Ureteral wall spasms caused by obstructing stones can interfere with successful stone passage. Significant inflammatory reaction with mucosal edema is common at the level of ureteral stone that may obstruct the ureteral lumen even with small stones leading to subsequent complications [16]. In the recent years, there has been a paradigm shift in the use of medical treatments to decrease ureteral peristaltic contractions while maintaining its tonic activities, which would allow distal propulsion of the stone [12, 17]. In the current NMA, we assessed the efficacy of different combination MET compared to α-blockers alone or each other. Our results revealed that combination MET with α-blockers, PDE5-Is, corticosteroids and phytotherapy increased the rate of SER 2.7 to 3.1 times more than α-blockers alone. Moreover, combination of nifedipine + corticosteroids seem more effective than corticosteroids alone. Regarding the expulsion time, statistically significant decrease in SET was found in combination of α-blockers and PDE5-Is compared to α-blockers alone or monotherapy groups. Finally, significantly less analgesia use was seen in the combination of α-blockers and PDE5-Is when compared to α-blockers and corticosteroids or α-blockers alone. In addition, combined nifedipine with corticosteroids showed significantly less MAU compared to α-blockers alone, α-blockers with corticosteroids, and monotherapy groups.
Given the high density of α1-adrenergic receptors in the distal ureter, different α-blockers with different uroselectivity have been used with the impression of inhibiting basal smooth muscle contraction and uncoordinated hyperperistaltic spasms, while maintaining intra-ureteral pressure gradient around the stone. Alfuzosin has no pharmacological uroselectivity while tamsulosin blocks the α-1 A and α1-D receptors, silodosin is highly selective for α-1 A receptor, and naftopidil has an effect on both α-1 A- and α-1D-receptors, but its affinity is approximately three-fold stronger for the α-1D-receptors than the α-1 A [2, 7, 16, 18, 27, 30,31,32,33,34]. While α1-D receptors are more abundant than α1-A, ureteral smooth muscle contraction predominantly relies on α1-A receptors, as evidenced by gene and protein expression profiles and contractile function analyses. This may explain why silodosin has demonstrated greater efficacy than tamsulosin for MET in the existing literature [18].
As mentioned earlier, PDE5-Is acts via the nitric oxide/cyclic guanosine monophosphate pathway, which leads to ureteral smooth muscle relaxation. Vardenafil is the most potent PDE5Is, and tadalafil is the least potent but more selective one [2, 10, 27, 32]. The concomitant use of PDE5-Is and α-blockers revealed better ureteral relaxation probably due to different pathways action on the ureteral smooth muscle contraction with significant pain control without adding significant side effects [3, 10]. In two studies by Kloner et el., the combination of tamsulosin and tadalafil was found to be safe [19, 20], as this was also shown in study by Bechara et al. [21]. Some studies reported that the prescription of tadalafil in patients with lower ureteric stone could provide another beneficial effect on improving erectile dysfunction when this problem coexists with ureteral stone [3]. In our NMA, combination MET of α-blockers and PDE5-Is had 2.7 more times higher SER together with significantly lower SET and analgesia use compared to α-blockers alone. Some patients had some degree of penile intumescence without any report of priapism [3, 10, 11, 15].
Early treatment with corticosteroids can result in decreasing the ureteral wall edema and inflammatory reactions at the site of stone impaction, which allows stone propulsion in the ureter [17, 22]. While some studies have demonstrated the benefit of combination MET with corticosteroids and α-blockers on SER [9, 23], the other clinical trials did not support this findings [17, 22]. Because of diversity in the prescribed steroid agents [22, 24, 25], lack of standard dosing and duration of the treatment, the evidence remains inconclusive to recommend its routine prescription in MET [22, 23]. Our studies revealed that combination MET with α-blockers and corticosteroids could significantly increase the expulsion rate (2.73 times) without lowering the expulsion time or increasing analgesia use.
