
Remember me






This prospective study included patients who were admitted to the Department of Emergency and Critical Care Center at Uonuma Kikan Hospital and who were prescribed physiotherapy between June 2020 and December 2022. In this study, critically ill patients were defined as those who stayed in the ICU for at least 48 h. The eligibility criteria were as follows: ability to start mobilization according to a doctor’s decision that was based on the criteria for early mobilization or initiation of active exercise from an early stage [4] and acquisition of consent for participation from the patients themselves or their family members. Patients were excluded if they spent < 48 h in ICU, if they were aged < 18 years, if their body mass index (BMI) exceeded 35 kg/m2, if they had new-onset cerebral strokes, if their rSO2 could not be measured because of a poorly fitting probe for NIRS, or if they refused active treatment.
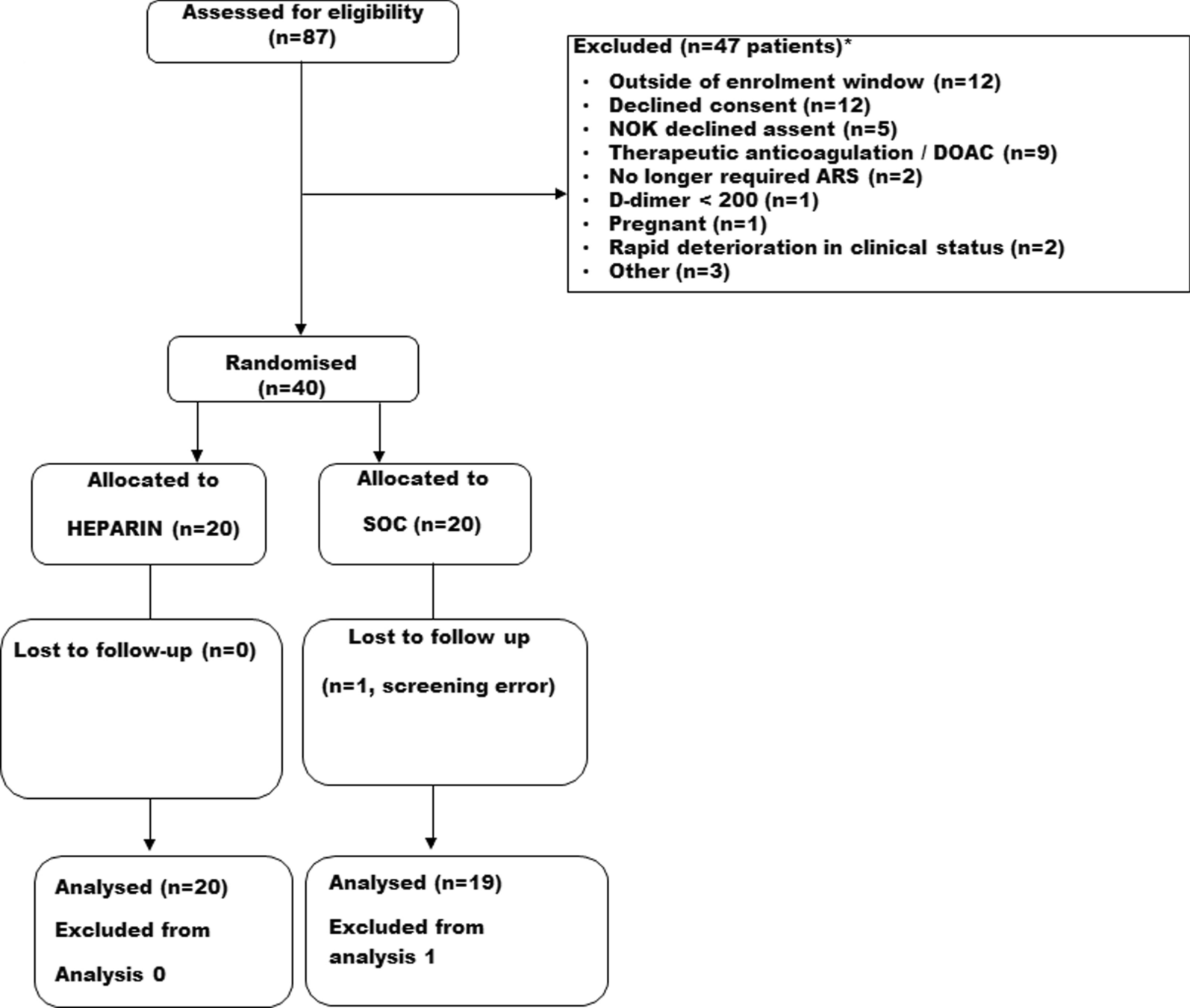
Patients who met these eligibility criteria were selected and grouped into tertiles based on their rSO2 values, and the patient backgrounds were compared. Subsequently, the association between rSO2 before initial mobilization and in-hospital death was investigated (Analysis 1). To investigate the temporal changes in rSO2 and other vital signs before and during initial mobilization (Analysis 2), patients whose measurements were interrupted during mobilization were excluded. Missing data were primarily caused by interruptions in measurement due to the displacement of the NIRS probe during mobilization or by the premature termination of mobilization owing to clinical conditions such as hypotension. These patients were excluded because these interruptions made it impossible to accurately analyse the changes during mobilization.
