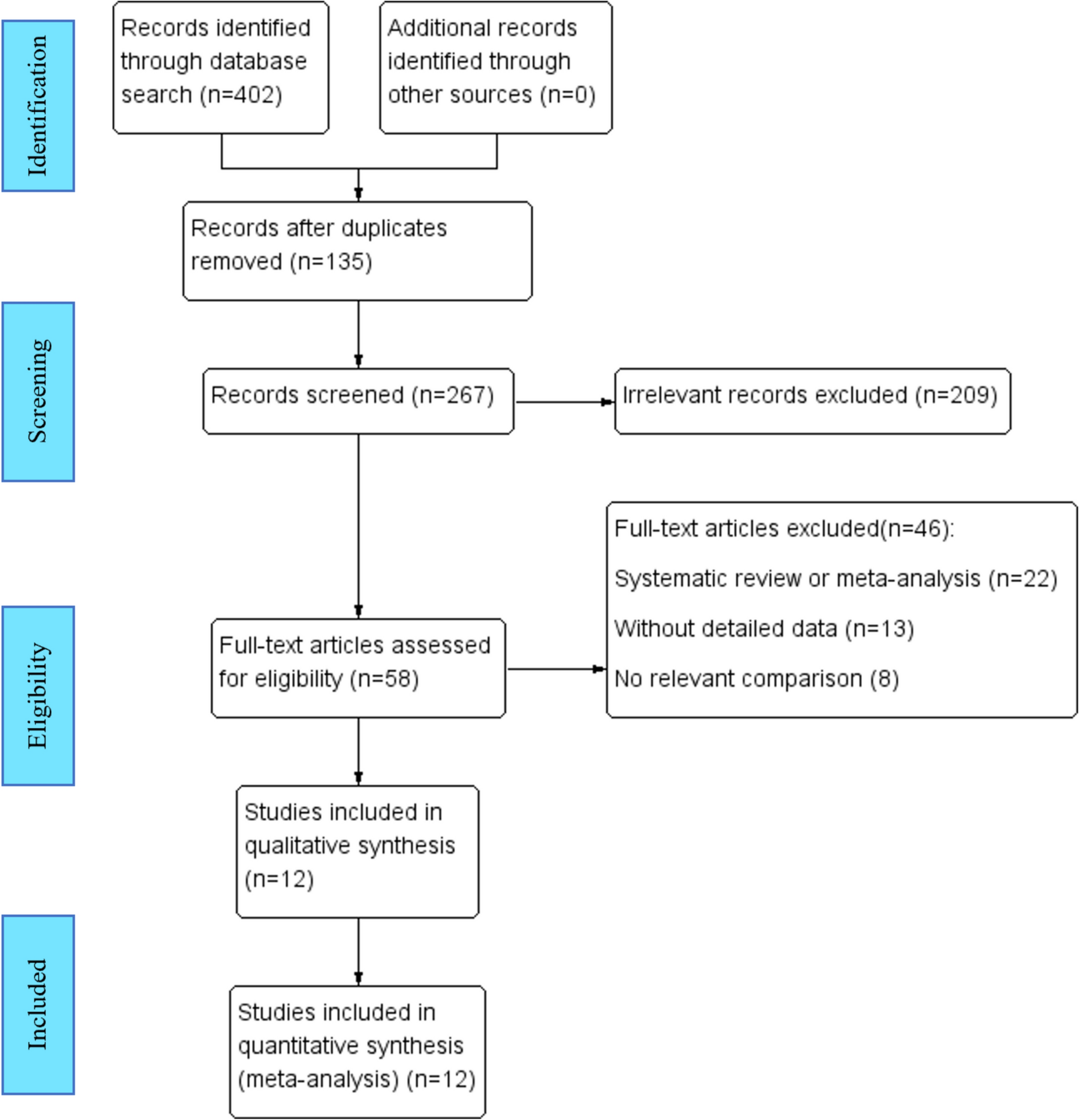
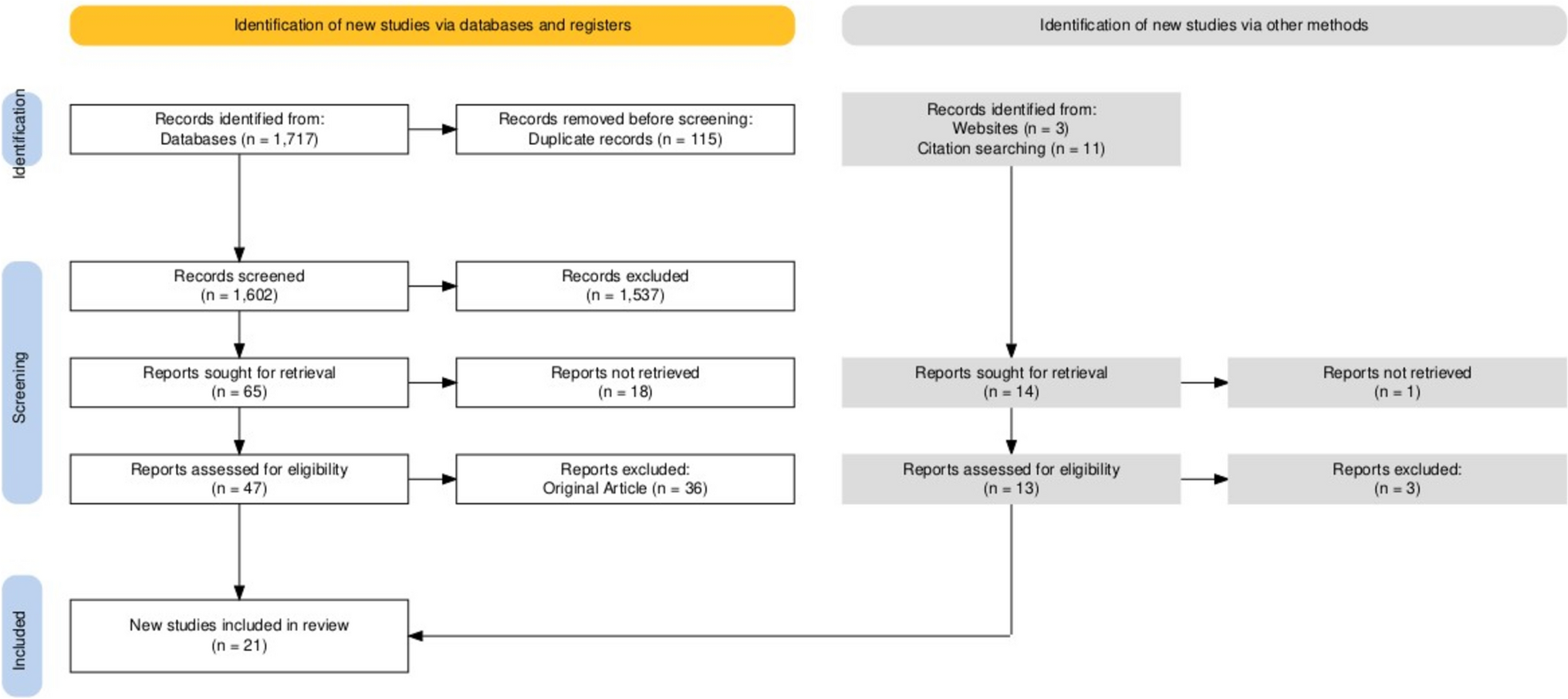
This is the first comprehensive evaluation and meta-analysis that, to our knowledge, compares LAP with other surgical approaches. 20 studies comparing the laparoscopic method to the open, retro-muscular, or robotic-assisted approaches involved 16,247 patients in total.
Ventral hernias are described as the protrusion of a part of a tissue or an organ via a weakness in the abdominal wall. Following abdominal wall surgery, this hernia incidence might reach 13%. An incisional hernia following a procedure on the abdominal wall is considered morbidity. These hernias are more likely to occur when certain risk factors are present, including wound infection, obesity, male sex, abdominal distension, occasionally inadequate surgical closure, and underlying disease processes. Nearly 350,000 ventral hernia repairs (VHR) are thought to be done yearly in the USA alone, at a cost of over $3 billion [28]. Previous studies have shown that VHR may contribute to total cost losses for healthcare systems [28].
In an effort to improve the value of care, surgeons have looked for ways to decrease the risk of hernias in patients undergoing initial abdominal operations as well as to lower intraoperative costs, improve patient outcomes, and shorten the length of stay (LOS) for patients undergoing VHR [26]. Incisional hernia incidence after midline laparotomy varied from 11 to 20% following a mean follow-up of between 12 and 20 months. After incisional hernia repair, incisional hernias have a significant recurrence risk. After open mesh surgery, the recurrence rate of hernia varied from 6.8 to 32.1%, while following laparoscopic repair, it ranged from 0 to 12.3%. Due to the high likelihood of recurrence following incisional hernia repair, both anatomical and prosthetic repairs have been tried. With a high recurrence frequency of roughly 30–50% following anatomical repair and 1.5–10% following prosthetic mesh repairs, the outcomes have been dismal. With the notion of tension-free mending, prostheses have transformed hernia surgery. Even though many different surgical techniques have been used to treat incisional hernias, prosthetic mesh implantation is still the most effective treatment option. Both the preperitoneal plane formed between the rectus muscle and posterior rectus sheath (sublay mesh repair) and the subcutaneous abdominal wall tissues and the anterior rectus sheath (onlay mesh repair) are suitable locations for the prosthetic mesh. The latter method has a number of benefits, one of which is that it rests relatively deeply in the preperitoneal plane and prevents infection from spreading from subcutaneous tissues down to the mesh [5].
