
Remember me


Chondroblastoma is a benign but locally aggressive cartilage-forming tumour of long bones. It is classically seen arising from the epiphysis of long trabecular bones in skeletally immature patients [1, 2].
A periosteal or surface-based chondroblastoma arising independent of the epiphysis is quite unique and an extremely rare entity, with only a few reported cases in the literature [3,4,5,6,7,8,9,10,11,12,13]. In 2002, Ishida et al. described the first case of an intracortical chondroblastoma in the distal femur of a 19-year-old with insidious knee pain [5]. Subsequently similar lesions have been described in the distal femoral metaphysis [6], distal tibial diaphysis[10], proximal tibial metaphyseal[11], tibial diaphysis [12] and in the femoral neck [13]: Our case represents yet another addition to this rare entity of an extramedullary surface-based chondroblastoma.
The exact pathogenesis of surface-based chondroblastoma remains unclear. However, it may involve neoplastic transformation of chondrocyte precursors displaced from the physis during prenatal or postnatal development (Figs. 1, 2, 3, 4, 5, and 6).
Fig. 1
Antero-posterior(AP) radiograph of the left knee shows a radiolucent juxta cortical lesion along the proximal lateral tibial margin causing saucerization of the adjacent lateral tibial cortex and secondary solid periosteal reaction
Fig. 2
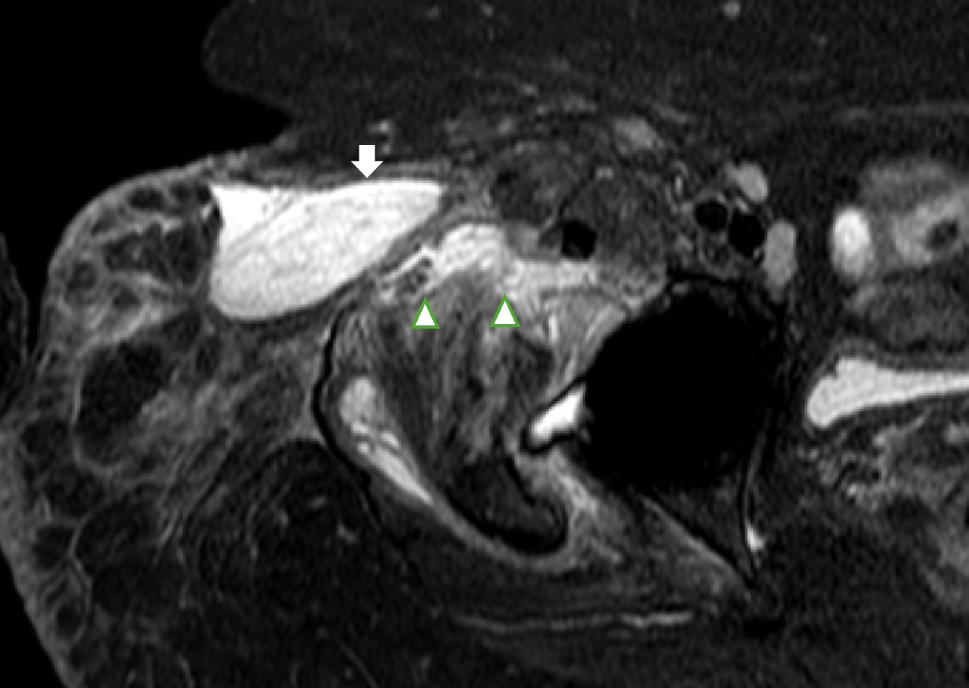
Coronal T1 (A), coronal PD-w fat-saturated MR sequences of left knee showing a hyperintense juxta-cortical solid mass-producing cortical pressure erosion and surrounded by sclerotic rim
Fig. 3
Coronal CT images of the left knee showed a juxtacortical lesion along the lateral margin of the proximal left tibia with few subtle chondroid calcification within and causing saucerization of the lateral tibial cortex and a peripheral sclerotic rim and periosteal reaction
Fig. 4
Axial CT showing biopsy needle placement targeting the juxtacortical lesion along the lateral margin of the left proximal tibia
Fig. 5
a Haematoxylin and eosin-stained and b immunohistochemistry images following CT guided biopsy shows features shows features of chondroblastoma consisting of sheets of ovoid to polygonal cells which have eosinophilic cytoplasm and small grooved nuclei. Foci of eosinophilic chondroid matrix and multinucleated giant cells are seen. The mononuclear cells are positive for H3F3 K36M, which is a specific marker for chondroblastoma
Fig. 6
A Immediate and B 1-month post-operative radiographs showing resection of the left sided juxta-cortical lesion along the proximal left tibia. C Coronal PD-w sequences showing resection of the juxta-cortical lesion along the proximal left tibia
Radiologically, periosteal chondroblastoma presents as a well-defined, cortically based mass with variable intrinsic “chondroid”-pattern mineralisation. An associated periosteal reaction is common, ranging from solid buttressing to an interrupted Codman triangle or even sometimes an aggressive “hair-on-end” type appearance. Computed tomography (CT) helps delineate the lesion’s surface origin and the intrinsic “chondroid”-pattern matrix mineralisation. MRI helps to further characterise the lesion by demonstrating the extent of the lesion’s intraosseous and extraosseous involvement. Extensive marrow and soft tissue oedema are frequently seen with a more sinister pathology like chondrosarcoma.
The imaging differentials of periosteal chondroblastoma include Periosteal chondroma, periosteal chondrosarcoma, and high-grade surface osteosarcoma. Periosteal chondroma classically appears as a well-circumscribed juxtacortical lobulated osteolytic lesion with a thin periosteal shell and saucerization of the adjacent cortex and buttress periosteal reaction. However, unlike chondroblastoma, chondromas lack a prominent periosteal reaction and exhibit variable intralesional matrix calcifications. Periosteal chondrosarcomas and osteosarcomas are usually larger, more aggressive-looking lesions and primarily present with marked pain and swelling. They have extensive intramedullary involvement and bone marrow oedema. High-grade surface osteosarcoma is a broad-based, extensively mineralised mass with an aggressive sunburst periosteal reaction and a more extensive soft tissue component.
Histologically, chondroblastoma is characterised by sheets of uniform, round to polygonal mononuclear cells with a “coffee-bean”-pattern nuclei with an eosinophilic chondroid matrix with fine, lace-like “chicken-wire” calcifications. H3F3 K36M is a sensitive and specific marker for chondroblastoma [14, 15]. Secondary aneurysmal bone cyst changes may occur in up to one-third of cases.
The treatment of periosteal chondroblastoma consists of thorough intralesional curettage or wide surgical resection. The prognosis is usually excellent after complete removal; however, long-term follow-up is advised as these lesions are quite rare and have scant published literature.
Ours was an interesting and rare case of an extramedullary surface-based chondroblastoma. The learning point is that radiologists should consider periosteal chondroblastoma in their differential diagnosis for any surface tumour in a young patient. Awareness of this entity can prevent diagnostic delays and avoid inappropriate treatment. Management parallels that of classic chondroblastoma, with complete surgical excision being curative.
Comments (0)