Smooth muscle contraction in most tissues typically results from increased intracellular calcium. Studies show that calcium channel blockers like nifedipine reduce fast electrical activity in ureteral tissue but do not affect the basic peristaltic rhythm [3, 26]. Although early research on nifedipine for ureteral stone passage exists, most studies indicate it is less effective than tamsulosin and associated with more adverse events. However, in this study, the combination of nifedipine and corticosteroids showed better outcomes in SER compared to some treatments (such as miscellaneous monotherapy and Steroids), did not differ significantly from others, and was less effective than α-blockers + corticosteroids (Table 2). According to Table 3, while it was not significantly different from other treatments in terms of MAU, it still performed better than α-blockers alone, α-blockers + corticosteroids and miscellaneous monotherapy.
Few studies evaluated the effects of phytotherapy in combination with α-blockers. Rowatinex is a compound drug containing seven natural terpenes including pinene (31%), camphene (15%), borneol (10%), anethole (4%), fenchone (4%), and cineole (3%) in olive oil and has been introduced as MET for kidney stone management in the literature [27]. Phloroglucinol (1,3,5-Trimethoxybenzene) is a synthetic agent with weak anticholinergic properties, which selectively acts on smooth muscle fibers in a state of spasm, which was used as monotherapy MET in some studies [13, 28]. Bromelain is another phytotherapy composed of a mixture of proteolytic enzymes extracted from pineapple (Ananas comosus). It is known for its anti-inflammatory, antimicrobic, antithrombotic and fibrinolytic effects [29]. In the current study, combination MET with phytotherapy and α-blockers resulted 3.1 higher SER compared to α-blockers alone without significant effect on reducing the expulsion time.
The effect of various other combination MET protocols was also investigated in our study and showed considerable results on SER, SET and MAU. For example, the combination MET with nifedipine and corticosteroids seemed more effective than corticosteroids alone or other monotherapy groups in lowering SER. Corticosteroids alone had lower efficacy in SER compared to α-blockers alone. Expulsion time was significantly lower when α-blockers and PDE5-Is were compared to α-blockers alone or monotherapy with rowatinex, ketorolac or furosemide. Finally, analgesia use was significantly lower in α-blockers and PDE5-Is compared to α-blockers and corticosteroids or α-blockers alone.
Regarding the choice of combination therapy for distal ureteral stone passage, it seems that the use of α-blockers is recommended as an essential component because of its high specific effect on distal ureteral smooth muscle and low side effects as well as their supportive evidences in different combination groups. However, choosing the PDE5-Is, corticosteroids, or phytotherapy for combination with α-blockers should be individualized according to the patient’s status, preferences and side effect profiles. For example, corticosteroids have received increased attention as a potential useful adjunct in first week of MET [9], however, their side effects should be considered. PDE5-Is could be a reasonable choice, especially in patients with simultaneous erectile dysfunction, and phytotherapy can be based on patient’s preference. Combination nifedipine or diuretics with α-blockers require further investigation based on our understanding of the current data.
It is worth mentioning that MET for ureteral stones has become controversial due to conflicting results from recent high-quality trials and meta-analyses. While guidelines and reviews support MET, robust randomized clinical trials often show minimal evidence of benefit. These discrepancies may arise from broad inclusion criteria or insufficient power for subgroup analyses, highlighting the need for detailed study evaluations [30,31,32,33].