VariablesBasic patient data, including age, sex, BMI, Acute Physiology and Chronic Health Evaluation II (APACHE II) score on ICU admission, underlying diseases, and the cause of death for in-hospital fatalities, were collected from medical records. Data regarding previous ventilator use, oxygen administration, catecholamine use, number of days to initial mobilization, duration of ICU stay, and blood haemoglobin (Hb) concentration at the start of initial mobilization were also collected.
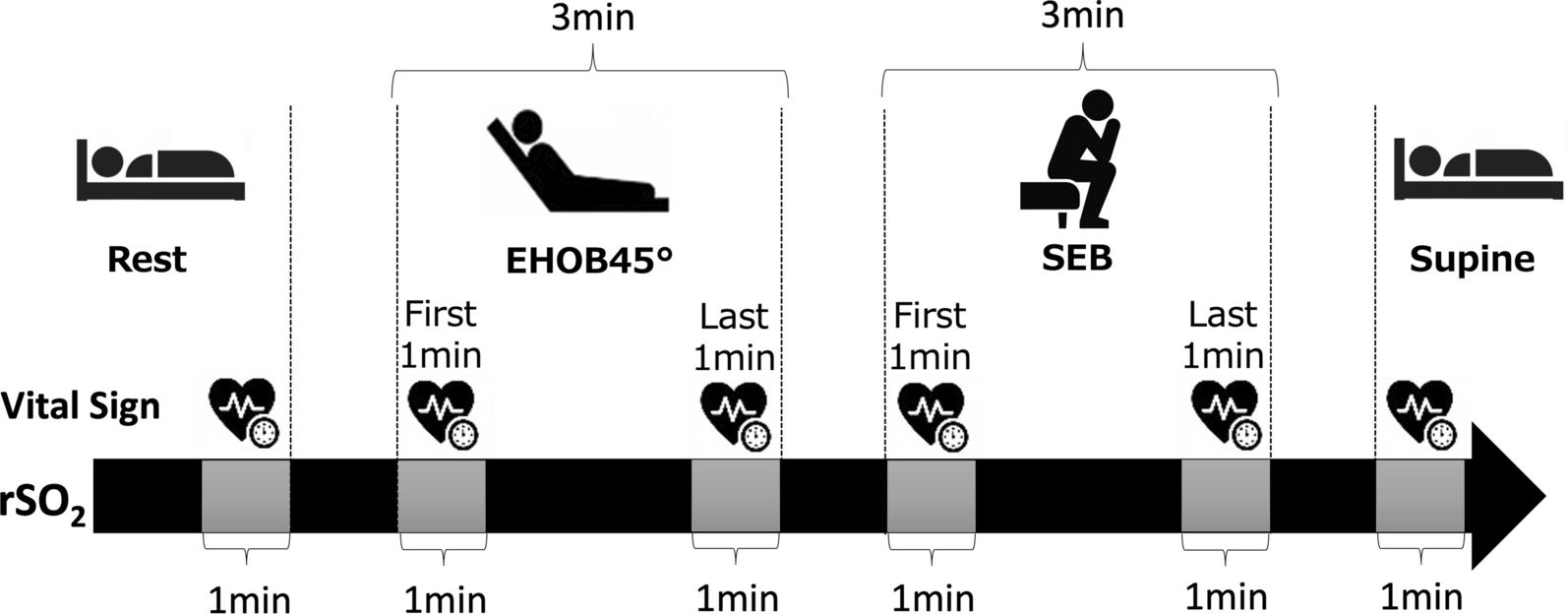
MobilizationIn this study, mobilization was defined as rehabilitation at the level of sitting on the edge of the bed (SEB; sitting position) or more [14]. First, the patients lay supine on the bed to relax for 5 min; rSO2 measurement was initiated 1 min before the start of mobilization. The HR, BP, and SpO2 were also measured. Figure 1 shows the mobilization procedure. It involved resting (supine), laying with the head of the bed elevated to 45° (EHOB45°), and SEB. The duration of each step was 3 min. This duration was determined based on early mobilization protocols tailored for critically ill patients. Particularly, extended physical exertion poses risks in the ICU, and short-duration mobilization is recommended, according to the study by Schweickert et al. [2]. Additionally, the Critical Care Guidelines (2018) advise beginning mobilization with brief, manageable sessions to assess patient tolerance [15]. This approach enables patients to adopt a seated position safely and within their limits. The rSO2, HR, BP, and SpO2 were measured from the rest period before the start of mobilization until the patient was once again supine at the end of mobilization. Head and torso movements were minimised during the procedure.
Fig. 1
Mobilization procedure. The patient first lies down in the supine position and rests. The head end of the bed is then raised to 45°. Next, the patient sits on the edge of the bed. Each step lasts for 3 min. The rSO2 values are measured continuously from the resting position until mobilization is