Ethical approval and consent
This study was conducted following the principles outlined in the Helsinki Declaration and its subsequent amendments. Ethical approval for the study was received from the Clinical Research Ethics Committee of the School of Dentistry, Marmara University, on 27.12.2023, with protocol number 08.12.2023.1763. All necessary written permissions regarding the study were obtained from the institution where the study was conducted and all related official authorities. Details about the study were explained to the participants verbally and in an appropriate language by the researchers. Subsequently, those who consented to participate in the study were requested to read and sign the consent forms, which provided detailed information about the study. In addition, consent for participation was obtained from the responsible legal guardians of orphan children and adolescents in the residential care facility.
Sample size calculation
The sample size was calculated using the G*Power statistical software (version 3.1.9.7, Universitat Kiel, Kiel, Germany). Based on the data reported by Khattab et al. [23], which demonstrated that the total DMFT scores were 0.75 ± 1.29 for non-orphan children compared to 1.80 ± 2.54 for institutionalized orphan children (p = 0.025), a minimum total sample size of 108 was determined to be sufficient. This calculation was performed to achieve a statistical power of 85%, with a significance level (α) of 0.05 and an effect size of 0.5212443.
Study population
A total of 112 Turkish male orphan children and adolescents, aged between 9 and 17 years, living in the same and single residential care facility in Istanbul, Türkiye, affiliated with Ministry of Family and Social Services of Republic of Türkiye, were included in this cross-sectional study. Children and adolescents who did not provide informed consent to participate in the study or failed to cooperate during the intraoral examination were excluded from the study.
In Türkiye, the residential social service model is implemented within each province’s social, cultural, and physical context, as well as in regions suitable for child-rearing, to ensure that children and adolescents under protection are cared for in smaller, more supportive units. The main aims of this model are to ensure that orphan children and adolescents under protection learn concepts such as friendship and neighborhood, understand the requirements of life in society, and become self-confident individuals who can look to the future with hope. Accordingly, children and adolescents who spend their lives as boarders in these institutions consume similar meals in the same institution. Educational processes are coordinated by various trainers and caregivers, with necessary support provided as needed. Institution officials coordinate with other authorities to meet the psychological, physiological, and sociological needs of the children. Caregivers, nurses, and other staff are responsible for controlling and supporting children in matters such as brushing their teeth, determining their treatment needs, personal hygiene, and nutrition [26].
Data collection
After obtaining the necessary permissions, the residential care facility administration was informed about the date of the visit one week in advance. The facility administration provided preliminary information to orphan children and adolescents. On the day of the visit, all orphan children and adolescents living in the facility were invited to the institution’s meeting hall. In this hall, the researchers provided information about the study to the participants with a visual presentation. During this presentation, explanations were made to the participants in a style appropriate to their ages and sociological conditions. Questions from the participants regarding the study were collected and answered. The children and adolescents who agreed to participate in the study were examined intraorally in a mobile examination section set up in a separate part of the meeting hall. The sociodemographic information of the participants and the findings from the intraoral examination were recorded on pre-designed forms. A validated questionnaire assessing OHRQoL was administered to participants following the completion of their intraoral examinations. After expressing gratitude to the participants, information regarding diagnosed systemic diseases and medications for the orphan children and adolescents was obtained from the responsible nurses and documented in the participant files.
Intraoral examination
Two pediatric dentists (N.A. and N.H.) conducted the intraoral examinations. Prior to the study, a calibration process was carried out to ensure consistency in diagnoses. Fifteen children and adolescents, who were not included in the study, were examined twice by both researchers under identical conditions, with a one-month interval between examinations. During the calibration, one of the researchers acted as the gold standard to provide a reference for consistency in diagnoses. Cohen’s kappa statistics were calculated to assess inter- and intra-examiner reliability for dental caries diagnosis, oral hygiene assessment, and evaluation of treatment need. The results demonstrated strong agreement, with kappa values exceeding 0.8 for inter- and intra-examiner reliability.
A common flat-surface mouth mirror (#5) was used for visual diagnosis during intraoral examinations. Standard dental probe #PCP11 was used for tactile inspection, and standard periodontal probe #PCPUNC15 with a millimeter scale was used for periodontal and gingival assessments.
Dental caries evaluation was conducted utilizing the decayed, missing, and filled teeth (DMFT/dft) index, with the dft index applied to primary dentition and the DMFT index to permanent dentition. Within these indices, a tooth is classified as carious (D/d component) if a cavity is visibly present, including untreated dental caries. The missing (M component) category encompasses teeth with extraction indications or those removed due to dental caries, while the filled (F/f component) category includes teeth restored due to dental caries. The DMFT/dft index is recommended by the World Health Organisation (WHO) and is widely used in population-based, cohort, and cross-sectional studies due to its simplicity, validity, reliability, ease of use, and statistical utility [27, 28]. Following the dental caries examination, a restorative care index and an unmet treatment needs index were calculated for each participant [23]. The Restorative Care Index was calculated using the formula [F / (D + M + F)] × 100, representing the proportion of restored teeth relative to the total number of decayed, missing, and filled teeth. The Unmet Treatment Needs Index was calculated using the formula [D / (D + F)] × 100, indicating the proportion of untreated decayed teeth relative to the total number of decayed and filled teeth.