Using a prosthetic mesh in a tension-free repair is the gold standard for treating ventral/incisional hernias. The open repair of a hernia may now be performed with this technique, or as an alternative, a laparoscopic approach can be used [29]. In comparing mesh-based repair to suture-based repair, an analysis of several incisional hernia repair approaches along multiple outcome characteristics suggests that mesh-based repair gives a superior choice. The main issue is the cost involved and the increased danger of infection brought on by the implantation of a foreign body. The considerable dissection and tissue manipulation involved in hernia surgery have been widely blamed for postoperative problems, including seroma development, hematoma, cellulitis, and wound infection [1, 28]. Mesh repair has a higher intraoperative blood loss rate and longer operating duration. These two elements have reportedly been linked to a rise in wound infection [1]. A large overlap of around 5 cm over the hernia defect in all directions with the mesh positioned in the preperitoneal, retro-muscular region was first used in the late 1980s. When this technique was improved, the recurrence rates dropped to as low as 3.5%, and it was deemed the standard of treatment for ventral hernias [1, 28].
The basic tenets of the open retro-muscular (preperitoneal) repair that Stoppa and Rives describe, which call for positioning the mesh in this plane, offer several benefits [25]. Furthermore, since the mesh is retro-muscular in a deeper plane, any infection in the subcutaneous plane has no effect on it because of how highly vascular this plane is. The preperitoneal method enables a uniform distribution of pressures throughout the mesh's surface area. This explains the robustness of the repair and the related reduction in recurrence. The posterior rectus sheath is attached to by the prosthesis, rendering it inextensible and preventing additional herniation, dislodging, or rupture due to intra-abdominal pressure. Instead, the force that produced the hernia holds the prosthesis in place [25, 28].
The laparoscopic intraperitoneal onlay mesh (IPOM) technique quickly gained popularity after the first report of laparoscopic ventral hernia repair published by LeBlanc et al. in 1993 since it resulted in a quicker recovery and less severe wound problems [18]. They provided evidence of the benefits of laparoscopic hernia repair over open surgery, with better outcomes and reduced complication rates. With the full loss of abdominal muscular structure, the only condition currently regarded as unfavourable for a laparoscopic technique is a major tissue defect. However, despite the fact that the hernia repair procedure has evolved in the last 20 years with regard to general methodology, many specialists still find the results to be subpar. Recurrence rates for incisional hernias treated with a primary suturing range from 12 to 54%, whereas they might reach 36% with mesh repairs. Furthermore, introducing foreign bodies like the Prolene mesh can have major negative effects like discomfort, fistula, infection, bowel adhesions, and bowel damage. The production aspects of the most recent mesh product types have been given greater thought in order to minimise the issues outlined above. Since that time, laparoscopic repair has been frequently used like a reliable alternative for open hernia surgery [2, 25].
The minimally invasive laparoscopic method involves a few stab-like incisions to allow the usage of laparoscopic equipment. Instead of fixing the fascial defect, the procedure involves covering it with mesh, either with or without shrinking the hernia sac. For a safe procedure with fewer risks, such as seroma, infection, haemorrhage, and intestinal damage, a thorough dissection is essential. According to some publications, laparoscopic incisional hernia repair yields improved results compared to open surgery since the recurrence rate is much lower (4.3%), and there are fewer wound complications [3]. A large overlap of around 5 cm over the hernia defect in all directions with the mesh positioned in the preperitoneal, retro-muscular region was first used in the late 1980s. It was deemed the standard of therapy for ventral hernias as the refining of the procedure reduced recurrence rates to as low as 3.5% [28].
Laparoscopic incisional hernia repair has purportedly demonstrated improved results with respect to postoperative complications and hernia recurrence. Wound complication rates can be as low as 38%, and recurrence rates can be as low as 43% during a 25-month follow-up period, according to a meta-analysis of several non-randomized comparative studies and case series. The laparoscopic approach provides minimally invasive access to the abdominal cavity. It allows for the placement of a prosthetic deep inside the abdominal tissue. A laparoscope is utilized to view the abdominal cavity and assist in the placement of the prosthesis after making several tiny incisions in the abdominal wall far from the hernia. Often, the hernia sac is left alone, and sutures, tacks, or a combination of the two are used to anchor the mesh in place. With this approach, the surgical insult is reduced. Additionally, it makes the defect more visible, including any secondary hernia flaws that are smaller and might not be seen clinically. As a result, the prosthesis may be placed more precisely with consistent fascial overlap. The limited amount of dissection needed might also lessen the chance of problems, including infection, gut wall damage, bleeding, and seroma development [28]. There were fewer wound infections with laparoscopy, according to a recent meta-analysis of ten published randomised, controlled studies comparing the open to laparoscopic technique [30]. Even without taking into account patient advantages like early hospital release and return to work, cost–benefit analyses have shown laparoscopic incisional hernia surgery to be equally expensive as open incisional hernia repair [3].