complete. Blood pressure and transcutaneous oxygen saturation are measured at six points: at rest, during the first 1 min of EHOB45°, during the last 1 min of EHOB45°, during the first 1 min of SEB, during the last 1 min of SEB, and while lying on one’s back. The rSO2 value is calculated as the average value over 1 min at the same six points. EHOB45°: head of the bed elevated to 45°; rSO2: regional cerebral oxygen saturation; SEB: sitting on the edge of the bed
rSO2 measurementsThe rSO2 was continuously measured using a wearable brain NIRS device (Brain Activity Monitor Hb133, Astem, Kanagawa, Japan) with two measurement channels having peak wavelengths of 770 ± 10 and 830 ± 10 nm, respectively. The distance between the probes was 35 mm. This device reportedly measures the status of oxygenation on the brain’s surface at a depth of approximately 12–20 mm beneath the skin [16]. The region of interest was the prefrontal cortex, which is not covered by hair and is considered to play a critical role in the ability to selectively allocate attention and integrate visual and proprioceptive information [17]. To ensure that the measurement sites were consistent, we fitted a special head mount to the patient’s forehead so that the probes were in close contact with the prefrontal cortex locations FP1 and FP2 according to the international 10–20 system [18], with measurements continuously obtained from start to finish of the initial mobilization. The sampling rate was 10 times per second (10 Hz), and the measured data were recorded on a computer via Bluetooth. The FP1 and FP2 measurement data were averaged and used as the rSO2 values before and after changing position for each of the following: rest before mobilization, during the first 1 min of EHOB45°, during the last 1 min of EHOB45°, during the first 1 min of SEB, and during the last 1 min of SEB, and during the 1 min in the supine position at the end of mobilization.