Participants’ oral hygiene was assessed using the Simplified Oral Hygiene Index (OHI-S), which is calculated by combining the Simplified Debris Index (DI-S) and the Simplified Calculus Index (CI-S). To determine the OHI-S, six surfaces were inspected, chosen from four posterior teeth and two anterior teeth (for primary dentition: buccal surfaces of teeth: #54, #61, and #64, lingual surfaces of teeth #82, #75, and #85; for permanent dentition: buccal surfaces of teeth #11, #16, #26, and #31, lingual surfaces of teeth #36 and #46). Score 0 means “no debris or stain present” for DI-S and “no calculus present” for CI-S. Score 1 means “soft debris covering not more than one third of the tooth surface, or presence of extrinsic stains without other debris regardless of surface area covered” for DI-S and “supragingival calculus covering not more than one-third of the exposed tooth” for CI-S. Score 2 means “soft debris covering more than one third, but no more than two third, of the exposed tooth surface” for DI-S and “supragingival calculus covering more than one-third but not more than two-thirds of the exposed tooth surface or the presence of individual flecks of subgingival calculus around the cervical portion of the tooth” for CI-S. And, score 3 means “soft debris covering more than two thirds of the exposed tooth surface” for DI-S and “supragingival calculus covering more than two-thirds of the exposed tooth surface or a continuous heavy band of subgingival calculus around the cervical portion of the tooth” for CI-S. The cumulative values from the scoring of debris and calculus on the buccal and lingual/palatal surfaces of selected teeth are averaged by dividing by the total number of surfaces scored. This calculation gives the subject’s DI-S and CI-S scores. Oral hygiene status is represented by the OHI-S score, calculated as summary of the DI-S and CI-S scores. A decrease in the OHI-S score indicates improved oral hygiene [29].
The Treatment Need Index (TNI), which identifies the realistic treatment requirements independent of the underlying cause (dental caries, trauma, and/or periodontal disease) was employed to evaluate dental treatment needs. TNI offers valuable insights that inform oral health planning. The index idenitifes seven fundamental levels of treatment. Code 0 means “no treatment needed”, code 1 means “preventive treatment (topical fluoride applications etc.) needed”, code 2 means “fissure sealants needed”, code 3 means “initial conservative restorations (one-surface restorations, preventive resin restorations etc.) needed”, code 4 means “moderate conservative restorations (one or two-surface restorations etc.) needed”, code 5 means “advanced conservative restorations (three or more-surface restorations, stainless steel crowns etc.) needed”, and code 6 means “radical treatment (endodontic, prosthetic, and/or surgical methods etc.) needed”. In this index, the number and percentage of teeth in each category are recorded for each participant [30].
Measurement of oral health related quality of life
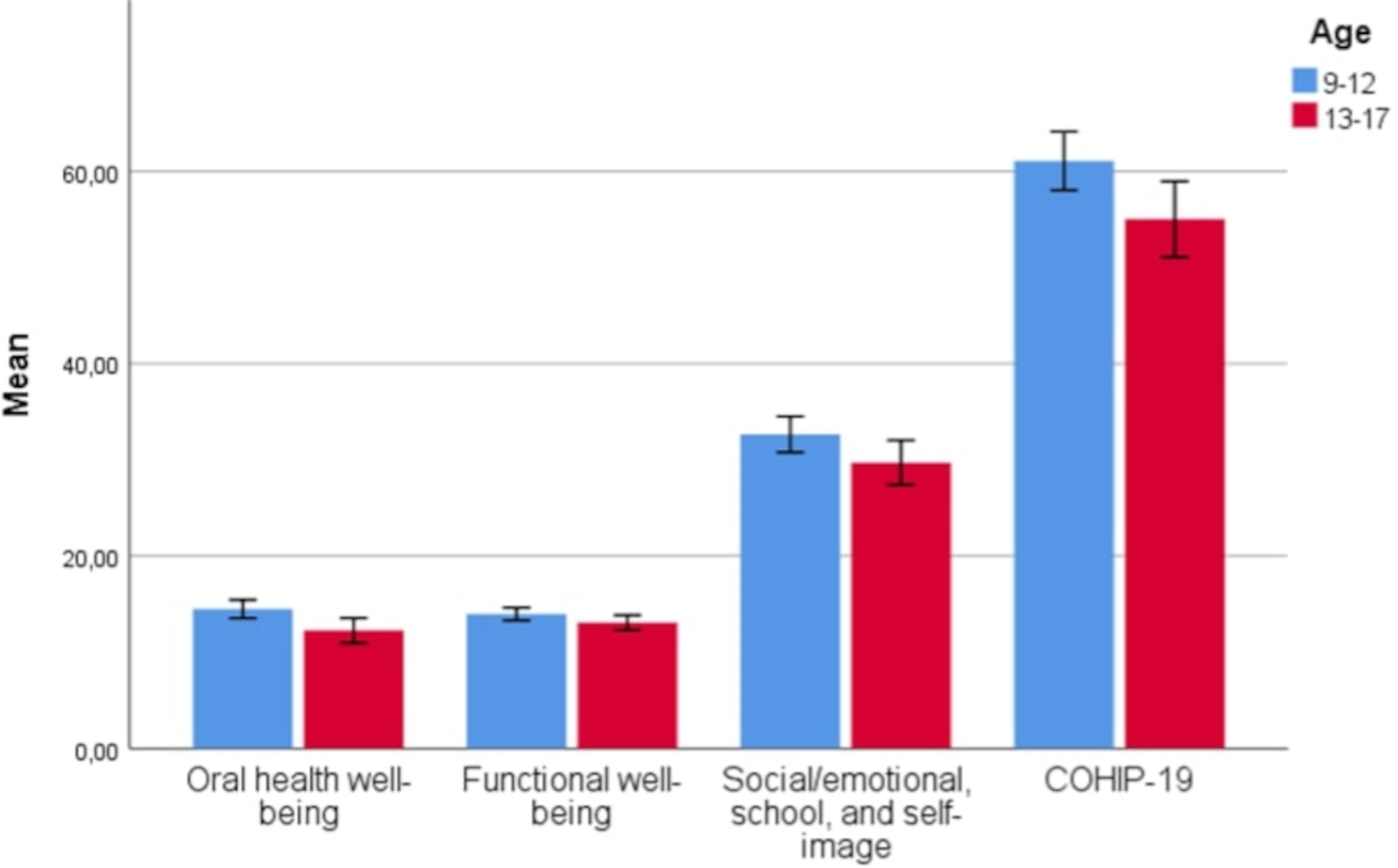