Surgery is required to treat an incisional hernia in 80% of patients. More than 20% of open incisional hernia repairs result in morbidity, including mesh infection and recurrence. Surgery is required to treat an incisional hernia in 80% of patients. More than 20% of open incisional hernia repairs result in morbidity, including mesh infection and recurrence. In general, laparoscopic surgery is risk-free and linked to fewer infections and a shorter hospital stay. Due to the incisional hernia's good exposure in obese individuals, it is quite practical. The surgical treatment, however, might be challenging, and it can take more time. It has not yet been determined which course of action is ideal for treating incisional hernias. A more well-defined treatment plan may have advantages, including a shorter hospital stay, lower costs, and fewer postoperative problems [31]. According to two recent meta-analyses, laparoscopic repair is as successful as open surgery and may even be superior in some cases [1, 28]. Less postoperative problems were seen, and the overall hospital stay was shorter.
According to a recent meta-analysis, incisional hernias following midline abdominal incisions are anticipated to occur 13% of the time at 2 years following the first operation, and approximately 80% of patients would ultimately need another procedure. Since its original description in 1993, laparoscopic incisional ventral hernia repair (LVHR) has been proven to be both secure and effective. Additionally, several surgical teams have begun inserting intraperitoneal mesh through trocar ports to address abdominal wall defects. Recent systematic reviews support the LVRH approach’s effectiveness and safety, but they also highlight the dearth of research that looks at the quality of life over the long term [8, 28].
Laparoscopic and open repairs for hernias did not vary in hernia recurrence, according to a meta-analysis. In six of the eight included trials, though the hospital stay length was shorter after laparoscopic surgery, the difference in operation time remained ambiguous. Fewer wound infections were linked to laparoscopic hernia repair [28]. Incisional hernias were substantially less common in the laparoscopic group, according to another meta-analysis. Additionally, the laparoscopic group’s wound infections were much lower than those in the open group, and both groups’ total postoperative morbidity was comparable. Compared to laparoscopy, open abdominal surgery resulted in a noticeably longer hospital stay [5]. According to Zhang et al. [2], investigations revealed that the laparoscopic group had a shorter hospital stay duration than the open group, and wound infection occurrences were considerably lower in the laparoscopic group compared to the open group (laparoscopic group 2.8%, open group 16.2%). Al Chalabi et al. compared laparoscopic versus open abdominal incisional hernia repair for effectiveness and safety [3]. They found that the recurrence rate was comparable, the length of hospital stay was not statistically different, wound infection was higher in the open repair group, and laparoscopic surgery took more time. Sains and colleagues examined data from 351 patients who were participants in five studies and discovered that the laparoscopic procedure resulted in a 12 min longer operating time that was and a 3–3 days shorter hospital stay; no difference was there in the wound infection rates or hernia recurrence rates [32]. One-fourth of mesh repairs and nearly half of all initial repairs fail after three years, according to a randomised, multicentre research. Additionally, using prosthetic materials increases the chance of serious wound complications, which in and of itself is a risk factor for hernia recurrence and additional morbidity [4].
The included studies included a substantial amount of heterogeneity, which was one of the study’s limitations. Due to the fact that none of the included studies were double-blinded, research bias is the first potential factor contributing to heterogeneity. Confounding factors, such as various hernia locations and sizes, patients with various surgical risks, and various meshes, are the second potential reason for heterogeneity. The fact that there was a sizable difference in operating methods between the trials is a second restriction.
While our systematic review compares laparoscopic IPOM procedures to open retro-muscular approaches, we recognize that recent advances in hernia surgery, including as laparo-endoscopic and robotic-assisted techniques, have moved the field's emphasis. However, most of the papers that satisfied our inclusion criteria focused on standard laparoscopic IPOM and open retro-muscular methods. This limitation reflects the condition of the literature at the time we conducted our review.
We understand that comparing IPOM to retro-muscular techniques may no longer adequately convey the intricacies of modern hernia repair strategies. As such, the findings given here should be taken into consideration the existing evidence. Future research is needed to make a more thorough comparison of emerging procedures, such as laparo-endoscopic and robotic retro-muscular repairs, with open repairs. This will be critical for guiding future clinical practice and improving surgical techniques.

Comments (0)