Measurements of vital signsThe vital signs used for risk assessment and management during mobilization included HR, systolic BP (SBP), diastolic BP (DBP), mean arterial pressure (MAP), and SpO2. An IntelliVue X2 patient monitor (Philips, Amsterdam) was used to monitor the patients. HR was measured using the three-lead monitoring method (lead II) with the electrode applied to the chest, and the SBP, DBP, and MAP were measured using a noninvasive BP cuff placed on the upper arm. The SpO2 was measured using a disposable probe worn in a way that it enclosed the tissue of any of the fingers at a point where it was 6–18 mm thick. Each of these indicators was measured and recorded by the patient monitor at the following six time points during the initial mobilization: rest before mobilization, during the first 1 min of EHOB45°, during the last 1 min of EHOB45°, during the first 1 min of SEB, during the last 1 min of SEB, and during the 1 min in the supine position at the end of mobilization (Fig. 1).
Statistical analysesAnalysis 1: This analysis aimed to examine whether premobilization rSO2 value and the primary endpoint of in-hospital death are associated. To compare the characteristics of patients categorised into the three study groups based on their rSO2 values, we used a one-way analysis of variance and the Kruskal–Wallis test or Fisher’s exact test. The normality of the data was evaluated using the Shapiro–Wilk test. The vital signs before mobilization were analysed in the same way.
The association between premobilization rSO2 and in-hospital death was analysed using logistic regression analysis adjusted for age and the APACHE II score, with in-hospital death (survival/non-survival) and rSO2 as the target and explanatory variables, respectively. Collinearity between the variables was evaluated using the variance inflation factor. Receiver operating characteristic (ROC) curve analysis was used to evaluate the optimum cut-off value of rSO2 for in-hospital death. The Youden index was used as the criterion for deciding the cut-off value. Next, to evaluate the ability of rSO2 to predict death, we conducted a logistic regression analysis using in-hospital death (survivor/non-survivor) as the dependent variable and the conventional vital signs (HR, MAP, and SpO2) plus rSO2 as the independent variables. In our study, the variables selected for the statistical model were based on vital signs frequently used for risk assessment in critically ill patients during mobilization in the ICU. These indicators are considered essential elements for assessing physiological stability in severely ill patients and are often associated with prognostic evaluation [19, 20]. Specifically, HR, MAP, and SpO₂ are widely used as predictors of clinical outcomes in critically ill patients, and they formed the basis for our variable selection. These variables are crucial for evaluating the immediate physiological state of patients in critical care and for predicting long-term treatment outcomes.
Analysis 2: This analysis aimed to investigate the temporal changes in rSO2 and other vital signs during exercise.
Patients with interrupted measurements during mobilization were excluded, and the remaining patients were divided into the survival and non-survival groups. Patients who survived until discharge or who were transferred to another hospital were classified as survivors, whereas those who died in the hospital were classified as non-survivors. Patient characteristics, vital signs, and rSO2 before mobilization were compared between the two groups using the t-test and Mann–Whitney U or Fisher’s exact test. To investigate whether the patient groups in Analysis 2 and Analysis 1 were similar or not, the characteristics of the patients excluded from the analysis were compared with those of the patients included in Analysis 2.
Two-way repeated measures analysis of variance was conducted to investigate changes over time in vital signs and rSO2 associated with changes in the position during mobilization. Additionally, correlations between changes in vital signs and those in rSO2 at each of the six measurement points during mobilization were investigated by calculating Pearson’s correlation coefficients or Spearman’s rank correlation coefficients.
Because of the exploratory nature of this study, the sample size was not calculated in advance. All statistical analyses were conducted using EZR [21] (EZR on R commander version 1.54), a graphical user interface of R (The R Foundation for Statistical Computing, Vienna, Austria). A p-value of < 0.05 was considered statistically significant in all analyses.
Research ethicsThe Institutional Review Board of Uonuma Kikan Hospital approved this study (approval number 02–006). Informed consent was obtained from all patients or their families. The study team at Uonuma Kikan Hospital conducted the study in accordance with the principles of the Declaration of Helsinki. Additionally, a record was created in the University Hospital Medical Information Network before data collection (record number R000040749).
Comments (0)