various characteristics. The simplest method for tailoring involved using participants’ names or sending messages at their preferred times. More sophisticated tailoring was also utilized. For example, Rollo et al. (2020) personalized messages based on barriers identified by participants as impacting their ability to eat healthfully and be physically active [61]. Nanditha et al. (2020) tailored messages according to participants’ stages of change based on the Transtheoretical Model (TTM), with messages specific to each stage (pre-contemplation, contemplation, preparation, action, and maintenance) [53]. Cheung et al. (2019) used prespecified algorithms to send personalized messages based on baseline data, such as ethnicity and breastfeeding status [62].
Unidirectional vs. Bidirectional Messages
While most studies allowed only one-way communication, some offered bidirectional interaction. This included automated responses based on participant replies (i.e., on-demand) or live interactions with human operators (e.g., lifestyle change coaches). Automated systems used keywords so that participants could receive follow-up messages. Some studies asked participants to reply to the messages with their weekly weight or other specific requests. In a few cases, participants could send free text-messages monitored by investigators or lifestyle coaches, who would then respond to the participants, providing support on the topics mentioned in their messages [15, 55]. In myAgileLife DPP, a lifestyle coach contacted participants at least once per module, and more often if necessary, to discuss module content and lifestyle recommendations [55].
Wearables
Some studies also incorporated wearable monitors, such as the Fitbit smartwatch and physical activity tracker to complement the program [49, 52, 54, 57, 62, 71]. These devices captured physical activity in real-time and provided immediate feedback through text-messages. Some also combined the Fitbit watch with the app for tracking dietary practices. For example, Soltero et al. (2023) tailored text-messages based on participants’ step counts, with weekly goals increasing incrementally [71]. In Steward et al. (2022), participants used the Fitbit app to log food consumption and physical activity, receiving personalized text content based on their entries [57].
Participants
The smallest study, a pre-post feasibility study, included 23 participants [59], while the largest, an RCT, had 1,031 participants [53]. Consistent with the DPP translational literature, which has demonstrated the underrepresentation of men in T2DM prevention interventions [14], we observed that men were less likely to participate in the interventions included in this review. One exception was a protocol by Sinclair et al. (2020), which was specifically designed for American Indian and Alaska Native men [70].
Participants were typically older than 40 or 50 years, reflecting the higher prevalence of prediabetes in older populations [13]. Studies targeting women with a history of gestational diabetes enrolled younger participants, averaging in their thirties [49, 61, 62, 69]. Two interventions focused on children and adolescents, addressing the high prevalence of obesity in youth and their associated risk for developing T2DM [59, 71, 75]. Studies conducted in the U.S. tended to focus on racial and ethnic minority groups, such as Hispanic/Latinos, Blacks, and American Indian/Alaska Native men, or included a representative percentage of participants from diverse races and ethnicities.
T2DM risk was primarily assessed using hemoglobin A1c or fasting plasma glucose. Intervention development studies tended to be vague about inclusion criteria, generally stating participants had prediabetes or were at high risk of T2DM [72,73,74, 76]. For studies targeting women with previous gestational diabetes, a prior diagnosis was used to assess T2DM risk [49, 61, 62]. Notably, a few studies assessed T2DM risk solely based on overweight/obesity levels (through body mass index [BMI]) [67, 70, 71, 75], with one study justifying this approach to be more inclusive of potential participants [67].
Feasibility and Acceptability
Table 2 presents an overview of the studies’ feasibility, acceptability, and effectiveness. Nine studies that reported outcome data included data on feasibility and/or acceptability. Feasibility was assessed through recruitment and retention rates, engagement levels (






Comments (0)