
Remember me
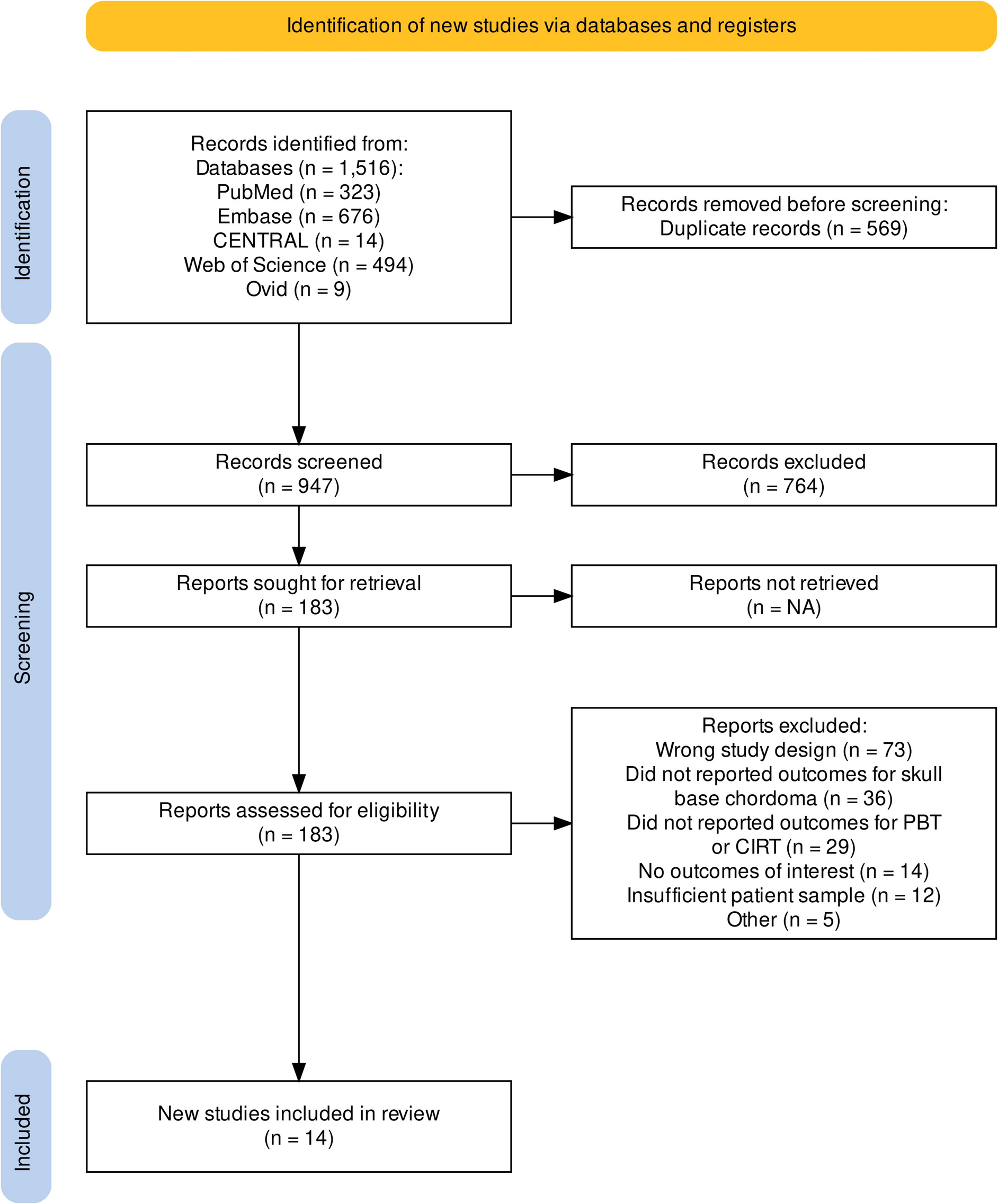
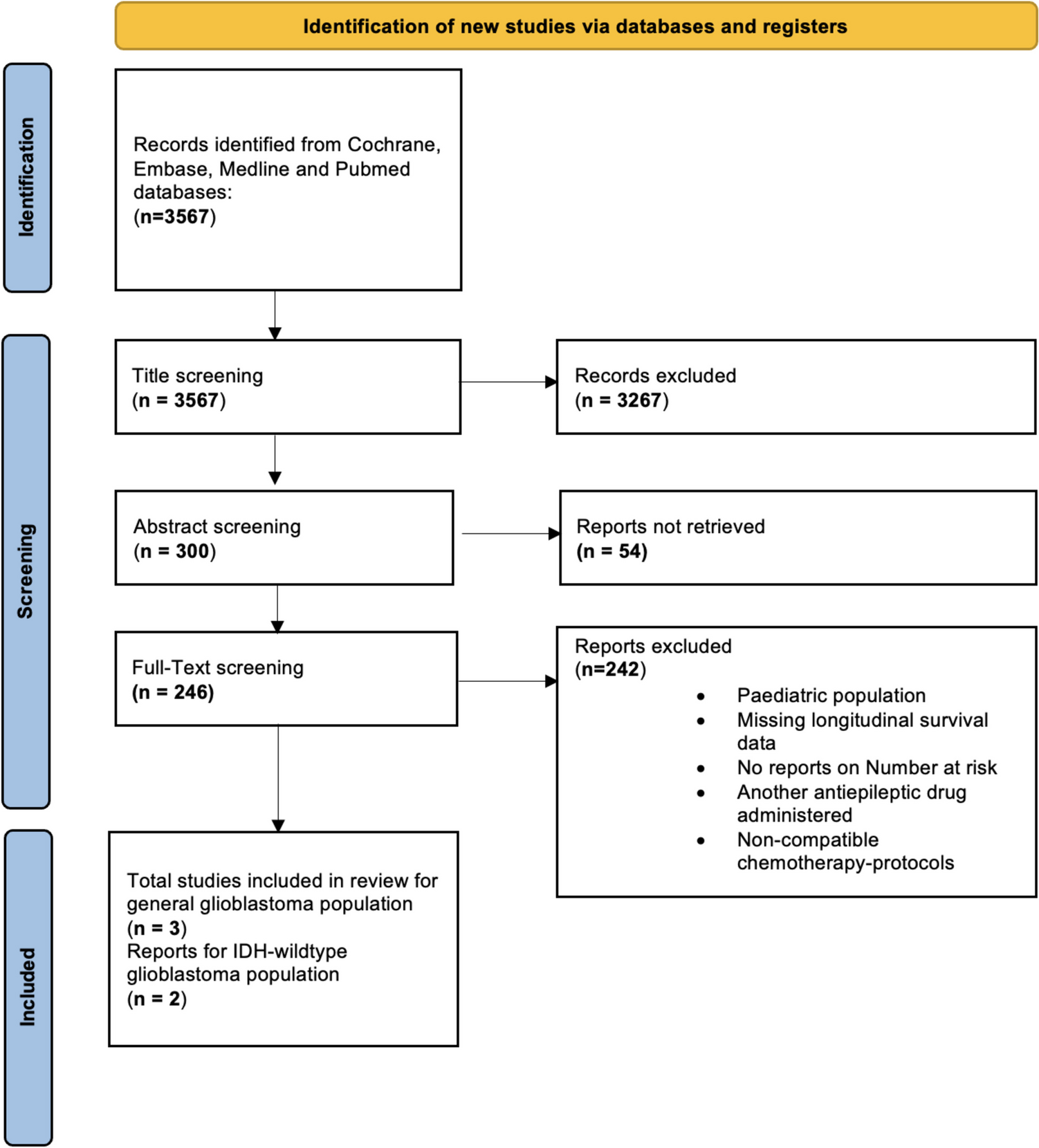
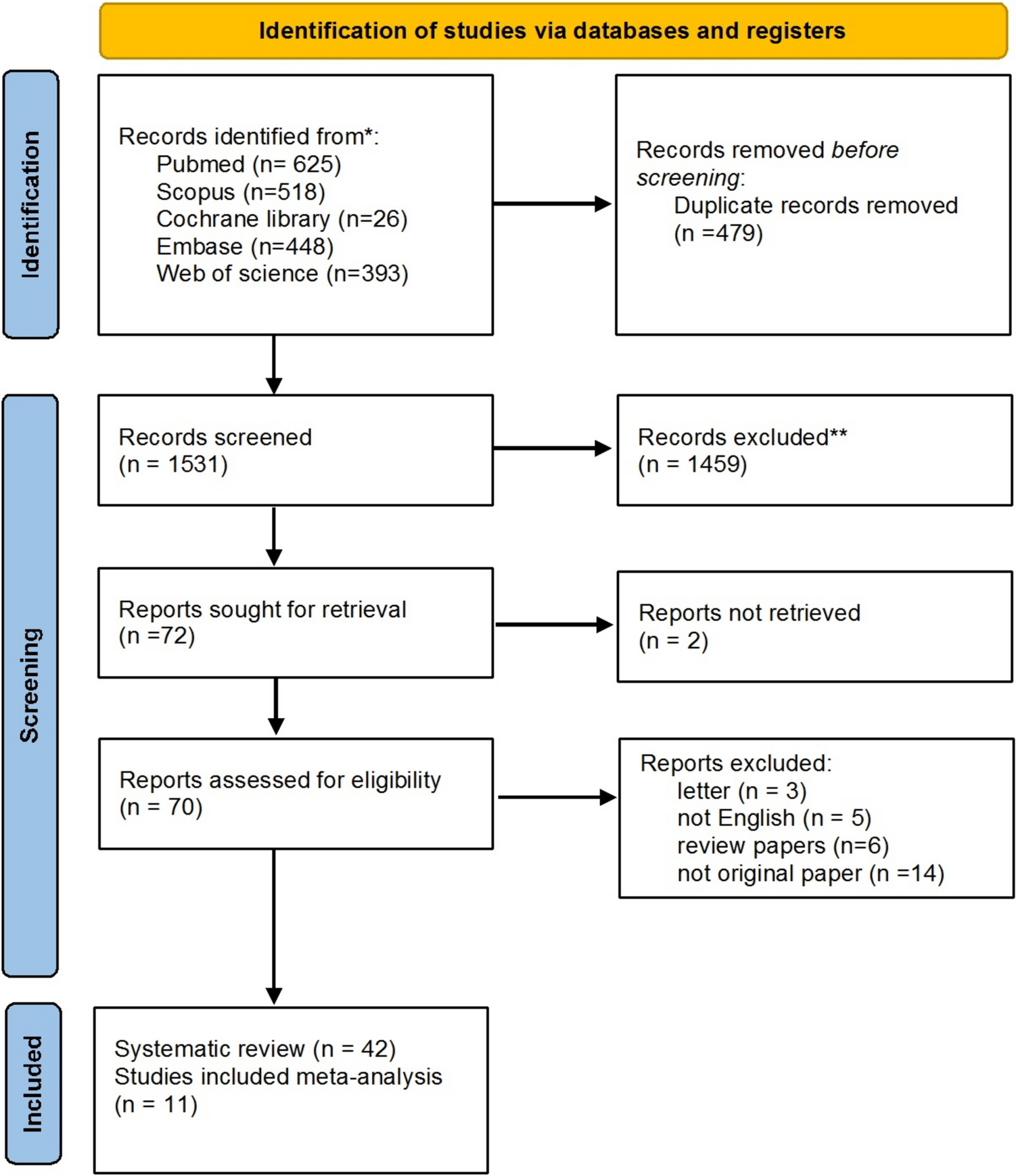
Our search yielded 2,251 unique articles regarding the use impedance probes or ECoG in intraoperative brain tumour monitoring. Seven further articles were found via citation searching of included articles. Following application of the exclusion criteria, a total of 18 articles were included in our study, of which 10 were specific for impedance [35,36,37,38,39,40,41,42,43,44] and 8 for ECoG [29, 45,46,47,48,49,50,51] (Fig. 2). This provided details of 286 different patients, 216 of whom had impedance monitoring and 70 of whom had intraoperative ECoG. No study exploring measurement of impedance and electrical signature using a single device (i.e. ECoG) was identified. Regarding design, all research was conducted as small-scale prospective experimental feasibility studies.
Fig. 2
PRISMA systematic review flowchart of screening
Risk of bias assessmentRisk of bias analysis results are available in full in Fig. 3, with 11 studies scoring as “high risk”, 7 studies presenting “some concerns” and no studies being of “critical” or “low risk”. Although all study designs were prospective and some had pre-registered protocols available, this is a relatively small field of research without established best practices.