In the current study, the Child Oral Health Impact Profile-Short Form (COHIP-SF-19) questionnaire, comprising 19 questions, was employed to assess the OHRQoL of the orphan children and adolescents. The validity and reliability of the COHIP-SF-19 were assessed specifically for the age group of the study participants and adapted for the Turkish language [31].
The questionnaire efficiently assesses the child’s overall OHRQoL across three domains: oral health, functional well-being, and socio-emotional well-being, school environment, and self image. Oral health domain is a section where various oral health symptoms (toothache, tooth discoloration, etc.) that are not necessarily related to each other are scored. Functional well-being domain includes items related to the child’s ability to perform specific tasks and activities related to the mouth (speaking, chewing, etc.). Socio-emotional well-being, school environment, and self-image domain includes statements that evaluate the child’s peer interactions, mood state, factors related to the school environment, and positive feelings about oneself [32]. Participants were asked to evaluate the items using a five-point Likert scale with numerical values: 0 = never, 1 = almost never, 2 = sometimes, 3 = fairly often, and 4 = almost all the time. Negative questions (first 17 questions) are reverse scored: 0 to 4, 1 to 3, 2 to 2, 3 to 1, and 4 to 0. After re-coding, the maximum of score is 76, indicating a higher quality of life in the context of oral health [32, 33].
Statistical analysis
The demographic, health-related, dental, and OHRQoL-related data collected from the participants were recorded in Microsoft Excel 2016 (Microsoft, Redmond, WA, USA). The statistical analysis of the data was conducted using the Statistical Package for the Social Sciences (SPSS Version 25.0, IBM Corp., Chicago, IL, USA). Normality of variables was assessed using the Shapiro-Wilk test and homogeneity of variance was assessed using the Levene test. Quantitative data are presented as mean ± standard deviation, median, and minimum and maximum values. ANOVA (Analysis of Variance) test was used to compare three or more independent groups with normal distribution and Kruskal Wallis test was used for data without normal distribution. Post hoc Bonferroni tests, including the Bonferroni correction, were performed to identify the group or groups responsible for the differences. The relationships between variables exhibiting non-normal distribution were assessed using the Spearman’s rank correlation coefficient. Kendall’s Tau Correlation was used to examine the relationships between ordinal and continuous measurements. For detailed analyses, participants were divided into two groups as 9–12 years old and 13–17 years old to define late mixed dentition and permanent dentition. A stepwise multivariate linear regression analysis was used to examine the impact of clinical characteristics of participants aged 13–17 on their total COHIP-SF-19 scores. p < 0.05 was considered statistically significant.




Comments (0)