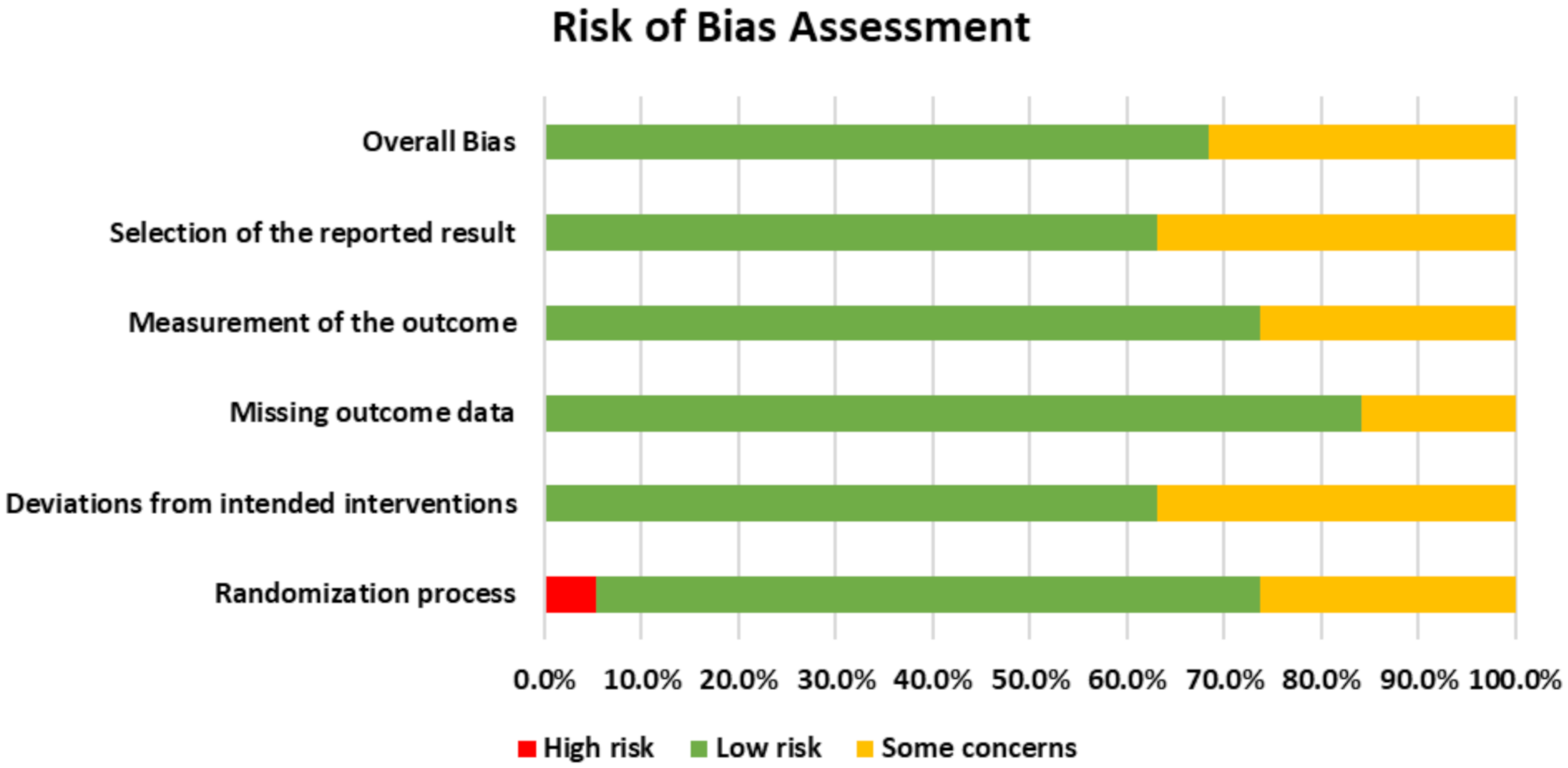
One of the limitations of this network meta-analysis is the scarcity and inconsistency of the data on analgesic use in the primary studies. Some studies did not report about the type and dosage of consumed analgesic Moreover, various analgesic treatments with different doses have been prescribed to the patients in other studies, that it was not possible to include them for assessment of MAU analysis. The heterogeneity of the data made it difficult to compare and combine the results across the studies and to draw reliable conclusions about the effectiveness of the treatments. Second, a few included studies did not have enough descriptions regarding randomization, conceal allocation, and blinding, which may lead to synthetize unreliable evidence. And finally, we found only a limited number of studies include combination of nifedipine or phytotherapy agents with α-blockers or PDE5-Is.



Comments (0)