Fig. 3
Detailed Risk of Bias (RoB) analysis results using the ROBINS-I tool. This graph was created using the robvis tool
Impedance resultsThe patient and tumour characteristics can be seen in Table 2. In general, study aims were to investigate the feasibility of in-vivo measurement of impedance during brain surgery and to assess whether there is a difference between the electrical impedance of brain tumours and apparent healthy tissue. Where reported, ages ranged from 18 to 88 years and there were more males (n = 63, 57.8%) than females. Additionally, there was a similar distribution of tumours located in either the left or right hemisphere (9 in the left and 6 in the right). Reported pathologies studied included intra- (n = 150, 70.0%) and extra-axial (n = 31, 14.5%) brain tumours and CNS metastases (n = 33, 15.5%). Most of the WHO grades of tumours corresponded to high grade gliomas (HGG) (n = 64, 67.3% grades III-IV). No further information on the molecular profile of lesions was available.
Table 2 Impedance monitoring study and patient characteristicsSix studies opted for a transcranial approach [35, 36, 38, 40,41,42], while the remaining four conducted a stereotactic operation [37, 39, 43, 44]. Of note, four studies reported continuous monitoring as the probe was transversing different tissues [38, 39, 43, 44] while the rest reported single point measurements either before or after the tumour resection [35,36,37, 40,41,42]. No impedance studies reported on their anaesthetic regimens, or whether these were changed compared to standard practice.
The choice between type of probe varied, with six studies using a monopolar, three studies using a bipolar and one study using a custom-made 3 electrode probe (Table 3). Where reported, the location of the probe was confirmed intra-operatively in three studies either via imaging (CT/MRI) or 5-ALA enhancement [35, 39, 44]. Furthermore, three studies compared impedance measurements with imaging or biopsy findings [37,38,39]. Where reported, the electrode tip lengths were 2–5 mm [36,37,38,39, 41, 42, 44], with their diameters ranging from 1–3 mm [35, 37,38,39, 41, 42, 44] and only one study reported the inter-tip distance, which was 5 mm [35]. The materials of the electrodes used were mostly steel [35,36,37,38, 43] or platinum iridium [40].
Table 3 Impedance monitoring resultsThe current signal and frequencies applied varied across studies. For example, Organ et al. applied a current of 0.1 μΑ at a frequency of 100 Hz [43], Abboud et al. injected 0.7 μΑ at 140 Hz [35], Go et al. used 1 μΑ at 10 kHz [38], both studies by Latikka et al. operated with 2 μΑ at 50 kHz [41, 42] and Becker et al. injected currents at 20 mA [36]. The low currents used are in line with the use of small surface area of the probes. Lastly, five studies reported calibration of the probe before measurements were obtained [35, 36, 40,41,42].
Key results from impedance monitoring studies are highlighted in Table 3. The average total number of recordings of the healthy WM was 25, for healthy cortical tissue this was 27 and 45 for pathologic tissues. Only one study measured the impedance of associated oedema and necrotic areas [35] and three measured the impedance of peri-tumoural areas, obtaining an average of 21 measurements. Where reported, characterisation of tissue was based on intra-operative MRI-based neuronavigation with or without 5-ALA enhancement [35, 39], CT [35, 37, 39, 44] or intraoperative histology [37, 38].
Impedance measurements were reported either as Ohms (Ω) which is a direct measure of impedance in seven studies [36,37,38,39,40, 43, 44] or Ohm meters (Ωm), which refers to the resistivity of tissue (does not account for resistance and reactance), in three studies [35, 41, 42]. Individual means reported by each study can be seen in Table 3. A pooled mean impedance of tissues was calculated based on the IPD of six studies [36,37,38, 40, 43, 44]. This was calculated to be 574.31 ± 308.62 Ω in white matter (WM) and that of grey matter (GM) was 604.32 ± 267.94 Ω. The mean impedance of perilesional areas was noted to be 473.55 ± 168.03 Ω and that of lesions was 494.90 ± 330.45 Ω. Statistically significant differences were observed between all tissue types except for between perilesional and lesional tissue (Fig. 4).
Fig. 4
Pooled means of impedance measurements from different tissue types. Tissue from the perilesional area had the lowest impedance followed by lesional tissue, healthy white matter (WM) and lastly, healthy grey matter (GM) [36,37,38, 40, 43, 44]. There was a statistically significant difference between perilesional and healthy WM tissue and between lesional and healthy WM tissue at *p < 0.05. The difference between perilesional and healthy GM tissue was significant at **p < 0.01, and the difference between lesional and healthy GM tissue was significant at ***p < 0.0001 (Mann Whitney U
Comments (0)